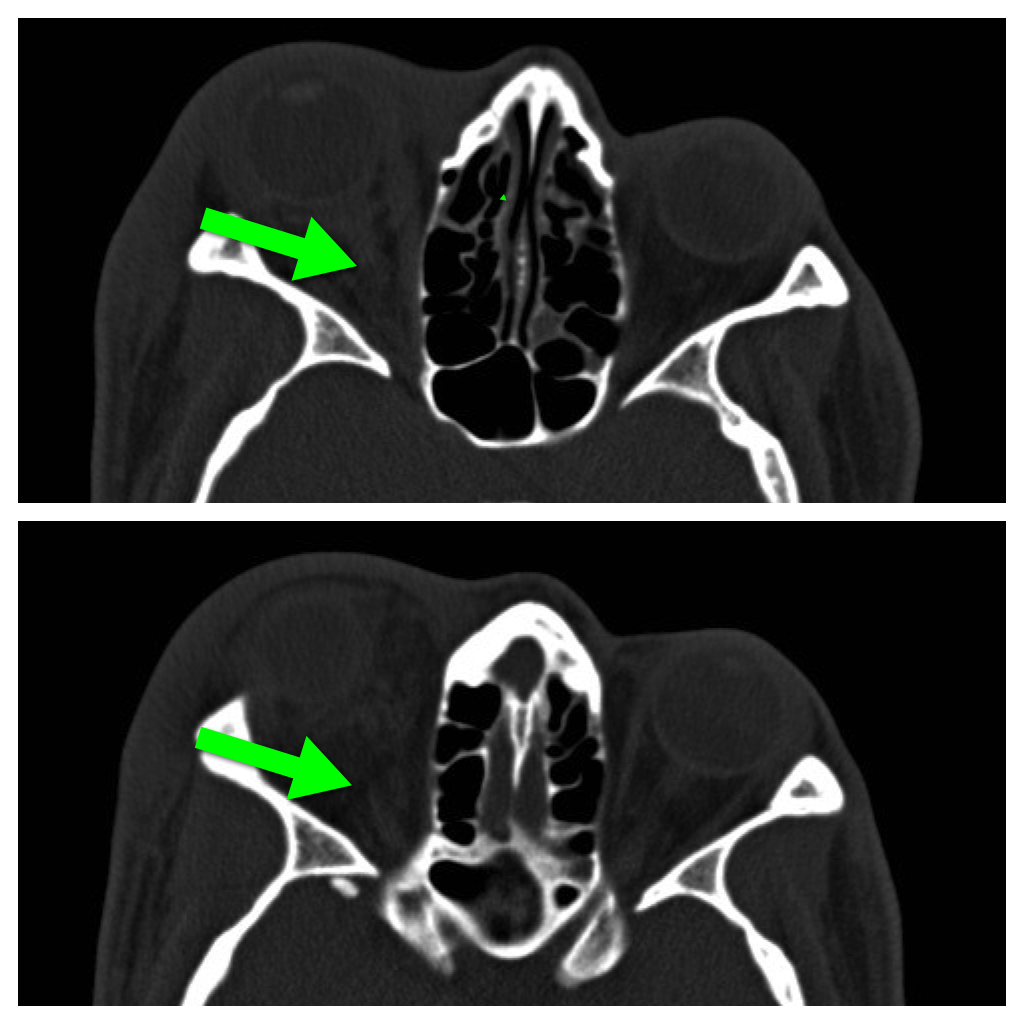
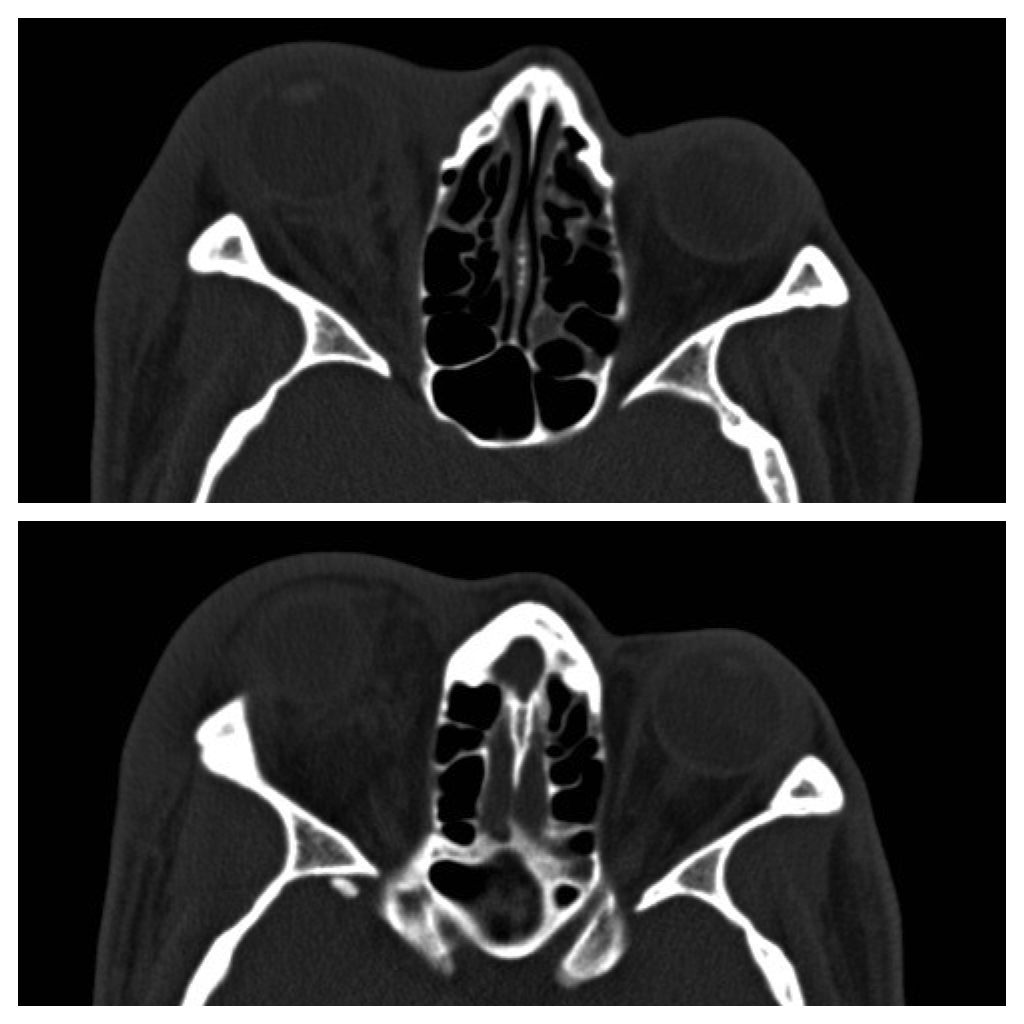
42 year-old male s/p assault complains of right sided facial pain, swelling, and decreased vision. Physical exam reveals subconjunctival hemorrhage, proptosis, afferent pupillary defect, and a firm globe. What's the diagnosis and what's the emergent treatment?
37 year-old male presents after sustaining a burn from a pot of boiling water. He states that his skin started to blister a few hours after and it’s quite painful. What type of burn does he likely have?

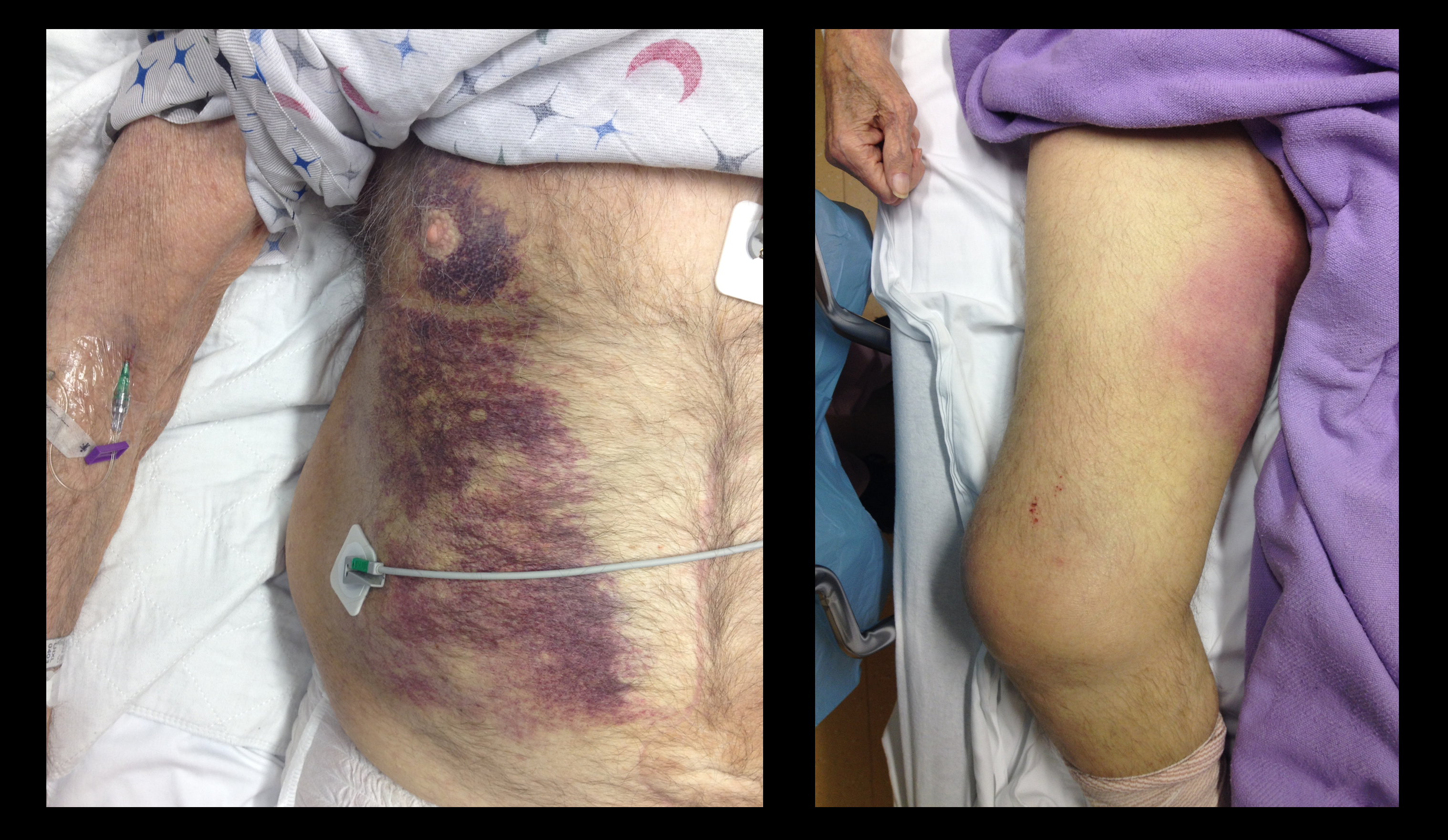
68 year-old male presents with weakness after surgical repair of his abdominal aorta. What’s the diagnosis and name at least one eponym for the signs displayed (there are five total)?
The morbidity and mortality from pseudomonas aeruginosa infections is high and empiric double-antibiotic coverage (DAC) is sometimes given; quality evidence for this practice is lacking.
Although there is little supporting data, the following reasons have been given for DAC:
The potential harm of antibiotic overuse cannot be ignored, however, and include adverse reaction, microbial resistance, risk of super-infection with other organisms (e.g., Clostridium difficile), and cost.
There may be a signal in the literature demonstrating a survival benefit when using DAC for patients with shock, hospital-associated pneumonia, or neutropenia. The IDSA guidelines, however, do not support DAC for neutropenia alone; only with neutropenia plus pneumonia or gram-negative bacteremia.
Bottom line: Little data supports the routine use of DAC in presumed pseudomonal infection. It may be considered in patients with shock, hospital-associated pneumonia, or neutropenia (+/- pneumonia), but consult your hospital’s antibiogram or ID consultant for local practices.
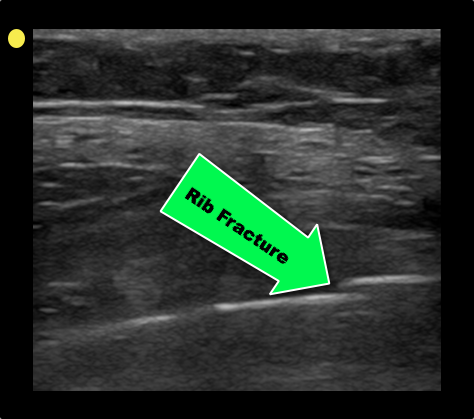
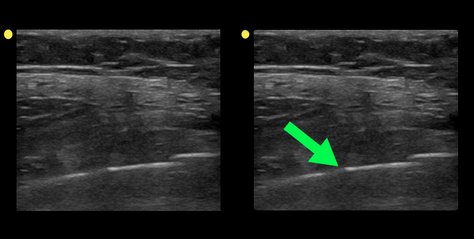
Patient with a history of osteogenesis imperfecta presents with right lateral chest pain following a sneeze. The ultrasound of his chest is shown (hint: arrow points to a rib). What's the diagnosis?
46 year-old female found unresponsive at a party. EMS transports the patient in cardiac arrest. A parasternal-long axis view of the heart is obtained during the pulse check. What's the diagnosis?
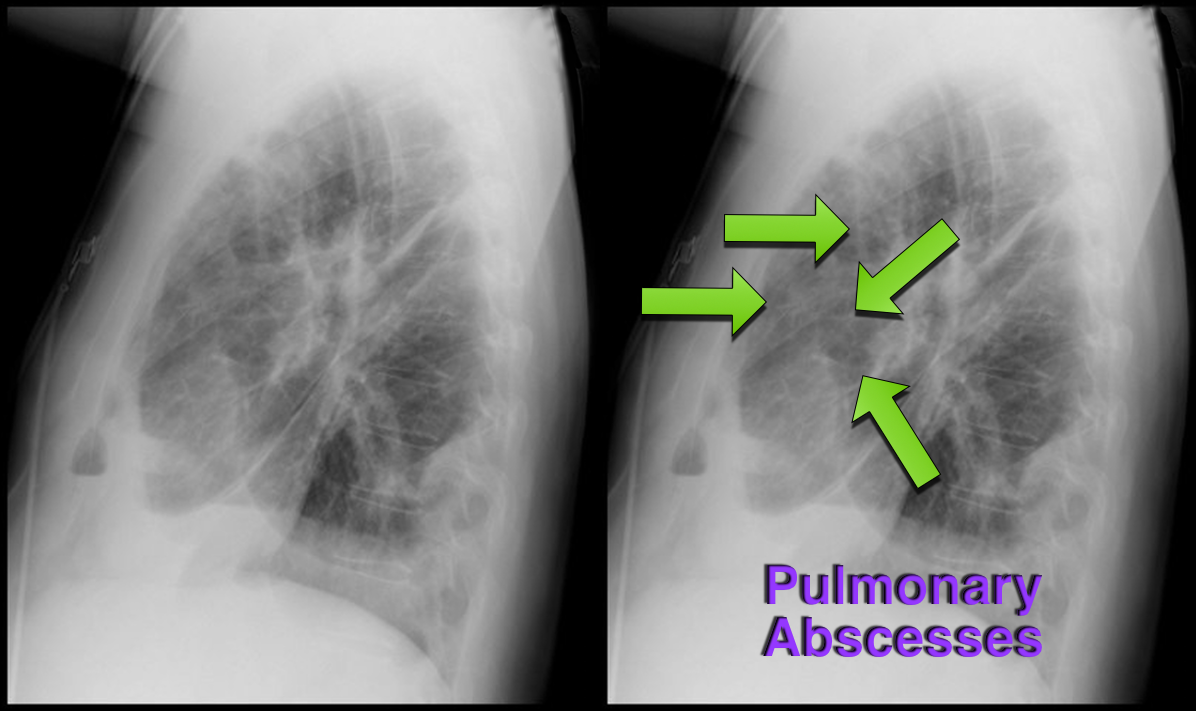
37 year-old male presents with cough and a fever. What's the diagnosis and name three risk factors assiciated with disease?

Which view of the heart is this and can you name the structures from A-G?
The management of alcohol withdrawal syndrome (AWS) includes supportive care focusing on the ABC’s and administration of benzodiazepines (BDZ).
While BDZ are effective in the treatment of AWS, some patients may require very high doses of BDZ to control symptoms (tachycardia, hypertension, diaphoresis, etc.); unfortunately, high-doses of BDZ may lead to suppression of the respiratory drive and endotracheal intubation.
Dexmedetomidine (DEX) is a sedative agent that is an intravenous alpha2-agonist (it's like clonidine); it reduces sympathetic outflow from the central nervous system and it may help treat withdrawal syndromes. The major benefit of DEX is that it does not suppress the respiratory drive, thus intubation is not required.
Smaller trials and case series have shown that patients with AWS who were treated with BDZ in addition to DEX had better symptom control, lower overall BDZ doses, and less respiratory depression/intubation.
Bottom-line: While more trials are needed, consider adding DEX for patients with AWS who require high-doses of BDZ.
What view of the heart is this and can you name everything from A-G?
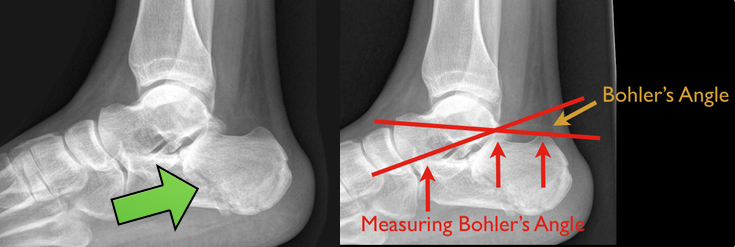
48 year-old presents after falling 15 feet following a “misunderstanding” with police. What's the diagnosis? ...and for a bonus question, why is this called a “Lover’s Fracture”?

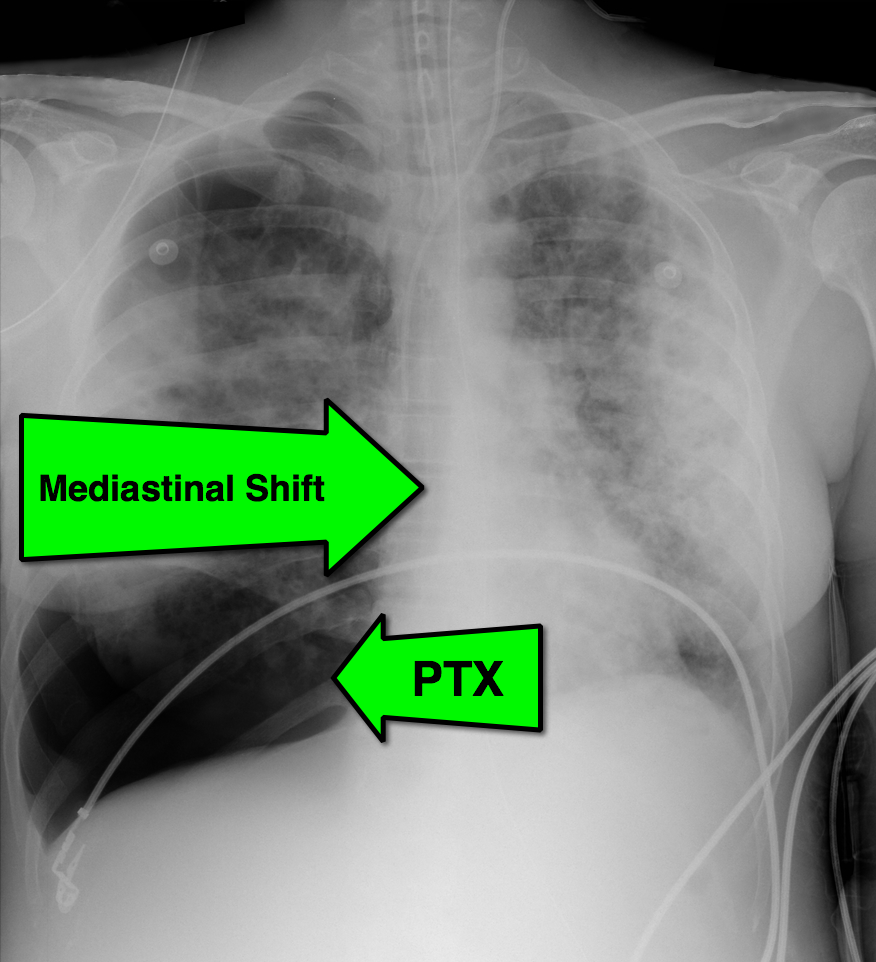
28 year-old cachectic female presents in respiratory distress and is immediately intubated on arrival to Emergency Department. What's the diagnosis and what are some potential etiologies?

This week's visual pearl reviews the structures of the heart when being viewed in a parasternal long-axis view. What do the labels correspond to in the clip below (note: "E" and "F" are valves) and do you see any obvious abnormalities?
The pregnant patient normally has increased cardiac output and minute ventilation by the third trimester. Despite this increase, however, these patients have little cardiopulmonary reserve should they become critically-ill.
Remember the mnemonic T.O.L.D.D. for simple tips that should be done for the pregnant patient who presents critically-ill or with the potential for critical illness:
15 year-old right-hand dominant male received a direct blow to the right arm with a hockey stick. What’s the diagnosis?

55 year-old male presents with chest pain. You take a look at his cardiac function with ultrasound and here's the patient's apical four-chamber view. What's in his right ventricle and why would it be there?
There have been so many great talks at ACEP 2013, but Dr. Michael Winters' talk "The ICU is NOT Ready for Your Patient" was chock full of great critical care pearls. Here are just a few:
A 23 year-old male presents with the rash below. He originally presented to his primary care doctor for a sore throat and was given a prescription for a medication; this rash subsequently broke out. What's the diagnosis and which medication did he receive?

25 year-old female struck in the left hand by a football. Presents with pain, visible deformity, and the Xray below. What are the next step(s) in management?

The efficacy of epinephrine during out-of hospital cardiac arrest has been questioned in recent years, especially with respect to neurologic outcomes (ref#1).
A recent study demonstrated both a survival and neurologic benefit to using epinephrine during in-hospital cardiac arrest when used in combination with vasopressin and methylprednisolone.
Researchers in Greece randomized 268 consecutive patients with in-hospital cardiac arrest to receive either epinephrine + placebo (control group; n=138) or vasopressin, epinephrine, and methylprednisolone (intervention arm; n=130)
Vasopressin (20 IU) was given with epinephrine each CPR cycle for the first 5 cycles; Epinephrine was given alone thereafter (if necessary)
Methylprednisolone (40 mg) was only given during the first CPR cycle.
If there was return of spontaneous circulation (ROSC) but the patient was in shock, 300 mg of methylprednisolone was given daily for up to 7 days.
Primary study end-points were ROSC for 20 minutes or more and survival to hospital discharge while monitoring for neurological outcome
The results were that patients in the intervention group had a statistically significant:
probability of ROSC for > 20 minutes (84% vs. 66%)
survival with good neurological outcomes (14% vs. 5%)
survival if shock was present post-ROSC (21% vs. 8%)
better hemodynamic parameters, less organ dysfunction, and better central venous saturation levels
Bottom-line: This study may present a promising new therapy for in-hospital cardiac arrest and should be strongly considered.