Excessive and improper administration of local anesthetic (a.k.a. local anesthetic systemic toxicity or L.A.S.T.) can lead to cardiac toxicity with symptoms ranging from benign arrhythmias to overt cardiac arrest.
Administration of a 20% intra-lipid emulsion has been experimentally known to reverse L.A.S.T in animal models, but in 2006 the first documented human case of ILE was successfully used during cardiac arrest secondary to L.A.S.T. with hemodynamic recovery and good neurologic outcome. Many case reports have emerged since then, including the use of ILE in toxicity with other lipophilic drugs (e.g., calcium channel blockers, tricyclic antidepressants, etc.)
Several mechanisms have been proposed explaining how ILE works. They include:
Dosing of ILE:
Check out this video by our own Dr. Bryan Hayes(@PharmERToxGuy) and Lipidrescue.org for more information.
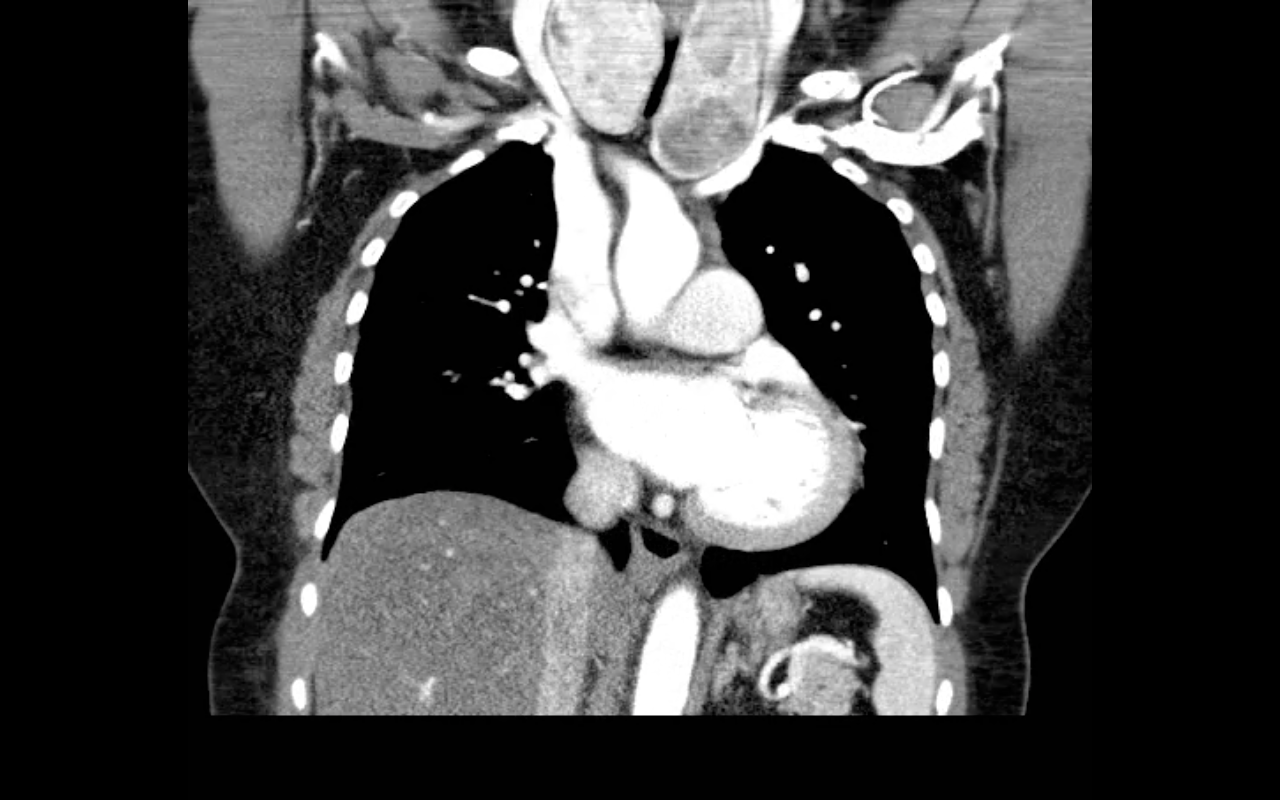
68 year-old female presents with stridor and palpable goiter. Here's a clip from CT of the chest. What's the diagnosis?
Propofol is generally a well-tolerated sedative / amnestic but occasionally it can lead to the propofol infusion syndrome (PRIS); a metabolic disorder causing end-organ dysfunction.
Suspect PRIS in patients with increasing lactate levels, worsening metabolic acidosis, worsening renal function, increased triglyceride levels, or creatinine kinase levels. End-organ effects include:
The true incidence of PRIS is unknown, however, certain risk factors have been identified:
Prevent PRIS by using adequate analgesia (with morphine or fentanyl) post-intubation, which may reduce the overall dosage of propofol ultimately reducing the risk.
If PRIS develops, stop propofol and provide supportive care; IV fluids, ensuring good urine output, adequate oxygenation, dialysis (if indicated), vasopressor and inotropic support.
A 25 year-old female presents complaining of a "net-like" rash bilaterally on her medial thighs. She denies any pain but states that the rash looks “pretty scary” What's the diagnosis?

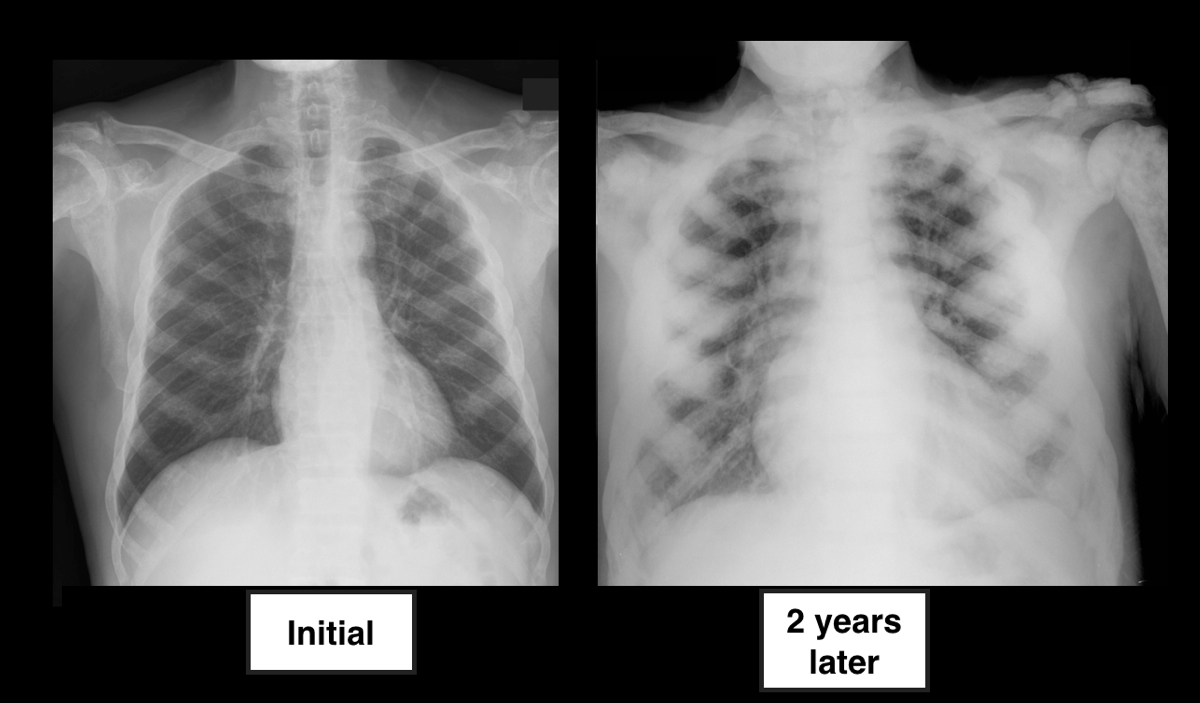
40 year-old male presents with fever, chills, & cough. What’s the diagnosis and the MOST likely cause?
The updated Surviving Sepsis Guidelines have been released (click here) and here are some recommendations as they pertain to hemodynamic management (grades of recommendations in parenthesis).
Fluid therapy
Vasopressors (targeting MAP of at least 65 mmHg)
Corticosteroids
Inotropic Therapy
40 year-old female drove into a ditch. Right sided chest pain and stable vitals. Here's the CT but what do you think the initial CXR showed (Hint: it's a trick)?
45 year-old male complains of chest pain and cough. He also tells you, "...oh, and by the way doc, I just smoked something." What's the diagnosis?
Intra-aortic balloon pumps (IABP) are devices that provide hemodynamic support during cardiogenic shock; the balloon inflates during diastole (improving coronary artery perfusion) and deflates during systole (reducing afterload and improving systemic perfusion). Click here to see a 41 second video illustrating how it works.
Several guidelines recommend placement of an IABP for patients in cardiogenic shock secondary to acute myocardial infarction (AMI), if early revascularization (e.g., CABG) is planned (Class I recommendation). Data behind this recommendation, however, is limited.
The IABP-SHOCK II trial was a randomized, multi-center, open-label study that enrolled 600 patients (598 in the analysis) with cardiogenic shock secondary to AMI (STEMI or NSTEMI). Patients were randomized to the control group (receiving standard therapy; N=298) or the experimental group (receiving IABP; N=300).
No significant difference was found between groups with respect to 30-day mortality (primary end-point), secondary end-points (e.g., time to hemodynamic stabilization, renal function, lactate levels, etc.), or complications (e.g., major bleeding, peripheral ischemic complications, etc.).
Bottom line: Perhaps it is time to reassess the approach to cardiogenic shock secondary to AMI when early revascularization is planned. At this time consultation with local expertise is recommended.
4 year-old female with the post-procedural CXR shown below. What's the diagnosis? (Hint: use the zoom...this one is tricky)
DRESS (Drug Reaction with Eosinophilia and Systemic Symptoms) or DIHS (Drug-Induced Hypersensitivity Syndrome) is a potentially life-threatening adverse drug-reaction.
Incidence is 1/1,000 to 1/10,00 drug exposures. It occurs 2-6 weeks after the drug is first introduced, distinguishing it from other adverse drug-reactions which typically occur sooner.
The syndrome classically includes:
The most commonly implicated drugs are anticonvulsants (e.g., carbamazepine, phenobarbital, and phenytoin), sulfonamides, and allopurinol.
Recovery is typically complete after discontinuing the offending drug; systemic steroids may promote resolution of the illness.
31 year-old male with recently diagnosed hypertension presents with rapid lip swelling. He started taking an unknown medication for his hypertension last week. Further history reveals that he has had prior, although milder, episodes previously. Name two medications that may help treat him.

52 year-old male with diabetes complains of severe left foot pain for one month and now inability to ambulate. Vital signs are normal and X-rays are shown below. What's the diagnosis and why should you get a biopsy early?

Management of patients with severe traumatic brain injury (TBI) typically involves the use of invasive intra-parenchymal pressure monitors. Although use of these monitors is recommended by TBI management guidelines, good quality evidence of benefit is lacking.
A recently published study evaluated the outcomes of TBI patients using a management protocol incorporating either an intracranial pressure (ICP) monitor compared to use of the clinical exam PLUS serial neuroimaging; a total of 324 patients were prospectively randomized into either group.
The primary study outcome was a composite of survival, impaired consciousness, and functional status at both three and six months.
The results of the study did not show a significant difference in the:
Bottom line: This study suggests that clinical exam PLUS serial neuroimaging may perform as well as invasive intra-parenchymal monitors for guiding therapy in TBI patients.
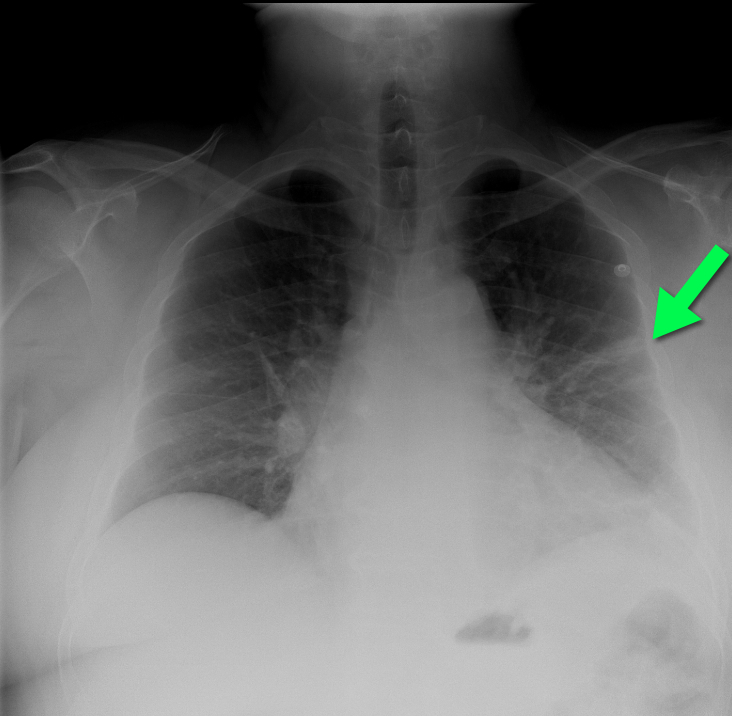
50 year-old man with presents with acute-onset sharp left-sided chest pain and dyspnea. What's the diagnosis and the name of the abnormality on chest x-ray?
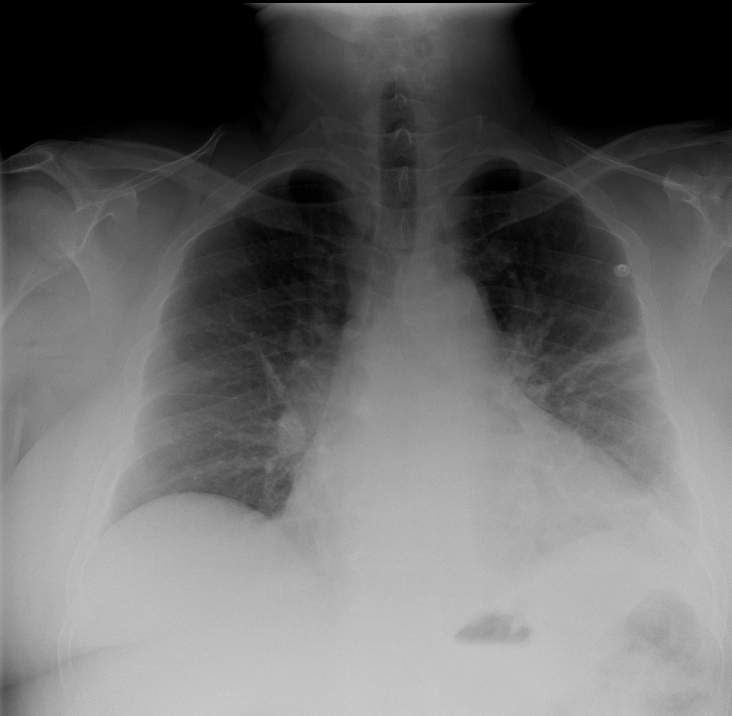
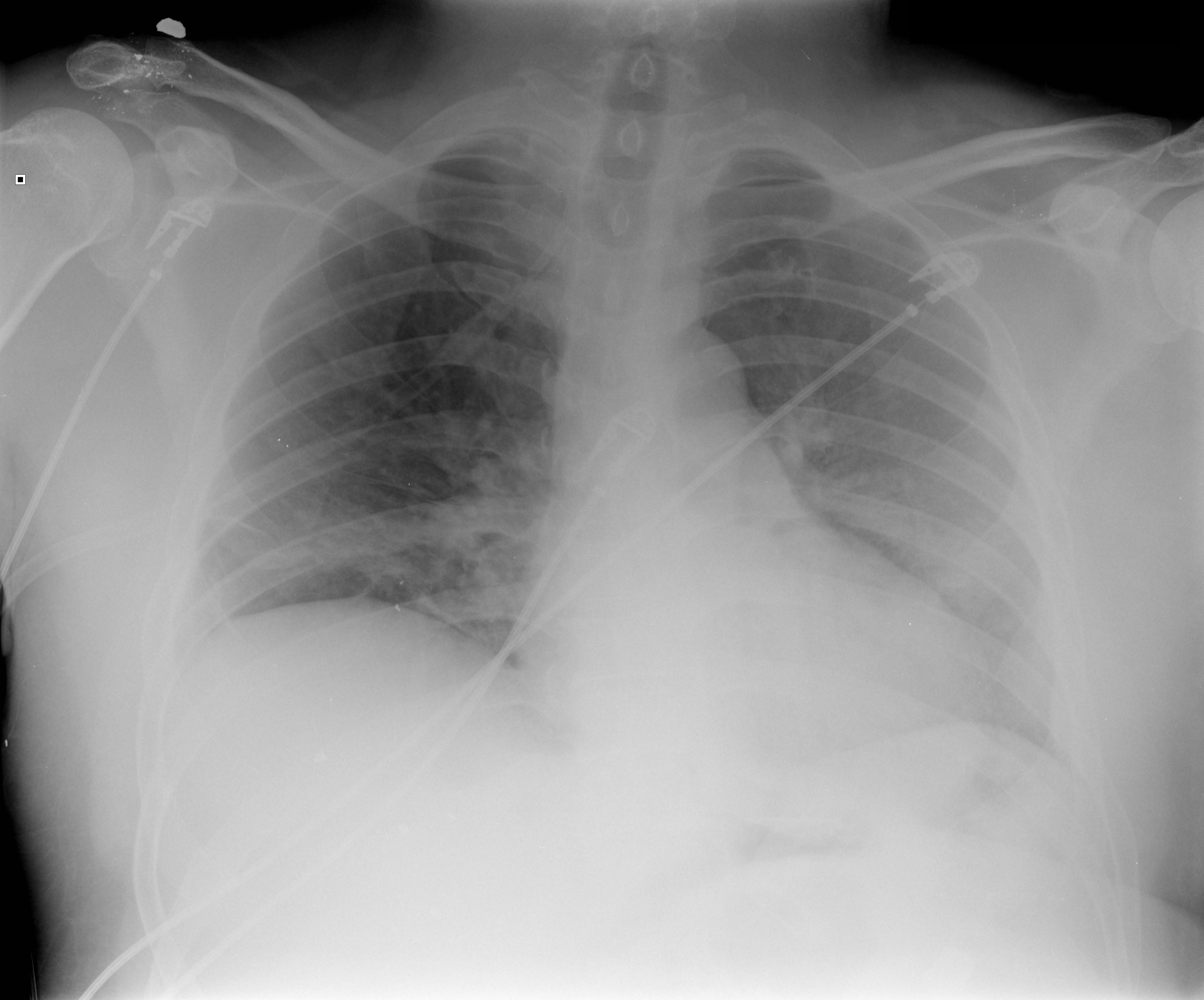
64 year-old male with no past medical history presents complaining of chronic weight-loss and diffuse chest pain; CXR is shown below. What's the diagnosis, and what other disease(s) may present this way?

An 86 year-old nursing home resident presents to the ED with a urinary tract infection, four days after discharge from the inpatient service for the same diagnosis. She was discharged from the inpatient service with a prescription for ciprofloxacin to be given through her gastric feeding tube (she does not take anything orally). Could her tube feeds be playing a role in the relapse of her urinary tract infection?
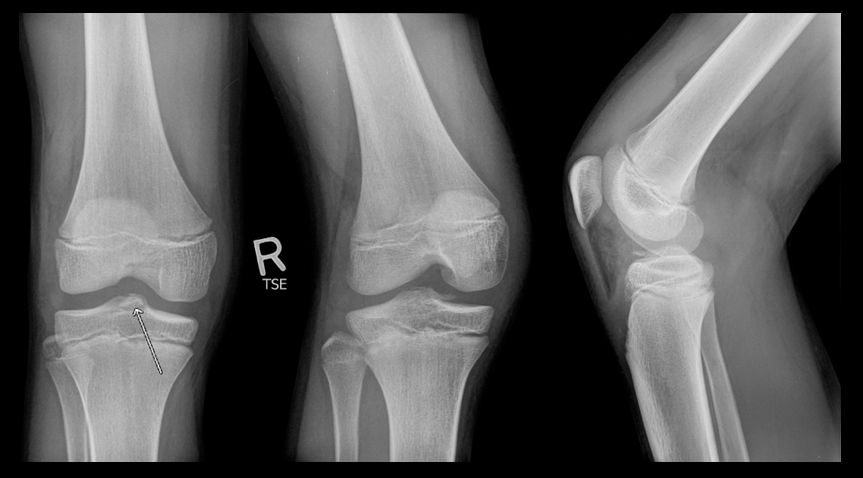
11 year-old boy presents with right knee pain and swelling after falling off of his bicycle. What's the diagnosis?
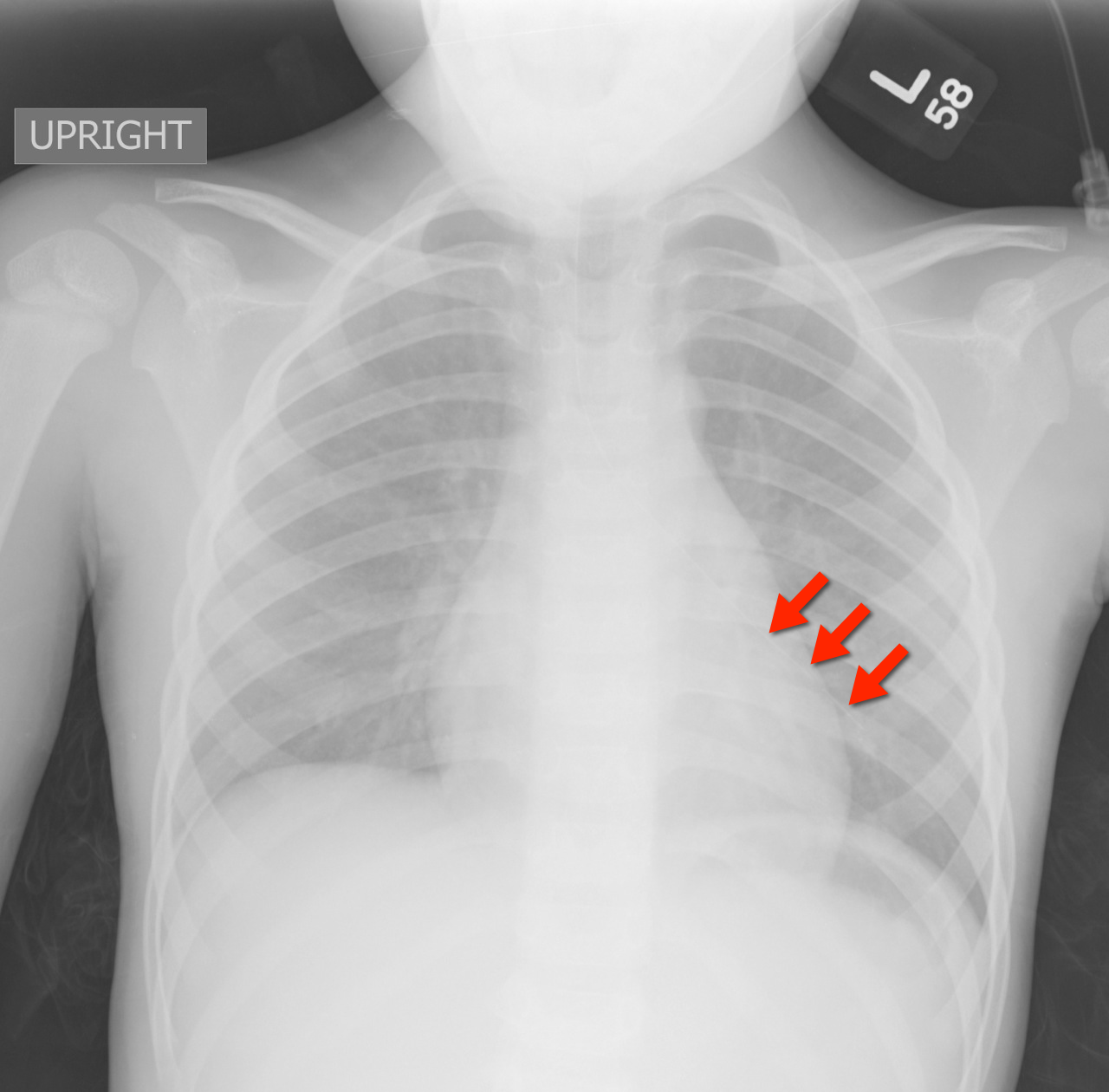
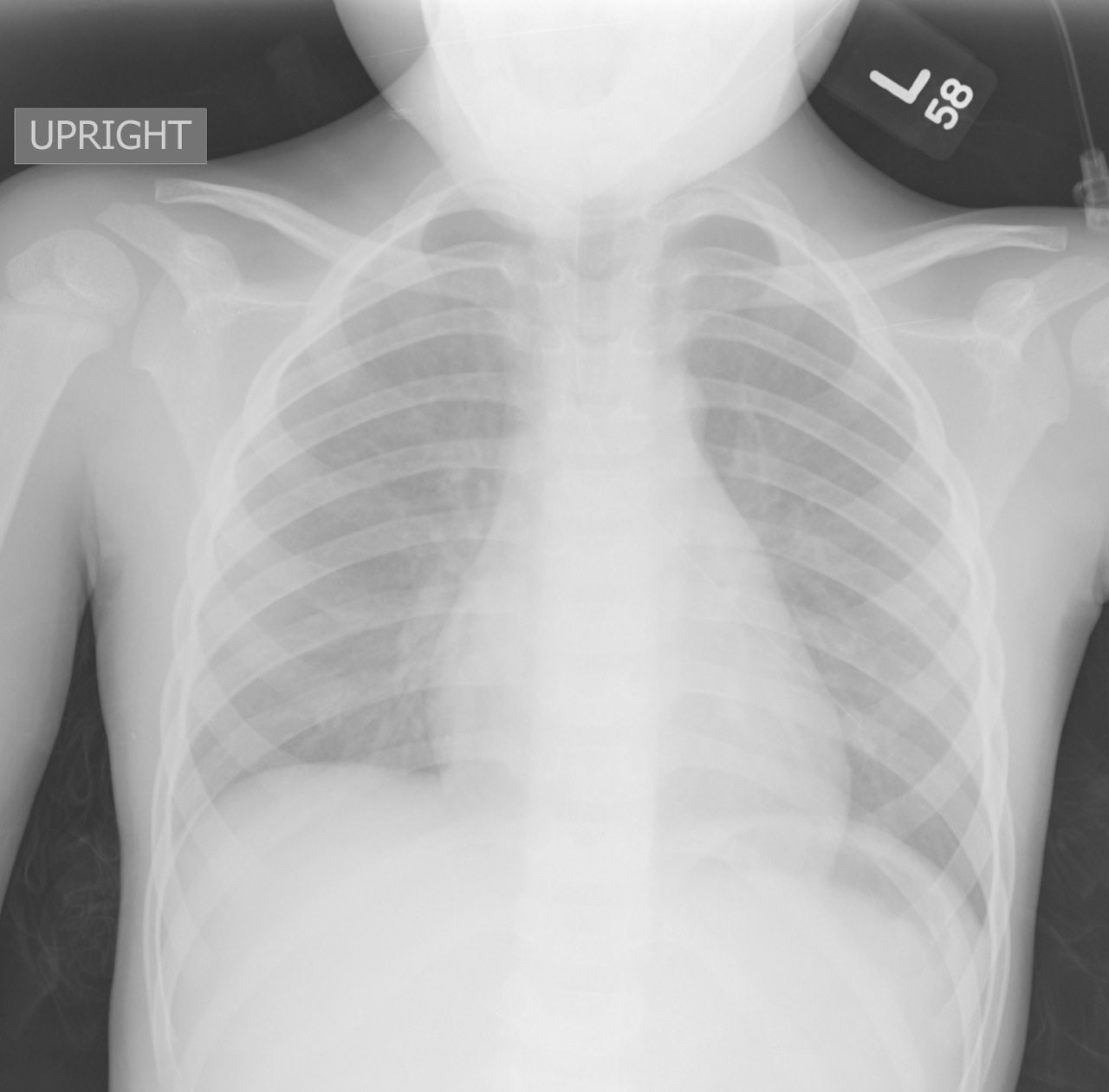
2 year-old male with past medical history of asthma presents with fever and respiratory distress. CXR is shown below. What’s the diagnosis? (Hint: ...look beyond the obvious)

A low-tidal volume (or protective) strategy of mechanical ventilation (i.e., tidal volume of 6-8cc/kg of ideal body weight) has previously been demonstrated to be beneficial in patients with acute respiratory distress syndrome (ARDS).
A meta-analysis was recently performed to determine whether this strategy of mechanical ventilation is also beneficial for patients without lung injury prior to initiation of mechanical ventilation.
Dr. Neto, et al. performed a meta-analysis of 20 studies (total of 2,822 mechanically ventilated patients) comparing a conventional ventilation strategy (average tidal volume was 10.6 cc/kg) to a protective ventilation strategy (average tidal volume was 6.4 cc/kg) of mechanical ventilation.
The authors concluded that patients ventilated with a protective lung-strategy had reductions in:
Bottom-line: This meta-analysis supports the notion that a strategy of low-tidal volume ventilation may have benefits for patients without ARDS, however prospective studies are needed.