Manageing the airway of a trauma patient presents difficulties because of both anatomic and physiologic derangement.
The Bottom Line: Trauma patients requiring intubation are a challenge and should be managed by the most expereinced person in the room. No study shows superiority of direct vs.video laryngoscopy. Use the technique you are most facile with and develop more techniques through courses, mentoring, and expanding your repertoire in less ill patients first. Use induction agents with lower liklelihood of causing hypotension like Etomidate and ketamine (avoid propofol and benzodiazepenes). Avoid hypoxia, hypotension and hypocarbia by resucitating as much as possible prior to intubation (use blood products and pressors where appropriate). Have a plan, a back up plan, and know when to switch to a surgical airway approach. This ia a low frequency, high risk proceedure. Mentally visualize yourself doing this proceedure regualrly to create a comfort level when it is actually needed.
PEARLS:
1. Blood/Emesis A. Use a double suction set up with one suction placed into the airway near the esophagus and then moved to the left of the mouth with the second used by the intubator to clear their view.
B. If you can't visualize becaue of vomit/emesis it is very likely BVM and super glotic airways are not going to be possible and you will need to move to a surgical (front of neck) airway.
2. Limited Jaw Opening Cervical collars can impede jaw opening. Loosen/open the collar to allow more jaw opening. Studies show that there is limited movement of C-Spine when the intubator uses caution not to flex the neck during intubation meaning the collar does not have to be in place. No study shows diret or video laryngoscopy to be superior.
3. Blunt or penetrating neck injury Highest level of difficulty. Should be most expereienced intubator. Can use an awake intubation technique if you are adept at this method. Go with the airway approach that gives YOU the best first pass success chance. Another situation where BVM or suprglotic airway device may not work and requires surgical airway. May require low tracheostomy approach.
4. Hypoxia Avoiding hypoxia is a must especially in traumatic brain injured patients. Pre-oxygenate and use the airway technique that is going to give you the best first past chance of success.
5. Hypotension: A. Resuscitate with blood products as much as possible before intubation. B. Use induction agents that are the most hemodynamically neutral such as Etomidate or Ketamine (safe in head injury patients!)
6.. Hypocarbia: Congrats on getting the tube! Now slow down your bagging. Hypocarbia leads to increased injury in traumatic brain injured patients.
(Please note the prior version of this pearl was incorrect with respect to the images referenced. This version is corrected.)
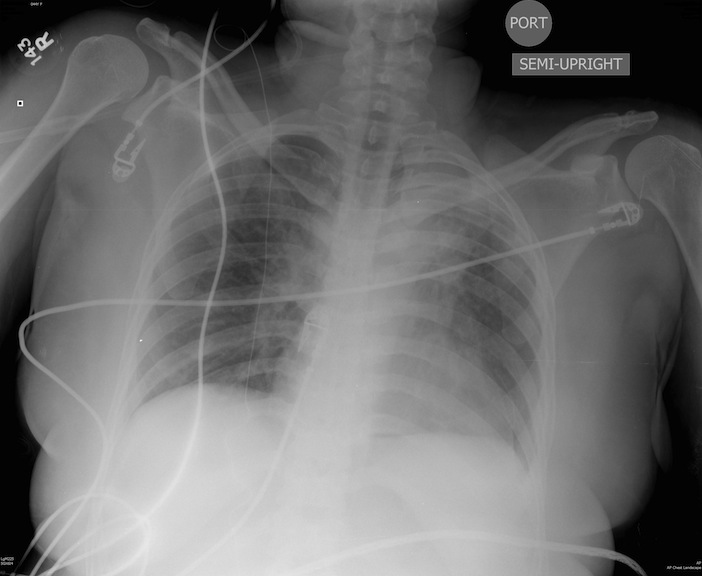
Patient s/p blunt chest trauma. CXR (image 1) vs. lung ultrasound (image 2), do you see any inconsistencies?
44 y/o female restrained driver s/p motor vehicle crash complaining of chest pain and shortness of breath.
Lidocaine with Epinephrine and it use on Fingers and Toes
It has been taught for a long time that Lidocaine with Epinephrine should not be used on fingers, toes, ears and nose [There has to be a kid's song in there somewhere] due to the risk of vasoconstricition/vasospasm and possible digitial infarcation.
The short story is that this practice is not supported by the literature, and there are now numerous publications that have shown that lidocaine with epinephrine is safe for use on the finger tips. It turns out the the original case reports were submitted with procaine and epinephrine and not lidocaine with epinephrine. Most of the cases of digital infarction where with straight procaine that is now thought to have been contaiminated or too acidic pH close to 1 when injected.
The effects of epinephrine last approximately 6 hours. This time is well within the accepted limit of ischemia for fingers that has been established in digitial replanation.
So why use Lidocaine with Epinephrine:
Trauma patients over age 65 should be cared for by a multidisciplinary trauma team. Here is another study affirming that patients over age 65 do worse when having similar injuries to those under 65. Interestingly, those under 65 had more operative repairs of their orthopedic injuries as well.
The authors conclude: “Although the ISS and NISS were similar, mortality was significantly higher among patients aged ≥ 65 years compared to patients < 65 years of age”.
Also it bears further investigation of why those under 65 received more operative repairs
