Cervical Radiculopathy
The most commonly affected level is C7 (31-81%), followed by C6 (19-25%), C8 (4-12%) and C5 (2-14%)
Anterior compression can selectively affect motor fibers
Posterior compression can selectively affect sensory fibers
-More common due to posterior lateral disc herniation or facet degeneration
Signs and symptoms: Sensory complaints (findings are in a root distribution) and possible weakness and reflex changes.
Dr. Corwell covered Spondyloysis in July 2010 https://umem.org/res_pearls_referenced.php?p=1134 but if you are like me you might have trouble remembering the differences between the following terms:
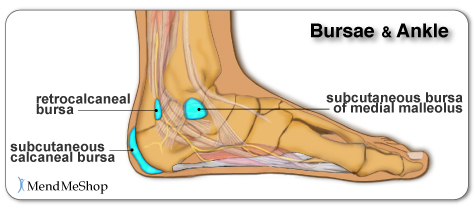
Chief complaint: “Posterior heel pain”
http://www.aidmybursa.com/_img/ankle-retrocalcaneal-subcutaneous-bursitis.jpg
Retrocalcaneal bursitis
The retrocalcaneal bursa is located between the Achilles tendon and the posterior superior border of the calcaneus.
H&P: Inflammation and pain may follow repetitive dorsi/plantar flexion of the ankle (excessive running, jumping activities). Tenderness anterior and superior to the Achilles insertion on the heel.
Treatment: Minimize weight bearing. ½ inch elevation. NSAIDs.
Posterior calcaneal bursitis
This bursa is subcutaneous, just superficial to the insertion of the Achilles tendon.
H&P: Inflammation and pain may follow irritation from the upper border of the heel counter of a shoe. Posterior heel pain. Tender “bump” (the inflamed and swollen bursa) on the back of the heel.
http://podiatry.files.wordpress.com/2006/12/patient2.jpg
Treatment: Opened-heeled shoes, sandals, or placement of a “U-shaped” pad between the heel and the counter. NSAIDs. Advance to shoes with soft or less convex heel counters.
Evaluation of Potential Intra-Articular Joint Lacerations
Skin and soft tissue injuries in proximity to a joint often prompt concern of whether the injury violated the joint space. Joint Space involvement is important to exclude as it can lead to septic joints and long term disability.
One easy way to determine if the joint capsule has been violated is to inject methylene blue into the joint and watch to see if any of the methylene blue extravasates through the soft tissue.
Indications for a methylene blue injection include:
There are no absolute contraindications. Though clearly the procedure does not need to be done when the injury highly suggests an open joint injury and the patient will require operative debridement and exploration.
To watch a video of a injection head to eMedicine by clicking http://emedicine.medscape.com/article/114453-overview
Transverse Myelitis
A group of inflammatory disorders characterized by acute or subacute motor weakness, sensory abnormalities and autonomic (bowel, bladder, sexual) cord dysfunction.
Symptoms are usually bilateral but both unilateral and asymmetric presentations can occur.
Look for a well-defined truncal sensory level
-below which sensation of pain and temperature is altered or lost.
Causes: Autoimmune after infection or vaccination (60% of cases in children), direct infection, or a demyelinating disease such as MS. No cause is found in 15 – 30% of cases.
Incidence: Bimodal peak at 10-19 years and at 30-39 years.
Diagnostic testing: MRI of the ENTIRE spine to both rule out structural lesions and rule in an intrinsic cord lesion. If MRI is normal reconsider the original diagnosis.
Treatment: Steroids are first-line therapy. Dosing is controversial but generally involves high IV doses for 3-5 days (1000 mg methylprednisolone). Plasma exchange is second line for those who don’t respond to steroids.
Risk Factors for Spinal Epidural Abscesses
Building on Dr. Corwell's pearl from last week concerning Spinal Epidural Abscess, risk factors for Spinal Epidural Abscesses other than IV drug abuse are:
The infection can occur via three routes 1) hematogenous spread 2) Direct Extension from a local infection such as osteoomyelitis, and 3) iatrogenic introduction which is thought to be responsible for 14-22% of the cases. A catheter in the epidural space for more than 2 days has a infection rate of 4.3%.
Epidural compression syndrome encompasses spinal cord compression, cauda equina syndrome, & conus medullaris syndrome.
Causes include:
Measurement of a post-void bladder residual volume tests for the presence of urinary retention with overflow incontinence (a common, though late finding) (sensitivity of 90%, specificity of 95%). Large post-void residual volumes (>100 mL) indicate a denervated bladder with resultant overflow incontinence and suggest significant neurologic compromise. The probability of cauda equina syndrome in patients without urinary retention is approximately 1 in 10,000.
Use this in your daily practice!!
The administration of glucocorticoids can minimize ongoing neurologic damage from compression & edema until definitive therapy can be initiated. The optimal initial dose and duration of therapy is controversial, with a recommended dose range of dexamethasone anywhere from 10 to 100 mg intravenously. Consider traditional dosing (dexamethasone 10 mg) for those with minimal neurologic dysfunction, & reserve the higher dose (dexamethasone 100 mg) for patients with profound or rapidly progressive symptoms, such as paraparesis or paraplegia.
Subungual Hematomas:
Previous pearls have described tips for smart and safe documentation of typical ED complaints such as chest pain. Properly assessing and documenting orthopedic complaints is likewise very important. No evaluation or chart is complete if it does not include include the following 7 components:
The joint above
The joint below
Motor
Sensory
Vascular
Skin
Compartments
The joint above/below is important in cases of shoulder and hip pain actually being radicular pain (from the neck and back respectively). Also, hip pain from trauma may be due to a femur fracture for example.
For motor and sensory evaluation, test the most distal isolated innervation of a particular nerve (L5 - great toe dorsiflexion for example).
Note distal pulses and check ABIs for injuries with potential subtle vascular findings.
Note intact skin especially in cases where the joint will be covered by a splint.
Note "soft" compartments especially in cases of forearm and lower leg fractures.
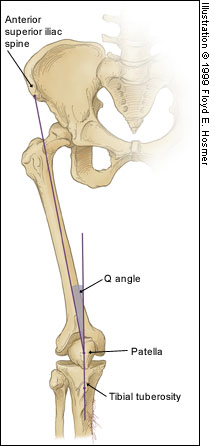
Patellofemoral Syndrome (Chondromalacia Patella)
Injury was originally described as an occupational hazard in Scottish gamekeepers (from breaking the necks of rabbits against the ground). Today, skiing is now the most common cause and injury is now the second most common orthopedic injury in skiers (MCL injury #1).
Injury to the ulnar collateral ligament (UCL) results from a sudden forced abduction (radial deviation) stress at the MCP joint of the thumb, commonly due to a fall against a ski pole or the ground.

http://blog.fitter1.com/wp-content/uploads/2010/04/b_14_1_2a.jpg
The most frequent site of rupture is the insertion into the proximal phalanx. The UCL may even avulse a small portion of the proximal phalanx at its insertion site.

http://img.medscape.com/pi/emed/ckb/sports_medicine/84611-97564-98460-1652013.jpg
Consider imaging before stress testing (to avoid further displacing a fracture)

http://img.medscape.com/pi/emed/ckb/sports_medicine/84611-97564-98460-1652060.jpg
Stabilize in a thumb spica splint and refer to hand surgery.
Calling this entity a “simple sprain” may result in chronic disability (chronic pain, instability, loss of pinch strength)
Pain Control in the Elderly
So the take home lesson for this pearl is that the elderly have a lower risk of delirium if their pain is treated appropriately.
Supraspinatus: “Empty can” test. Have the patient abduct the shoulders to 90 degrees in forward flexion with the thumbs pointing downward. The patient attempts to lift the arms against the examiner’s resistance.
http://bjsportmed.com/content/42/8/628/F2.large.jpg
Infraspinatus and teres minor: These muscles are responsible for external rotation of the shoulder. Have the patient flex both elbows to 90 degrees while the examiner provides resistance against external rotation.
http://www.physio-pedia.com/images/4/4b/Infraspinatus_test.jpg
Subscapularis: “Lift-off” test. The patient rests the dorsum of the hand on the lower back (palm out) and then attempts to move the arm and hand off the back. Patients with tears may be unable to complete test due to pain.
http://www.aafp.org/afp/2008/0215/afp20080215p453-f4.jpg
Radiologic evaluation of the elbow (Part 2)
Helpful clues in the evaluation of elbow trauma:
Adhesive Capsulitis -- Frozen Shoulder
Rotator Cuff Tears:
Four muscles make up the rotator cuff (SITS) which control internal and external rotation of the shoulder and abduct the shoulder.
Tears can be due to acute injuries (falls, heavy lifting, forceful abduction), though the majority (>90%) of rotator cuff tears are chronic in nature and due to subacromial impingement and decreased blood supply to the tendons.
Most patients can be treated with sling immobilization, NSAIDs and referral to sports medicine or orthopaedic surgeons. Elderly patients should be referred quickly as prolonged immobilization can lead to a frozen shoulder.
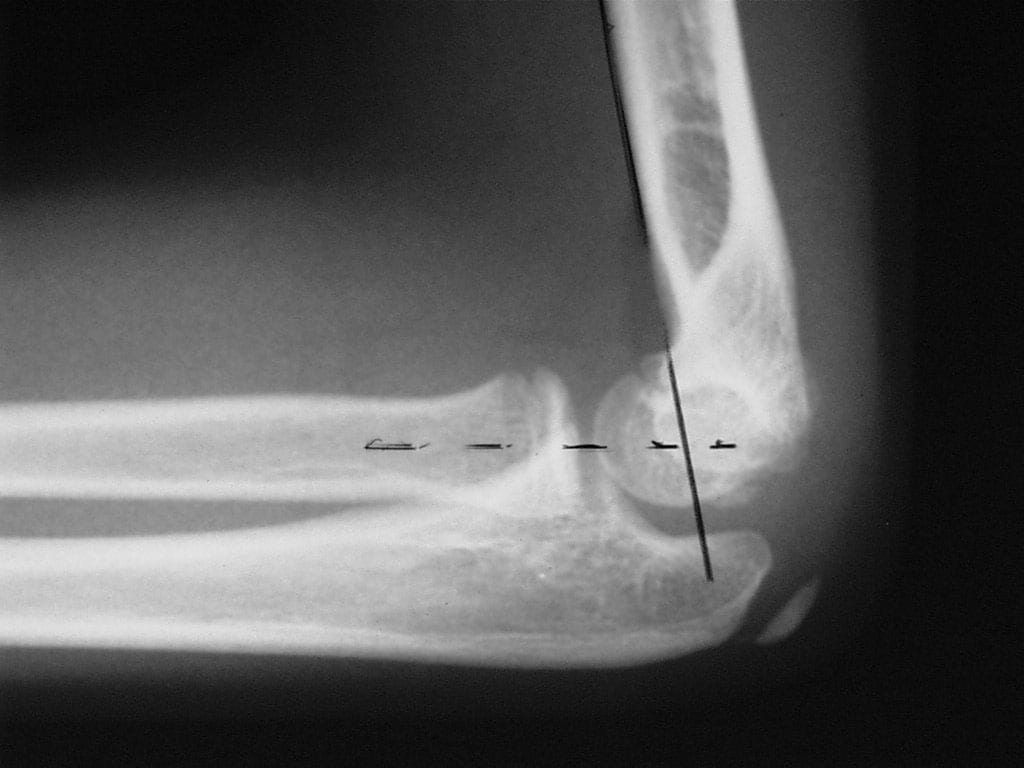
Helpful clues in the evaluation of elbow trauma
Fat pads: The fat pad sign can be seen with any joint effusion (infection, inflammation) but in the setting of trauma, effusions are indicative of fractures about the elbow (even if no fracture line can be identified).
There are two fat pads within the elbow. Normally, on a true lateral radiograph only the anterior fat pad is seen as a small triangular radiolucent shadow anterior to the distal humeral diaphysis. The posterior fat pad is ordinarily not visualized on a lateral radiograph because it is tucked away within the olecranon fossa.
Normal lateral view: http://nypemergency.org/images/ElbowNormal.jpg
With fractures, the joint becomes distended with blood. The anterior fat pad becomes displaced superiorly and outward from the humerus giving the so called "sail sign." Similarly, the posterior fat pad gets displaced out of the olecranon fossa and becomes visible on the lateral radiograph.
Anterior (sail) and posterior fat signs: http://nypemergency.org/images/Elbowsfatpadarrow.jpg
Some common injuries and their board review associated complications
| History and Physical Examination Red Flags | |
| Historical Red Flags | Physcial Red Flags |
| Age under 18 or over 50 Pain lasting more than 6 weeks History of cancer Fever and chills Night sweats, unexplained weight loss Recent bacterial infection Unremitting pain despite rest and analgesics Night pain Intravenous drug users, immunocompromised Major trauma Minor trauma in the elder | Fever Writhing in pain Bowel or bladder incontinence Saddle anesthesia Decreased or absent anal sphincter tone erianal or perineal sensory loss Severe or progressive neurologic defect Major motor weakness |
The Salter Harris Classification System is used in pediatric epiphyseal fractures. The higher the type of fracture the poorer the prognosis
Some common exam facts about Salter Harris Fractures are:
The Classification system as listed by Type:
A image of the fractures can be found on FP Notebook at http://www.fpnotebook.com/_media/OrthoFractureSalterHarris.jpg
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}