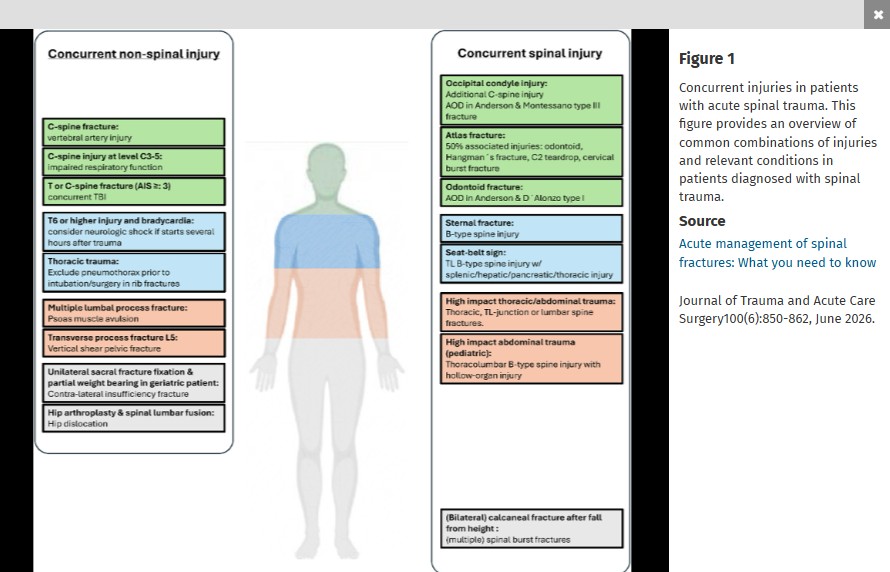
This review article in the Journal of Trauma and Acute Care Surgery states:
“In obtunded patients, an adequate and normal high-quality CT supports collar removal without the need for adjunctive imaging.”
The first step toward developing a healthy ED is to develop a vision of the way emergency medicine should be practiced. The second is to analyze the way it is practiced within a physician group or department. The third is to generate a plan for transitioning from the way it is to the way it ought to be.
A robust department begins with principled physician and nursing leadership.
- Laura Pimentel, The Healthy Emergency Department, in Croskerry P, Cosby KS, Schenkel SM, Wears RL (editors), Patient Safety in Emergency Medicine, Wolters Kluwer, Philadelphia, PA, 2009; 41-44.
A mentor, a colleague, a leader, and a friend, Dr. Laura Pimentel died on June 23, 2026. She led the Emergency Departments at Bon Secours (1993-94), Mercy Medical Center (1995-2007), and Upper Chesapeake Medical Center (2007-08). She was Vice President and then CEO of the Maryland Emergency Medicine Network and, from 2011-2013, President of Maryland ACEP. She will be greatly missed. Her legacy of caring and clarity live on.
Taking a slight detour into the trauma critical care realm today…
BLUF: Favor aggressive calcium supplementation following trauma, especially when patient requires transfusion. Recent evidence is pointing towards a signal for improved outcomes.
Hypocalcemia in trauma is common. Roughly half to two-thirds of trauma patients are hypocalcemic on arrival, driven by both shock physiology and citrate chelation from blood products. Some authors advocate for hypocalcemia to be added as the fourth element of a "lethal diamond" alongside coagulopathy, acidosis, and hypothermia. See reference 1&2 for good discussions of this physiology.
Time for a grain of salt: A recent article in JTACS advocates for favoring calcium chloride during whole-blood or massive transfusion and was associated with improved early survival. Calcium chloride at a threshold of at least 1 g per 2 units of low-titer O whole blood was independently associated with an 84% (!) reduction in 24-hour mortality, with the benefit strongest at this 1:2 ratio and weaker at less aggressive thresholds. (LOTS of caveats with this finding, but interesting nonetheless).
Current major civilian guidelines say only that hypocalcemia should be prevented, with limited specificity on timing or dose, and the Joint Trauma System recommends 1 g calcium after the first unit and after every fourth unit thereafter. The current CAVALIER trial is evaluating prehospital calcium specifically. Those results and other recent literature could push major trauma organizations to update their recommendations in the near future.
Bottom Line: Among hospitalized patients boarding in the emergency department, care at an academic safety-net hospital, overnight admission, and elevated lactate levels may be independent predictors of early clinical deterioration.
In a randomized multicenter trial comparing direct vs video laryngoscopy in trauma patient intubation, video had a higher first pass success rate and equal complication to direct laryngoscopy.
This study found that of all 283 EM residencies in the US, only 4% listed pronouns on resident webpages, 3% had LGBT+ dedicated sections of their website, and only 31% had DEI sections of the website at all.
In the post COVID era of residency interviews, the programs' websites become a vital source of information for the applicants. There is still a large gap in the visibility of the LGBTQIA+ population in the majority of program websites.
This was a metanalysis which included 5 studies of 3933 pediatric patients requiring seizure management without IV access, mostly in the prehospital setting.
Bottom line: IM midazolam appears superior to IN midazolam as a first-line non-IV benzodiazepine for pediatric seizures in the prehospital setting, though IN remains a clinically effective alternative — particularly when caregiver acceptability and ease of administration are prioritized.
This single center prospective study asked residents to determine if their patient had barriers to post ED discharge health care such as having a PCP, transportation issues, affording medications, and need for assistance with activities of daily living. They then compared the physicians’ answers to patient’s answers and found: “Physicians had poor sensitivity for accurate identification of patient barriers.”
Some of our discharged patients are struggling more than we realize.
This was a retrospective study of the pediatric cardiac arrests over a 5 year period (including COVID years) in Vienna.
Infants (<1 year) had the highest incidence of OHCA among all pediatric age groups, consistent with German registry data showing an incidence of 23.4 per 100,000 in this age group.
Non-shockable rhythms (asystole/PEA) predominated, as expected given that most pediatric OHCA results from progressive respiratory failure or shock rather than primary cardiac causes.
Survival to hospital discharge remained low, consistent with international data showing pediatric OHCA survival ranging from 6.6% for infants to 17.3% for adolescents in the US CARES registry.
Bystander CPR rates and witnessed arrest status were important modifiable factors associated with improved outcomes, aligning with findings from the adult Vienna cohort where witnessed arrests with shockable rhythms had substantially higher survival (39% vs. 9.3% overall).
The study highlighted that even in a high-resource, physician-staffed EMS system, pediatric OHCA outcomes remain poor, underscoring the importance of primary prevention and early bystander intervention
There were a handful of big name critical care studies published the last few weeks (LOGICAL, ARISE FLUIDS, SODa-BIC to name a few) but many of you probably already saw those so we're gonna stick with something a little more off the beaten path.
A retrospective observation trial was published recently by Gastanadui et al in Journal of Intensive Care looking at the mortality impact of corticosteroids in cardiogenic shock. They looked at 167,721 patients from the Vizient database admitted with cardiogenic shock (excluded patients with other indications for steroids). The unadjusted mortality was a whopping 48.8% in the steroid group and 29.6% in the non-steroid group. They did Inverse Probability Treatment Weighting (IPTW), which attempts (imperfectly, but best as you can retrospectively) to control for treatment selection bias, and still found a roughly 3% mortality increase in the steroid group.
Bottom Line: Corticosteroids were already controversial (at best) in cardiogenic shock, but this further adds to the reasons to avoid them in this condition. Of note, this trial excluded patients with classic hard-indications (e.g. adrenal insufficiency, COPD exacerbation, etc) and steroids should still be given to those groups, but in my opinion if you feel cardiogenic is the primary driver of the patient's shock and they do not have another indication, I would consider avoiding steroids solely for the shock.
This multicenter study looked at trauma patients with a hemothorax who underwent early tube thoracostomy vs. being observed. They found volume of over 300 ml predicted observation failure. Those observed had shorter hospital stays and less ICU admissions. Twenty two percent of observation patients required tube thoracostomy. The failed observation group had similar outcomes except longer hospital stays.
Bottom Line: Lactate is a useful but imperfect marker of critical illness. Below are some key points to consider when interpreting lactate.
Bottom Line: In pediatric patients, identifying the underlying etiology of hypercalcemia is essential to guide appropriate long-term management.
Etiology: The causes of hypercalcemia in children are diverse and are broadly classified into parathyroid hormone (PTH)-mediated and non–PTH-mediated categories. Non–PTH-mediated causes include endocrine disorders, inborn errors of metabolism, medication-induced hypercalcemia, granulomatous diseases, immobilization, and malignancy.
Clinical Presentation: Symptoms vary depending on the severity of hypercalcemia. Mild hypercalcemia may be asymptomatic or present with findings such as shortened QT interval, polyuria, and constipation. Severe hypercalcemia can lead to significant complications, including seizures, altered mental status (e.g., hallucinations), dehydration, cardiac dysrhythmias, abdominal pain, and pancreatitis.
Management: In the emergency setting, the primary treatment is intravenous hydration, typically with 0.9% saline, to cause calcium dilution and increased urinary excretion of calcium. Loop diuretics should be used with caution in pediatric patients due to the risk of exacerbating dehydration. Additional pharmacologic therapies, including calcitonin, bisphosphonates, and glucocorticoids, may be indicated depending on the etiology and severity, and should be administered in consultation with a nephrologist and/or endocrinologist. In patients with contraindications to aggressive fluid management (e.g., renal or cardiac dysfunction), or in cases of severe, life-threatening hypercalcemia, dialysis may be required.
When managing suspected or proven Group A Streptococcus (GAS) Necrotizing Soft Tissue Infections (NSTIs), standard beta-lactams can lose efficacy due to the Eagle effect—where stationary-growth phase bacteria become less susceptible to cell-wall acting agents.
To counteract this and aggressively suppress life-threatening bacterial toxin production, always add a protein-synthesis inhibiting antibiotic to your empirical broad-spectrum base.
Expert consensus recommends not prescribing these eight classes of medications to older adults mostly due to sedative affect and fall risk. 1. Benzodiazepines 2. Barbiturates 3. Muscle relaxants 4. 1st generation antihistamines 5. Sulfanylureas 6. 1st generation antipsychotics 7. Zolpidem 8. Metocloprimide
A recent study shows marginal improvement in not prescribing these medications to older ED patients.
This single center study looked at diabetic patients who had a POC glucose over 300 and POC ketone over 1.1 and reviewed their diagnosis vs the laboratory accepted diagnosis of DKA.
“The most recent international consensus laboratory definition of (non-euglycemic) DKA includes a glucose of >?250; a pH <?7.3 or a bicarbonate ??18?mmol/L; and a beta-hydroxybutyrate (BOHB) ??3.0?mmol/L or urine ketone strip ??2+”
This nice review article reminds us “The AO-Spine classification is the most frequently utilized system for thoracic and lumbar fractures, and it categorizes fractures into three types. Type A fractures are compression injuries. In these fractures, the assessment of the involvement of the posterior elements of the vertebral body is essential. Type B fractures are distraction injuries implying tension band involvement, whereas type C fractures are translational or dislocated injuries. The AO-Spine Upper Cervical Injury Classification System… In this classification system, type A injuries have no ligamentous involvement and are considered stable. Type B injuries have tension band or ligamentous injury and may be unstable. Type C injuries are characterized by significant translation and loss of anatomic integrity and are considered unstable."
A 22 year old normally healthy male presents with tachycardia (HR 140), dilated pupils (7 mm), dry flushed hot skin, and confusion/agitation. His mother states he has a 1 day history of “talking out of his head not making sense”, “seeing things that aren’t there”, and “speaking to video game characters”. He has suprapubic tenderness with markedly distended bladder on exam revealing over 1 liter of urine on bladder scan. She found a small bottle containing a large amount of small 2-3 mm black seeds in his room and suspects he ingested them. What treatment options would you consider?

Do you have a patient with shortness of breath and pulmonary edema?
Don’t forget to place the color doppler over the mitral valve to look for acute mitral regurgitation.
{kind=link}