-- CSF reforms within 6 hours, making its removal short-term, unless there is a CSF leak.
-- LP can be challenging in obese patients and uncomfortable for patients, in general.
-- LP complications such as low pressure headaches, CSF leak, CSF infection, and intraspinal epidermoid tumors.
Optimal management of subarachnoid hemorrhage requires prognostic understanding and effective communication with neurology and neurosurgical consultants, as well as the patient and their family members.
It is therefore often helpful to utilize and reference the widely recognized Hunt and Hess Scale in grading symptoms of ruptured cerebral aneurysm and subarachnoid hemorrhage severity:
For your convenience, an online Hunt and Hess Scale calculating tool can be found at:
http://www.mdcalc.com/hunt-and-hess-classification-of-subarachnoid-hemorrhage-sah
Classic Cerebrospinal Fluid Characteristics
--- High NIH Stroke Scale scores.
--- Large areas of infarct.
--- Cerebellar infarcts.
--- Extended time to tPA administration.
--- Previous stroke.
--- Older age.
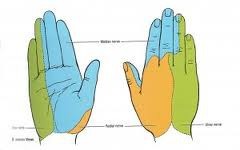
How to Perform a Median Nerve Block
-- ulnar nerve >>> supplies palmar surface and dorsal tips of little finger and medial half of ring finger, including
adjacent parts of hand.
-- median nerve >>> supplies palmar and dorsal aspects of thumb, index finger, middle finger, and lateral half
of ring finger, including adjacent parts of hand.
-- radial nerve >>> supplies most of dorsal surface of hand.
Consider the diagnosis of a Cervicogenic Headache when the following findings are present:
A. Pain localized to the neck and occipital region, potentially with projection to forehead, orbits, temples, vertex or ears.
B. Pain is precipitated or aggravated by particular neck movements or sustained postures.
C . At least one of the following:
1. Resistance to or limitation of passive neck movements.
2. Changes in neck muscle contour, texture, tone or response to active and passive stretching and contraction.
3. Abnormal tenderness of neck muscles.
D. Radiological imaging reveals at least one of the following:
1. Movement abnormalities in flexion/extension.
2. Abnormal posture.
3. Fractures, congenital abnormalities, bone tumors, rheumatoid arthritis or other distinct pathology (not spondylosis or osteochondrosis).
Cluster headaches are defined as a group of at least five headache attacks causing unilateral orbital, supraorbital and/or temporal pain, with at least one of the following simultaneous associated findings on the affected side:
Cluster headaches can occur at a frequency of one every other day t eight episodes per day.
A. At least two attacks with at least 3 of the following:
1. One or more fully reversible aura symptoms (indicates focal cerebral cortical and/or brain stem functions).
2. At least 1 aura symptom develops gradually over greater than 4 minutes, or 2 or more symptoms occur in succession.
3. No aura symptom lasts greater than 60 minutes.
4. Headache follows aura with free interval of at least 60 minutes.
B. At least 1 of the following aura features establishes a diagnosis of migraine with typical aura:
1. Homonymous visual disturbance.
2. Unilateral paresthesias and/or numbness.
3. Unilateral weakness.
4. Aphasia or speech difficulty.
A.
1. Pulsatile or throbbing in quality
2. Unilateral in location
3. Moderate to severe in intensity
4. Aggravated by activity (i.e.climbing stairs, exertion), plus
B. at least 1 of the following 2 during the headache ("VP"):
1. Vomiting and/or nausea
2. Photophobia and/or phonophobia