Ever been in an acute rescucitation and found yourself unable to remember all of those famous ACLS Hs and Ts? I know I have. A few years ago Littman et al published an alternative approach to critically ill, hypotensive medical patients with non shockable rhythms. Unfortunately, it seems like some of the enthusiasm for this approach has died down, but I still think it's something you're more likely to recall in a pinch than the Hs and Ts and is a better way of getting started with a hypotensive non-trauma patient. And it's so simple you may actually remember it!
1) Look at the monitor. Is the rhythm narrow or wide?
2a) Narrow - more likely a mechanical problem (tamponade, tension PTX, autoPEEP, or PE). Give IVF and search for one of these causes (and correct it!). Keep in mind that ultrasound can help you differentiate a lot of these.
2b) Wide - more likely a metabolic problem (hyperK, sodium channel blockade, etc*). Give empiric calcium, bicarb, and other therapies targeted for these problems (if desired) and get stat labs.
Take a minute and either go to this REBEL EM post:
https://rebelem.com/a-new-pulseless-electrical-activity-algorithm/
To review this, or look at the attached diagrams.
*Dr. Mattu would want me to remind you that hyperkalemia IS a sodium channel poisoned state, so there's no need to think of these two separately
The Critically Ill Geriatric Patient with Sepsis
Rationale: Data regarding temperature management in patients suffered from cardiac arrest with nonshockable rhythm was inconclusive.
Objective: whether moderate hypothermia at 33C, compared with normothermia at 37C would improve neurologic outcome in patients with coma after cardiac arrest with nonshockable rhythm.
Outcome: survival with favorable 90-day neurologic outcome (Cerebral Performance Category scale 1-2/5)
SummaryThere was higher percentage of patients achieving CPC 1-2 in the hypothermia group (10.2%) vs normothermia group (5.7%, Hazard Ratio 4.5, 95% CI 0.1-8.9, p=0.04)
This randomized multicenter trial involved 581 patients with cardiac arrest and nonshockable rhythm. Hypothermia group included 284 patients vs. 297 in the normothermia group. Median GCS at enrollment = 3.
Majority of patients was cooled with the use of a basic external cooling device: 37% for hypothermia and 50.8% for normothermia group.
There was higher percentage of patients achieving CPC 1-2 in the hypothermia group (10.2%) vs normothermia group (5.7%, Hazard Ratio 4.5, 95% CI 0.1-8.9, p=0.04)
Limitation:
A. The study used strict enrollment criteria:
B. normothermia group had higher proportion of patients with temperature at 38C.
C. Hypothermia group underwent temperature management of 56 hours vs. 48 hours for normothermia patients.
Take home points:
In a selected group of patients with cardiac arrest and nonshockable rhythm, moderate hypothermia at 33C may improve neurologic outcome.
Blood Transfusion Thresholds in Specific Populations
Sepsis - 7 g/dL
Acute Coronary Syndrome - no current specific recommendations pending further studies
Stable Cardiovascular Disease - 8 g/dL
Gastrointestinal Bleeds
Acute Neurologic Injury - Traumatic Brain Injury - 7 g/dL
Postpartum Hemorrhage - 1:1:1 ratio strategy
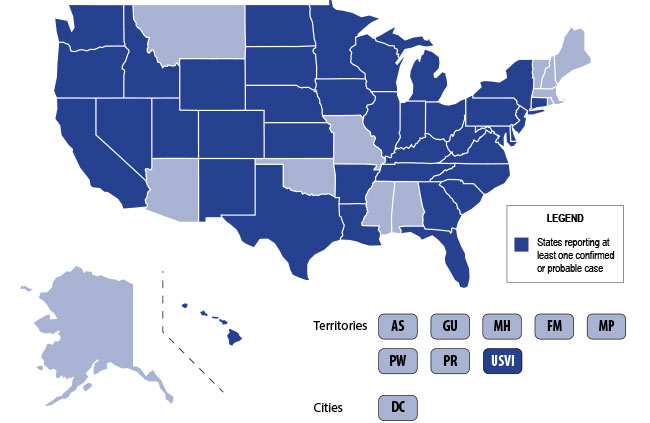
The U.S. is currently experiencing an epidemic of a severe lung disease termed Vaping-Associated Pulmonary Illness (VAPI), with over 500 cases and 7 deaths across 38 states and 1 U.S. territory since July 2019.
The clinical presentation of VAPI varies --
Diagnostics --
Treatment is supportive +/- steroids --
Bottom Line: Include vaping-associated pulmonary illness in your differential for patients presenting with acute lung disease.
Most non-OB physicians experience some fear or anxiety over taking care of the average pregnant patient. There are two patients to consider when caring for these women. Critical illness adds another layer of complexity to an already challenging patient population. Due to the normal physiologic changes that occur during pregnancy there are specific and important factors to be aware of when considering and preparing for intubation.
It's important to remember the differential for the patient with Ventricular Assist Device (VAD) difficulties, as these patients are likely to show up in your ED.
1) Assess the patient as you usually would (signs of life, mental status, breathing, arrhythmias on monitor, etc). Listen for a hum over the chest. Don't expect to feel a pulse.
2) Look at the VAD including controller, driveline, and power source for alarms, disconnections, signs of infection, and other obvious issues.
3) Look at the power (displayed flow), pulsatility index, and pump speed on the controller to help determine the cause of the issue (see attached chart). Once you have a suspected etiology, typical management of these issues is usually similar to non-VAD patients (i.e. gentle IVF for hypovolemia, vasodilators if low flow is due to afterload/hypertension, defibrillation/CPR for arresting pts, etc).
Don't forget to call your VAD coordinator when able. Consider a-line placement for precise evaluation of blood pressure (focus on MAP).
Bottom Line: Consider obstruction/thrombosis, bleeding, infection, hypovolemia, afterload/hypertension, arrhythmia, worsening LV function, and suction events when troubleshooting VADs. The power, pulsatility index, and pump speed help differentiate these conditions.
One third of your critically ill patients will have atrial fibrillation.
More than one third of those patients will develop immediate hypotension because of it.
More than one in ten will develop ischemia or heart failure because of it.
This is what you should know for your next shift:
#1 Don't wait to use electricity. If your patient is hypotensive or ischemic because of atrial fibrillation, you do not need to wait for anticoagulation before you cardiovert.
#2 Electricity buys you time to load meds. Fewer than half of patients you cardiovert will be in sinus rhythm an hour later and fewer than a quarter at the end of a day.
#3 There is no perfect rate control agent. Beta blockers have a lower mortality in A-fib from sepsis. Esmolol has the benefit of being short-acting if you cause hypotension. Diltiazem has better sustained control than amiodarone or digoxin.
#4 There is no perfect rhythm control agent. Magnesium is first-line in guidelines. Amiodarone can be used even when there is coronary artery or structural heart disease.
#5 Anticoagulation is controversial. In sepsis, anticoagulation does not reduce the rate of in-hospital stroke, but does increase the risk of bleeding. Use with caution if cardioversion isn't planned.
Critical Care Management of AIS
A new study confirmed the previously-known antibiotics to be associated with Torsades de pointes and QT prolongation (Macrolides, Linezolid, Imipenem and Fluoroquinolones). However, this study found new association between amikacin and Torsades de pointes/QT prolongation.
Methods
The authors queried the United States FDA Adverse Event Reporting System (FAERS) from 01/01/2015 to 12/31/2017 for reports of Torsade de points/QT prolongation (TdP/QT).
Reporting Odd Ratio (ROR) was calculated as the ratio of the odds of reporting TdP/QTP versus all other ADRs for a given drug, compared with these reporting odds for all other drugs present in FAERS
Results
FAERS contained 2,042,801 reports from January 1, 2015 to December 31, 2017. There were 3,960 TdP/QTP reports from the study period (0.19%).
Macrolides ROR 14 (95% CI 11.8-17.38)
Linezolid ROR 12 (95% CI 8.5-18)
Amikacin ROR 11.8 (5.57-24.97)
Imipenem-cilastatin ROR 6.6 (3.13-13.9)
Fluoroquinolones ROR 5.68 (95% CI 4.78-6.76)
Limitations:
These adverse events are voluntary reports
There might be other confounded by concomitant drugs such as ondansetron, azole anti-fungals, antipsychotics.
The Kidney Transplant Patient in Your ED
Managing the intubated patient with exacerbation of severe obstructive lung disease, especially asthma, can be very challenging as it carries higher risks of barotrauma due to higher pulmonary pressures and circulatory collapse due to auto-PEEP and decreased venous return. When measures such as medical therapy and noninvasive positive-pressure ventilation fail to prevent intubation, here are some tips to help:
1. Utilize a volume control ventilation mode to ensure a set tidal volume delivery / minute ventilation, as pressure-targeted modes will be more difficult due to the high pulmonary pressures in acute obstructive lung disease.
2. Set a low RR in order to allow for full exhalation, avoiding air-trapping / breath-stacking and circulatory collapse due to decreased venous return. This may require deep sedation and potentially paralysis.
3. Increase your inspiratory flow by shortening your inspiratory time (thereby increasing your time for exhalation.
4. Monitor for auto-PEEP:
5. Peak inspiratory pressures will be high -- what is more important is the plateau pressure, measured by performing an inspiratory hold at the end of inspiration. Provided your plateau pressure remains <30, you don't need to worry as much about the peak pressure alarms.
6. If your patient acutely decompensates in terms of hemodynamics and oxygenation -- first attempt to decompress their likely auto-PEEPed lungs by popping them off the ventilator and manually press on their chest to assist with exhalation of stacked breaths allowing venous return to the heart.
With increasing critical care boarding and the opioid crisis leading to more intubations for overdose, extubation - which was once a very rare event in the ED - is taking place downstairs more often. Prolonged mechanical ventilation is associated with a ton of complications, so it's important for the ED physician to be comfortable assessing extubation readiness. There is no single accepted set of criteria, but most commonly used are some variant of the following:
If the above criteria are met, two additional tests are frequently considered:
And don't forget to consider extubating high risk patients directly to BiPAP or HFNC!
Bottom Line: For conditions requiring intubation where significant clinical improvement may be expected while in the ED (e.g. overdose, flash pulmonary edema, etc), be vigilant about, and have a system for, assessing readiness for extubation.
The incidence of empyema as a complication of pneumonia has been increasing since the 1990's and source control requires removing the pus from the chest as soon as possible, but how large should the drain be? The American Association for Thoracic Surgery (AATS) released the most recent guidelines for identifying and managing empyema in June 2017 and at the time had no certain evidence to guide the choice of large-bore vs small-bore catheters. Most studies to guide us are flawed (not randomized), but no recently published randomized studies exist to provide a definitive answer.
Bottom line: a small-bore pigtail catheter is a reasonable choice to drain empyema and flushing it every 6 hours has been shown to prevent clogging.
POCUS in the Critically Ill Pregnant Patient
With a shortage of push dose epi, this may be an opportune time to review alternative options (see also Ashley's email on the subject).
The dose of vasopressor required to reverse hypotension has been most studied in pregnant women undergoing c-section who get epidurals and experience spinal-induced vasoplegia and hypotension (not necessarily our patient population, but we can extrapolate...)
Phenylephrine was found to reverse hypotension 95% of the time at a dose of 159 micrograms (a neo stick has 100 ug/mL, so around 1-2 mL out of the stick)
Norepinephrine reversed hypotension in 95% of patients at a dose of 5.8 ug. The starting dose for our norepi order in Epic is 0.01 ug/kg/min, so if you have a levophed drip hanging and have an acutely hypotensive patient, you may want to briefly infuse at a higher rate such as 0.1 ug/kg/min (for a typical weight patient), or bolus approximately 3-7 ug for a typical patient. Of course the degree of hypotension, particular characteristics of your patient and clinical context should be taken into consideration. When your a lucky enough to have this resource, always consult your pharmacist.
Bottom Line: To reverse acute transient hypotension you may consider:
-A bolus of phenylephrine 50-200 ug (0.5-2 mL from neo-stick)
-A bolus of norepinephrine 3-7 ug
-Briefly increasing your norepinephrine drip (if you have one) to something around 0.1 ug/kg/min in a typical weight patient
-Always search for other causes of hypotension and consider clinical context.
Wound botulism presents as descending paralysis when Clostridium botulinum spores germinate in anaerobic necrotic tissue. There have been hundreds of cases in the last decade, but it is poorly reported outside of California.
Black tar heroin and subcutaneous injection (“skin popping”) carry the highest risk, but other injected drugs and other types of drug use suffice. C botulinum spores are viable unless cooked at or above 85°C for 5 minutes or longer and this is not achieved when cooking drugs.
Early administration of botulism anti-toxin (BAT) not only saves lives but can prevent paralysis and mechanical ventilation. An outbreak of 9 cases between September 2017 and April 2018 cost roughly $2.3 million, in part because patients didn’t present on average until 48 hours after symptom onset and it took an additional 2-4 days before the true cause of their respiratory depression and lethargy were understood. One patient died.
PEARL: talk to your injecting drug users about the symptoms of botulism: muscle weakness, difficulty swallowing, blurred vision, drooping eyelids, slurred speech, loss of facial expression, descending paralysis, and difficulty breathing. Consider botulism early in your patients who inject drugs but who do not respond to naloxone or who exhibit prolonged symptoms. Testing at the health department is performed with mouse antibodies to Botulism Neurotoxin (BoNT) combined with the patient’s serum.
Post-Arrest Prophylactic Antibiotics?
Little people (patients with achondroplasia or "dwarfism") have little lungs. Even though the trunk may appear to be a normal size with small limbs, the vital capacity is actually about 75% the predicted value based on the patient's sitting height. Macrocephaly and a decreased anterior-posterior depth are the cause for this. When you want to mechanically ventilate a little person, you can estimate their height based on a typical person with the same sitting height, but their actual volume will be about 3/4 the tidal volume predicted.
When intubating, remember these patients also have a high risk of basicranial hypoplasia (the foramen magnum may be small and key-hole shaped). These patients will be predisposed to compress the vertebral arteries when you tilt the head back and this itself can cause ischemia of the medulla and pons leading to central apnea.
Stokes DC, Wohl ME, Wise RA, et al. The lungs and airways in Achondroplasia. Do little people have little lungs? CHEST. 1990; 98(1):145-52
Pauli RM. Achondroplasia: A comprehensive review. Orphanet Journal of Rare Diseases. 2019; 14(1):
Some patients with severe pulmonary hypertension receive continuous infusions at home of prostacyclins, such as epoprostanol (flolan). These are generally delivered via a pump that the patient wears, which is attached to an indwelling catheter. As with any indwelling device, they are at risk for infection and other complications, including malfunction.
Interruption of delivery of the medication can result in rapid cardiovascular collapse, sometimes within minutes. In this instance, the medication should be resumed as quickly as possible (by a traditional IV if the catheter is not functional), and the patients should be treated as one would approach a patient with decompensated right heart failure.
I once saw a patient in the ED whose listed chief complaint was "medication refill", but was actually there for dislodgement of her prostacyclin catheter (thankfully she was ok). With more patients receiving devices they are dependent upon (insulin pumps, AICDs, prostacyclin catheters), be wary of chief complaints such as "medication refill" or "device malfunction."
Bottom Line: Interruption of continuous prostacyclin therapy for pulmonary hypertension can be rapidly fatal and should be addressed immediately.