Right Heart Failure in the Critically Ill
A Cochrane review of 37 studies concluded that Succinylcholine (SUC) is superior to Rocuronium (ROC) during rapid sequence intubation.
The authors claim that compared to ROC, SUC has a faster onset of action (45 vs. 60 seconds) and overall a shorter duration of action (10 vs. 60 minutes).
Dr. Reuben Strayer wrote a letter to the journal editors and stated that these findings should be interpreted carefully; he highlighted that most of the studies in the review used doses of ROC less than 0.9 mg/kg (most studies used 0.6mg/kg).
Dr. Strayer asserted that ROC’s onset of action is dose dependent; when using doses of 1.2 mg/kg, ROC’s onset is indistinguishable from that of SUC. He also stated another major benefit of ROC is the lack of adverse effects that SUC possesses (hyperkalemia and malignant hyperthermia).
What are your thoughts on this? Go to http://www.facebook.com/Criticalcarenow and take the poll (there are 5 choices). Results will be posted next week.
AKI and Fluid Balance
Femoral venous access is typically limited to the acute resuscitation of critically-ill patients. Several practice-guidelines recommend avoiding the femoral site, or removal once admitted to the ICU, because of the risk of catheter-related bloodstream infection (CRBI) and deep-vein thrombosis (DVT).
A recent systematic review and meta-analysis (including two randomized-control trials and eight cohort-studies) evaluated the risk of CRBI and DVT for catheters placed in either the internal jugular, subclavian, or femoral-venous sites. No difference in the rate of CRBI or DVT was found between the three sites, although the DVT data was less robust (i.e., contained heterogeneous data).
The authors hypothesized that improvements in sterility during central-line placement (e.g., full-barrier precautions), improved nursing care (e.g., central-line site care), and ultrasound guidance may have led to a reduction in femoral site complications.
Although a prospective randomized-control trial is necessary to confirm these results, this meta-analysis challenges the traditional teaching that femoral central-access should be avoided.
Lung Protective Ventilator Settings Still Underutilized
Crystalloids (i.e., 0.9% saline and lactated ringers) have been used during resuscitation for more than a century. Their invention, however, was more accidental than intentional.
Crystalloids were first used during the European Cholera epidemic of 1831. Hartog Hamburger later modified this solution in 1896 to the solution we know today as "normal" saline. Hamburger's solution was only intended for in vitro study of RBC lysis and was never intended for clinical use.
Around this time, Sydney Ringer was testing several fluids to use for physiologic studies. Ringer's lab assistant was erroneously substituting tap water for distilled water when preparing these solutions. Ringer later discovered that this tap water contained minerals making the solution "physiologic", isotonic, and safe for human use; Alexis Hartmann later added sodium lactate to create Ringer's Lactate.
Since the invention of crystalloids, many types of resuscitation fluids have been created and studied (i.e., albumins, gelatins, and starches); all have been shown to be more expensive, with no more benefit, and with possibly more harm when compared to crystalloids.
The "perfect" resuscitation fluid still alludes us today, but of all of the solutions marketed crystalloids are arguably the best...despite their accidental history.
Steroids and Septic Shock
Wernicke encephalopathy (WE) is a neurologic disorder secondary to prolonged thiamine deficiency; it is characterized by confusion, ataxia, and ocular abnormalities.
Traditional medical teaching advises against the administration of glucose (or glucose containing fluid) in thiamine deficient patients, without first giving thiamine, as this may precipitate WE.
This teaching is problematic, however, in hypoglycemic patients who require the immediate administration of glucose while simultaneously being suspected of thiamine deficiency (e.g., malnourished alcoholics). Delays in treating hypoglycemia may be more harmful (e.g., seizures, permanent neurologic deficits, etc.) than the risk of WE.
Schabelman et. al performed a literature search to unearth the origins of this teaching. Nineteen papers related to this topic were found consisting of case reports, animal studies, and expert opinion; there were no randomized trials, cohort studies, or case-control studies.
Bottom-line: The available evidence does not support withholding glucose treatment until thiamine can be administered and educators should consider abolishing this dogmatic teaching until better evidence is available.
Anaphylaxis
Septic patients with hemodynamic instability often require intravenous fluids as part of their resuscitation. Major debate has occurred whether the optimal resuscitation fluids are crystalloids (e.g., normal saline) or colloids (e.g., albumin).
In theory, colloids are more potent intravascular expanders than crystalloids because their oncotic pressure is higher and should increase intravascular volume similarly to larger amounts crystalloid (i.e., colloids require less volume during resuscitation).
Despite these theoretical benefits, the colloid hydroxyethyl starch (HES), has come under scrutiny after prior studies have linked its use with adverse outcomes.
A recent prospective randomized-control trial compared the use of HES to lactated acetate for resuscitating septic patients and found that HES significantly increased both the incidence of renal-replacement therapy and mortality at 90 days (both primary end-points in the study).
Bottom line: There is no convincing data that HES performs superiorly to crystalloid for resuscitation in sepsis and there is increased harm with its use. Furthermore, the increased cost of HES compared to crystalloids does not justify its routine use.
Acute Kidney Injury and Tumor Lysis Syndrome
Two recently presented abstracts at the 2012 Society of Critical Care Medicine conference suggest that the combination of vancomycin and piperacillin-tazobactam may lead to acute kidney injury (AKI) in the critically ill. There may also be evidence to suggest that piperacillin-tazobactam alone increases the risk of AKI.
Both abstracts retrospectively compared patients who received either vancomycin alone or the combination of vancomycin and piperacillin-tazobactam. In both studies, the rates of AKI were significantly lower in patients treated with vancomycin alone as compared to patients receiving both vancomycin and piperacillin-tazobactam.
Bottom line: Although the current evidence does not support a change in our clinical practice, more prospective studies exploring this topic are necessary.
Use the Measured Sodium Concentration!
Consider rhabdomyolyisis secondary to heat exposure as summertime approaches; have a low threshold to screen patients if they are at risk (e.g., people exercising in high-ambient temperatures).
Symptoms include muscle tenderness, cramping, and swelling with associated weakness. Patients with altered mental status (e.g., heat stroke) should be examined for limb induration, skin discoloration (i.e., ischemia), or compartment syndrome.
Complications:
Treatment
Severe UGIB
Carcinoid tumors are neuroendocrine malignancies typically located in the GI tract; most commonly in the terminal ilium and appendix.
Carcinoid tumors produce serotonin, histamine, bradykinin, and/or prostaglandin that result in diarrhea, facial flushing, or bronchospasm. These vasoactive substances may also lead to hypotension and vasodilatory shock.
The tumor may also affect the tricuspid and pulmonary valves leading to right-heart failure secondary to valvular regurgitation, stenosis or both.
Treatment is directed at controlling the malignancy (e.g., octotrotide and tumor resection) as well as managing the right-sided heart failure when it occurs (e.g., inotropes, diuretics, vasopressors, etc.).
Balloon Tamponade for Variceal Bleeding
Severe acute pancreatitis (SAP) is a life-threatening form of pancreatitis, with up to 30% mortality.
SAP may lead to hypovolemic shock (secondary to vasodilation and capillary leak), hypoxemia (from acute respiratory distress syndrome), and multi-organ failure.
Suspect SAP with signs and symptoms of pancreatitis plus any of the following:
Treatment of SAP should focus on:
SBP, HRS, and Albumin
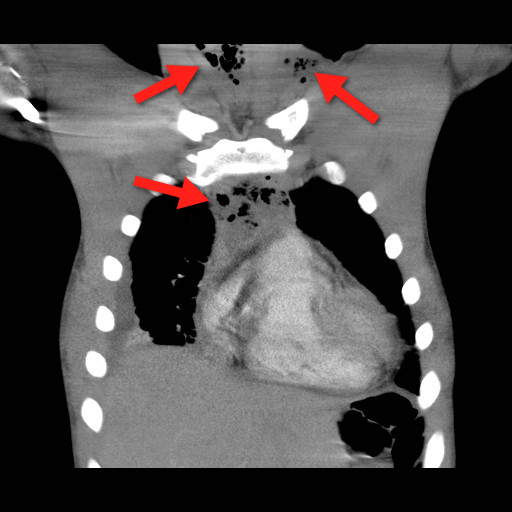
Mediastinitis is an infection of the mediastinum; a rapidly fatal surgical emergency if not recognized and treated early.
Causes include esophageal perforation, oropharyngeal infections (e.g., Ludwig’s angina), prevertebral or carotid space infections, and iatrogenically (endoscopy, hypopharyngeal perforations during intubation, etc.).
Plain films (neck / chest) may serve as a screening tool, but CT best defines the source and extent of disease; the CT below demonstrates gas within the soft-tissues and the mediastinum (red arrrows).
Infections may be polymicrobial and broad-spectrum antibiotics with anaerobic coverage (e.g., pipercillin-tazobacam) should be started initially.
Immediate treatment should also include:
Bonus Pearl
Can't keep up with all the great educational stuff in Emergency Medicine and Critical Care? Let the professionals at Life in the Fastlane do it for you (http://lifeinthefastlane.com). These guys scour the web and blog about the best educational pearls, podcasts, and radoiolgic finds...and they're also quite the laugh. Check them out today!