Category: Orthopedics
Keywords: Back pain (PubMed Search)
Posted: 2/8/2020 by Brian Corwell, MD
(Updated: 5/22/2026)
Click here to contact Brian Corwell, MD
Taking an accurate history to diagnose Cauda Equina Syndrome (CES)
Classic teaching is to inquire specifically about bowel and bladder function, sexual dysfunction, and/or loss of sensation in the groin.
Rather than asking about urinary incontinence, clinicians should ask specifically about difficulty passing urine, new leakage and retention.
Discussing issues related to sexual dysfunction are difficult for both clinicians and patients.
Rather than asking if there are any issues with sexual function, a more direct and informative way would be to ask if the patient has a “change in ability to achieve an erection or ejaculate” or “loss of sensation in genitals during sexual intercourse.”
Saddle anesthesia has the highest predictive value in diagnosing MRI-proven CES. Loss of sensation may be incomplete and patchy. Ask about change in sensation with wiping after a bowel movement.
Greenhalgh S, Truman C, Webster V, Selfe J. Development of a toolkit for early identification of cauda equina syndrome. Prim Health Care Res Dev. 2016;17(6):559-567.
Category: Orthopedics
Keywords: Concussion, (PubMed Search)
Posted: 1/25/2020 by Brian Corwell, MD
(Updated: 5/22/2026)
Click here to contact Brian Corwell, MD
Timeliness of Concussion Referral
Do patients with a self-limited diagnosis of “concussion” require specialty follow up?
If so, is there a benefit to earlier evaluation?
Recently published research from the University of Pittsburgh Sports Medicine Concussion Program suggests so.
Subjects: 162 concussed athletes between the ages of 12 and 22
Findings: Athletes treated in the first week after injury recovered faster than those who did not receive care until 8 to 21 days post injury.
Note: Once in care the length of time spent recovering was the same for both groups. This suggests that the amount of time prior to the initiation of care may explain the longer recovery time of the 2nd group.
Earlier recovery can help minimize effects on mood, quality of life and lost time in school/work.
Take home: Consiuder early follow up referral to a qualified provider for all concussed patients seen in the ED
Kontos et al., 2020. Association of Time Since Injury to the First Clinic Visit With Recovery Following Concussion. Jama Neurology.
Kontos et al., 2020. Association of Time Since Injury to the First Clinic Visit With Recovery Following Concussion. Jama Neurology.
Category: Orthopedics
Keywords: Klein's line, S sign, AVN (PubMed Search)
Posted: 12/14/2019 by Brian Corwell, MD
(Updated: 5/22/2026)
Click here to contact Brian Corwell, MD
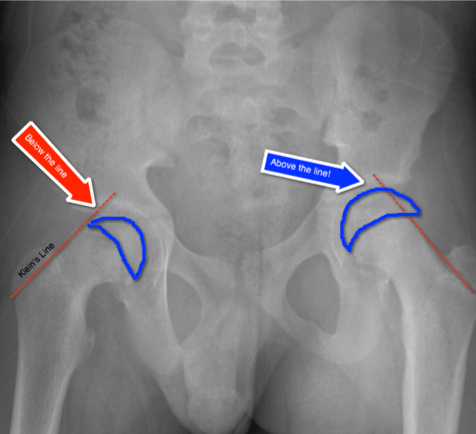
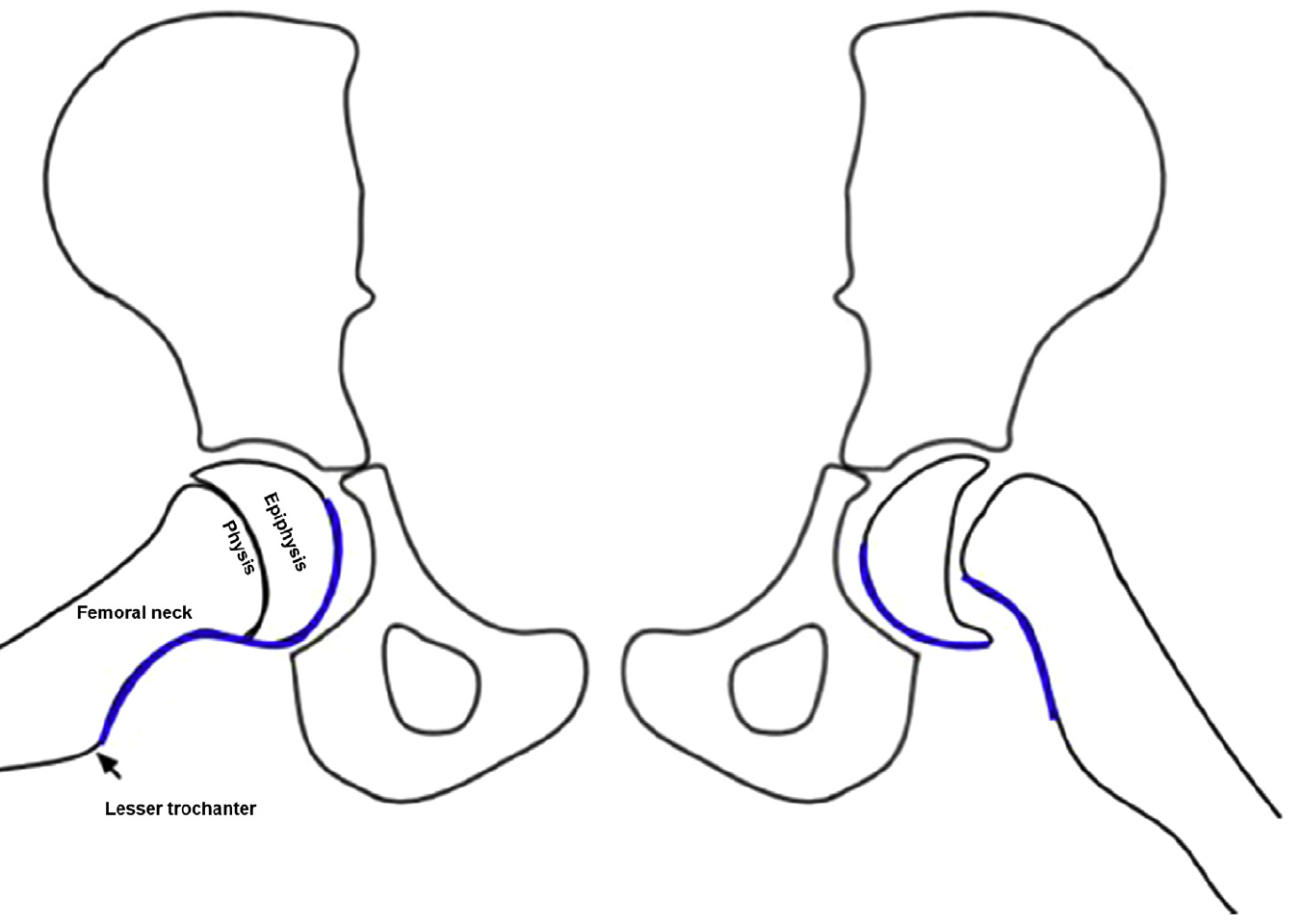
Slipped Capital Femoral Epiphysis (SCFE)
http://www.raymondliumd.com/images/SCFE%20illustrated%20and%20cropped.jpg
Early Diagnosis:
Klein’s Line on AP view
https://pedemmorsels.com/wp-content/uploads/2018/01/Slipped-Capital-Femoral-Epiphysis-3.png
Another virtual line may assist in diagnosis
S-sign
Klein's line and S-sign
Consider adding both of these virtual lines/signs to your review of the pediatric hip plain film
Rebich et al., 2018. The S Sign: A New Radiographic Tool to Aid in the Diagnosis of Slipped Capital Femoral Epiphysis. J Emerg Med.
Category: Orthopedics
Keywords: back pain, muscle relaxants (PubMed Search)
Posted: 11/23/2019 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
The role of skeletal muscle relaxants in the management of lower back pain in the ED
Patients with lower back pain (LBP) presenting to the ED are often treated with NSAIDs plus skeletal muscle relaxants.
A recent study in Annals of Emergency Medicine compared functional outcomes and pain in ED patients with acute non radicular LBP with 4 different treatment regimens.
Conclusion: Adding a muscle relaxant to ibuprofen did not improve pain or improve function at 1 week following an ED visit for LBP.
Note: Prior studies have found no benefit to adding opioids or diazepam to NSAIDs for ED patients with acute non radicular LBP
Friedman et al., 2019. Annals of Emergency Medicine
Category: Orthopedics
Keywords: geriatrics, orthopaedic, fractur (PubMed Search)
Posted: 11/16/2019 by Michael Bond, MD
(Updated: 5/22/2026)
Click here to contact Michael Bond, MD
Therefore, pain medications must be dosed carefully, which runs the risk of underdosing. Pain medications can also contribute to delerium, and decreased functional status.
Recommendations:
Category: Orthopedics
Keywords: Hip pain, bursitis (PubMed Search)
Posted: 11/9/2019 by Brian Corwell, MD
(Updated: 5/22/2026)
Click here to contact Brian Corwell, MD
Lateral hip pain is a common presentation of hip pain.
Typically seen in runners and women over the age of 40 who start unaccustomed exercise.
Pain from OA of the hip which is typically medial (groin pain)
Lateral hip pain has traditionally been diagnosed at trochanteric bursitis.
Research suggests that lateral hip pain may be multifactorial and better termed Greater trochanteric pain syndrome.
Pain from the gluteal medius and/or minimus due to non-inflammatory tendonopathy is likely causative. This may cause a secondary bursitis.
Pain is insidious, gradual worsens and is variable based on activity type.
Also, can be seen after a fall resulting in tearing.
Pain is described as a deep ache or bruise. It can stay localized or radiate down lateral thigh towards knee.
Patients report night/early morning pain and when rolling over onto the outer hip on affected side.
Fatigue from prolonged sitting, walking and single leg loading activities such as walking up stairs.
Provoking activities and postures cause compressive forces on the involved tendons.
These generally occur when the hip is adducted across midline such as with
Side sleeping,
Place pillow between legs to align pelvis and keep knee and hip in line
Crossed leg sitting
Sit w/ knees at hip distance and feet on floor
Selfie poses - Standing w a hitched hip (pushing hip to the side).
Attempt to correct biomechanical issues before progressing directly to bursal steroid injection
May only be a temporary fix if underlying issue not addressed.
A helpful clinical guide
https://bjgp.org/content/bjgp/67/663/479/F1.large.jpg?download=true
Category: Orthopedics
Keywords: Concussion Incidence, epidemiology, (PubMed Search)
Posted: 10/26/2019 by Brian Corwell, MD
(Updated: 5/22/2026)
Click here to contact Brian Corwell, MD
A recent epidemiology study in Pediatrics looked at concussions in 20 high school sports during the 2013–2014 to 2017–2018 school years.
For every athlete, one practice or competition was counted as one exposure.
Overall, 9542 concussions were reported for an overall rate of 4.17 per 10 000 athletic exposures (AEs).
Football continues to have the highest incidence with a concussion rate of 10.40 per 10 000 AEs.
As in previous studies, rates in competition (33.19 to 39.07 per 10 000 AEs) are increasing and higher than rates in practice which are lower and decreasing over the study period (5.47 to 4.44 per 10 000 AEs).
This may reflect better reporting or increasing injury rate
In all 20 sports, recurrent concussion rates decreased from 0.47 to 0.28 per 10 000 AEs.
Confirming prior studies, among sex-comparable sports, concussion rates were higher in girls than in boys (3.35 vs 1.51 per 10 000 AEs).
Also, among sex-comparable sports, girls had larger proportions of concussions that were recurrent than boys (9.3% vs 6.4%).
This study may reflect effective implementation of strategies to reduce concussion incidence such as mandatory removal from play and more stringent requirements associated with return to play.
Concussion Incidence and Trends in 20 High School Sports, Kerr et al., 2019, Pediatrics.
Category: Orthopedics
Keywords: Playing surface, concussion (PubMed Search)
Posted: 10/12/2019 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Synthetic turf playing surfaces have been growing in popularity over the last decade and seem to have become a new standard.
Due to the need for durable fields that can accommodate multiple teams/activities, in addition to the high cost of maintaining grass and the need to conserve water, many parks and schools have switched from grass to turf. Turf is advertised as maintenance free but ….this is not the case.
Locally, at M&T Bank Stadium, groundskeepers drive a LitterKat turf sweeper across the field for 4 hours 2-3 times a week to ensure that the synthetic rubber is cleaned and distributed evenly. The field is also repainted every 4 games because the paint may become hard. The cost of this level of maintenance is beyond what many parks and local high schools can afford.
A recent study examined high school concussion data at almost 2000 high schools with over 14,000 recorded concussions. Researchers concluded that more concussions occurred in games than practices. Interestingly, they also found that playing surface was significantly associated with concussion. Almost 90% of all injuries occurred on turf-based surfaces. Turf outweighed all other mechanisms of injury, including helmet-to-helmet hits and grass playing surface. Between 10 and 15.5% of concussions occur from helmet to ground contact. In the NFL, this mechanism accounts for about 1 in 7 concussions.
Attempting to limit total exposure time in practice and games on turf surfaces may be beneficial until more study is needed.
Category: Orthopedics
Keywords: Tenosynovitis, wrist pain (PubMed Search)
Posted: 9/28/2019 by Brian Corwell, MD
(Updated: 5/22/2026)
Click here to contact Brian Corwell, MD
Intersection Syndrome
De Quervain’s is a common tenosynovitis is involving the the 1st dorsal compartment of the wrist/forearm.
Intersection syndrome is a tenosynovitis that occurs at the intersection of the 1st and 2nd dorsal compartments.
Pathology located at crossing point of the 1st compartment structures (APL and EBP) with the radial wrist extensors (ECRB and ECRL)
Occurs most commonly from repetitive wrist extension and is common in rowers, weight lifters, and in those playing racquet sports.
Occurs about 4 to 6cm proximal to the radiocarpal joint VERSUS De Quervain’s which occurs near the level of the radial styloid.
Pain worse with resisted wrist and thumb extension
Radiographs not required
Splint and start NSAIDs
Recalcitrant cases can be referred for corticosteroid injection
https://stemcelldoc.files.wordpress.com/2012/09/intersection-syndrome-referral-pain-pattern1.jpg
Category: Orthopedics
Keywords: foot fracture, radiology (PubMed Search)
Posted: 9/14/2019 by Brian Corwell, MD
(Updated: 5/22/2026)
Click here to contact Brian Corwell, MD
Imaging of Lisfranc Injuries
Tarsometatarsal fracture-dislocation
Anatomy
3 Columns of the midfoot, divided by the tarsometatarsal joints
The Lisfranc ligament
- Extends from the 2nd MT to the medial cuneiform
- Critical to structure and stabilization of the 2nd MT and the midfoot arch
Imaging
Plain films: AP/lateral/oblique
Consider weight bearing view with contralateral comparison if high suspicion
CT: Can be useful to confirm abnormal plain films
MRI: not done in ED but can be used to diagnose pure ligament injuries
Below is a review of the lines of the foot which will ensure not missing this diagnosis. May be helpful to review with sample imaging.
Plain films findings: https://prod-images.static.radiopaedia.org/images/49189279/86408d5bae08ab80ae9ef377337ab7_big_gallery.jpeg
On AP view:
On Lateral view:
On the Oblique view:
Remember that the lateral margin of the 5th MT can project lateral to the cuboid (up to 3 mm)
Lines drawn on 2 view foot for review
https://radiopaedia.org/cases/lisfranc-ligament-normal-alignment
Orthobullets.org
Category: Orthopedics
Keywords: Foot, instability, dislocation (PubMed Search)
Posted: 8/24/2019 by Brian Corwell, MD
(Updated: 5/22/2026)
Click here to contact Brian Corwell, MD
Tarsometatarsal fracture-dislocation
The Lisfranc ligament is critical for stabilization of the midfoot arch and the 2nd MT
Injuries can range from mild (sprains) to severe (gross dislocation)
Injury may be purely ligamentous injuries or a fracture-dislocations
Difficult diagnosis to make
https://www.aafp.org/afp/1998/0701/afp19980701p118-f4.jpg
Mechanisms: MVAs, fall from height or athletic injuries
Common athletic mechanism: Axial load to a hyperplantar flexed forefoot
Injury severity is often underestimated
Severe pain and inability to weight bear
Plantar bruising and bruising throughout midfoot
No specific tests as exam is limited due to pain
Midfoot stress tests
-Often positive but unlikely to be allowed by patient due to pain
https://www.youtube.com/watch?v=v8SGVwz2RHs
Midfoot instability test
Grasp metatarsal heads and apply dorsal force to forefoot.
Other hand palpates the TMT joints and feels for dorsal subluxation
Category: Orthopedics
Keywords: Anterior knee pain (PubMed Search)
Posted: 8/10/2019 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Plica Syndrome
-A painful impairment of knee function resulting from thickened and inflamed synovial folds
Plicae are embryologic remnant inward folds of the synovial lining present in most knees
Most plica are asymptomatic
A pathological synovial plica can become inelastic, thickened and fibrotic. It may bowstring across the femoral trochlea at 70 to 100 degrees of knee flexion
Can be a cause of anterior knee pain/mechanical Sxs
Medial patellar plica most commonly involved
Hx: Snapping sensation, pain w/ sitting or repetitive activity
Anterior knee pain, clicking, clunking, and a popping sensation on knee loading activity such as squatting/stairs or with prolonged sitting
Many present with history of blunt trauma to the anterior knee
PE: A taut band of tissue that reproduces concordant pain with palpation
Tenderness in the medial parapatellar region
Painful, palpable medial parapatellar cord
-This can be rolled and popped beneath the examiners finger
The knee may be tender to the touch, swollen, and stiff
Can be difficult to distinguish from other intra-articular conditions such as meniscal tears, articular cartilage injuries, or osteochondral lesions,
The examiner can then palpate for the plica by rolling one finger over the plica fold, which is located around the joint lines in anterior knee compartment
https://www.ortho.com.sg/wp-content/uploads/2018/04/medial-plica-syndrome-31-e1478966479644.jpg
Lee et al., 2017. Surg J. Synovial Plica Syndrome of the Knee: A Commonly Overlooked Cause of Anterior Knee Pain.
Category: Orthopedics
Keywords: Bone stress reaction, fracture, overuse injury (PubMed Search)
Posted: 7/27/2019 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Bone stress injury (BSI) in Adolescents
A BSI occurs along a pathology continuum that begins with a stress reaction and may progress all the way to a stress fracture.
Difficult to diagnose clinically.
Identifying risk factors as part of the history is very important.
Common sites for BSI are most frequently in the lower extremity and include the tibia, fibula, tarsals and metatarsals, calcaneus, and femur.
When considering this in an ED setting, image the involved area and if there is no fracture, advise discontinuing the activity until time of PCP/sports medicine follow up. For those with rest pain, pain with minimal weight bearing or in whom a fracture was suspected but not present, consider providing a walking boot or crutches.
BSIs occur more frequently in young athletes than in adults.
Almost 50% of BSIs occur in those younger than 20 years of age
Primary care and sports medicine providers are seeing more of these patients due to many factors.
Year-round training, sports specialization at younger ages and increase in training intensity/duration contribute to the increase incidence in adolescents.
Not surprisingly, participation in organized sports as an adolescent is a known risk factor.
Just as a change in sporting level from high school to college is a known risk factor for BSI, young “gifted” athletes who are promoted to competing with the varsity team may be at similar risk.
Shin pain lasting more than 4 weeks may represent a unique subset of MSK pain complaints increasing risk of BSI.
A prior history of BSI is a strong predictor of future BSI.
Inquire about night pain, pain with ambulation, and pain affecting performance.
Athletes with BSIs have a significantly lower BMI than controls (<21.0 kg/m2).
Athletes with BSIs sleep significantly less than controls.
Athletes with BSIs have significantly lower dairy intake than controls.
Inquire about components of the female athlete triad (low energy availability, menstrual dysfunction and low bone mineral density)
Nussbaum et al., 2019. Identifying Factors That Contribute to Adolescent Bony Stress Injury in Secondary School Athletes: A Comparative Analysis With a Healthy Athletic Control Group. Sports Health.
Category: Orthopedics
Keywords: shoulder, overhead athlete (PubMed Search)
Posted: 7/13/2019 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Long head of biceps tendon (LHBT) Testing
Overhead activities can cause anterior shoulder pain due to LHBT instability. A review of 3 physical exam maneuvers for bedside evaluation.
Speed test
Shoulder at 90° of flexion with arm fully supinated and elbow extended
Patient attempts to fwd. elevate arm against a downward force
Positive test is pain localized to bicipital groove.
Sensitivity 54% and specificity 81% for biceps pathology
Yergason test
Elbow at 90° of flexion with arm fully pronated and held against thoracic wall. Examiner grips patient’s hand and resists attempts at supination.
Positive test is pain localized to bicipital groove or LHBT subluxation.
Sensitivity 41% and specificity 79% for biceps pathology
Upper Cut test
Shoulder neutral with Elbow at 90° of flexion, arm fully supinated and hand in a fist. Patient moves hand toward chin in an uppercut motion like a boxer. Examiner places hand over patient’s fist and resists upward movement.
Positive test is pain localized to bicipital groove or LHBT subluxation.
Sensitivity 73%, specificity 78%, +LR 3.38 for biceps pathology
Comprehensive Examination of the Shoulder. Cotter et al., 2018. Sports Health
Category: Orthopedics
Keywords: Disc, infection, back pain (PubMed Search)
Posted: 6/22/2019 by Brian Corwell, MD
(Updated: 5/22/2026)
Click here to contact Brian Corwell, MD
Children are prone to inflammation and infection of the intervertebral discs
-Mean age 3-5years at presentation.
Lumbar region frequently involved
Although disc biopsy is not necessary for diagnosis, as many as 60% of biopsied discs grow bacteria
-Usually Staphylococcus aureus.
Untreated - may spontaneously resolve or progress to vertebral osteomyelitis or abscess
Chief complaint: Back pain and irritability, often associated with a limp or refusal to crawl or walk.
Fever is absent or low grade.
Physical examination findings are nonspecific and may include a tendency to lie still and percussion tenderness over the involved spine.
Blood culture is generally sterile,
WBC count can be normal early in the disease course
However, the ESR is elevated in >90% of patients.
Plain radiographs are normal at the start of the illness, and generally take 2-3 weeks to demonstrate narrowing of the intervertebral space.
Therefore imaging study of choice is MRI.
Fernandez M, et al. Discitis and vertebral osteomyelitis in children: an 18-year review. Pediatrics 2000.
Category: Orthopedics
Keywords: Spine, Autonomic Dysfunction (PubMed Search)
Posted: 6/8/2019 by Brian Corwell, MD
(Updated: 5/22/2026)
Click here to contact Brian Corwell, MD
Acute transverse myelitis (ATM) refers to inflammation of gray and white matter in one or more adjacent spinal cord segments leading to acute/subacute dysfunction of all cord functions (i.e., motor, sensory, and autonomic).
There is a bimodal peak between ages 10-19 years and ages 30-39 years.
Most cases are idiopathic
Some patients may have had a preceding viral infection or autoimmune disorder.
The thoracic cord is most commonly involved.
Onset is characterized by acute/subacute development of neurologic signs and symptoms consistent with motor weakness, sensory changes or autonomic dysfunction.
Pain in the head, neck, and/or back may occur.
Motor and sensory changes occur below the level of the lesion and are more likely to be bilateral.
Motor symptoms include a rapidly progressing paraparesis.
Autonomic dysfunction may include urinary urgency or difficulty voiding, bowel or bladder incontinence, tenesmus, constipation, and sexual dysfunction.
Despite its low incidence, consider in a patient presents with a classic constellation of symptoms,
Rapid identification, and early initiation of treatment predicts the best outcomes
Diagnosis: whole spine MRI with and without gadolinium
Management: goals include reducing cord inflammation (IV glucocorticoids), alleviating symptoms (pain management, bladder decompression), and treating underlying causes (e.g., infections, autoimmune) as appropriate.
Category: Orthopedics
Keywords: cancer, pediatrics (PubMed Search)
Posted: 5/25/2019 by Brian Corwell, MD
(Updated: 5/22/2026)
Click here to contact Brian Corwell, MD
Bone tumors can present as MSK pain!
Pain may be activity related initially (can lead to misdiagnosis)
Over time will progress to rest pain and night pain
1) Primary osteosarcoma - most common primary malignant bone tumor
Adolescents, male > female
70% occur about the knee (also in hip/pelvis and upper arm)
pain, swelling, tenderness to palpation
Consider in the presentation of non traumatic knee pain!
2) Ewing's sarcoma
Peak incidence ages 10-20, male > female
pain, swelling, tendernes to palpation
Elevated temps and ESR
Consider in the differential of osteomyelitis!!
Variable location - lusually the extremities but also pelvis, scapula, ribs
Category: Orthopedics
Keywords: Rotation, Fracture, Phalanx (PubMed Search)
Posted: 5/18/2019 by Michael Bond, MD
Click here to contact Michael Bond, MD
Remember to evaluate for any rotational deformity when evaluating patients with a phalanx fracture.
The easiest way to do this is to have the patient flex all their fingers. They should all point to the scaphoid. If a finger deviates or overlaps another finger there is a rotational deformity. One should also make sure that all the nailbeds align.
This video shows how to evaluate for rotation https://www.youtube.com/watch?v=Dhp25UVn7RQ
Even if the finger is reduced otherwise, persistent rotational deformities should be referred to a hand surgeon for consideration of corrective surgery.
Category: Orthopedics
Keywords: Hyperthermia, cold water immersion (PubMed Search)
Posted: 5/11/2019 by Brian Corwell, MD
(Updated: 5/22/2026)
Click here to contact Brian Corwell, MD
The TACO method (tarp assisted cooling with oscillation)
Cold water immersion (CWI) remains the standard for cooling in exercise induced hyperthermia
A low cost alternative is modified cold water immersion.
Sometimes, monetary reasons and location venue prevent the feasibility of CWI
Benefits: fast, cheap, portable
Portable – Allows for on site location at area of collapse
Cheap: Equipment required – 3 providers, 1 tarp, 20 gallons of water and 10 gallons of ice
Fast: Average time to set up – 3.4 minutes
The TACO method – fast effective reduction in core temperatures
May be up to 75% as effective as CWI
https://www.youtube.com/watch?v=RxjP0-_RIdc
Hosokawa, Yuri et al.
Annals of Emergency Medicine , Volume 69 , Issue 3 , 347 - 352
Category: Orthopedics
Keywords: Spine infection, back pain (PubMed Search)
Posted: 3/16/2019 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Laboratory testing for Spinal Epidural Abscess
CBC
The CBC is poorly sensitive/specific
The WBC count may be nml or elevated
Left shift and bandemia may or may not be present
ESR and CRP
Sensitive but not specific
Elevated in >80% with vertebral osteomyelitis.
Reihsaus E, et al. Spinal epidural abscess: a meta-analysis of 915 patients. Neurosurg Rev 2000.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}