Bottom Line: Cervical collars can increased ICP in moderate-severe TBI. In patients with poor cerebral compliance and impaired cerebral autoregulation, even a small increase in ICP can affect cerebral perfusion.
Bottom Line: SARS-CoV has been associated with CNS involvement. Given their similar pathogenesis and finding of hyposmia in COVID-19, SARS-CoV-2 may be associated with risk of CNS involvement.
Bottom Line: Patients on warfarin or a combination of aspirin and clopidogrel have increased risk of significant intracranial injury after blunt head trauma. Aspirin or clopidogrel monotherapy do not appear to be risk factors.
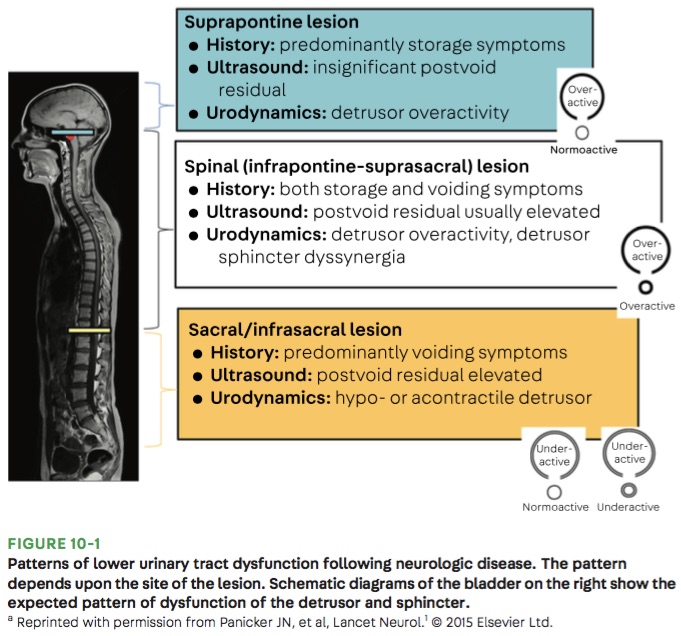
Bottom Line: Urinary retention can be seen with neurological injury involving the lower brainstem, spinal cord, cauda equina, and peripheral nerves.
Bottom Line: Fosphenytoin, valproate, and levetiracetaim have similar efficacy in treatment of benzodiazepine-resistant status epilepticus.
Bottom Line: Consider cryptococcal meningitis even in immunocompetent patients.
Bottom Line: Reduced SBP variability is associated with improved outcomes in ICH.
Bottom Line: Underdosing of benzodiazepines in status epilepticus may contribute to treatment failure.
Bottom Line: Use of IO allows more rapid administration of 23.4% NaCl with no immediate serious complications.
Bottom Line: The rate of serious neurologic conditions missed at an initial ED visit is low. However, the potential harm of misdiagnosis can be substantial.
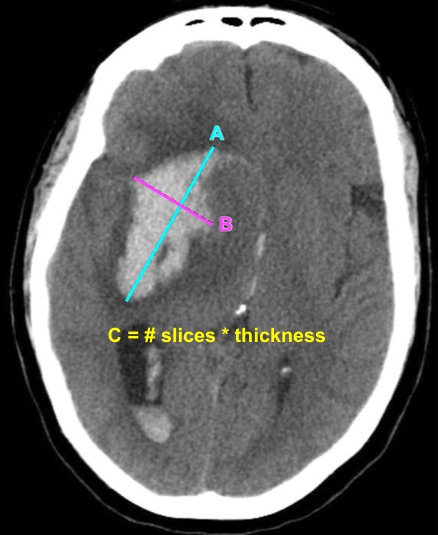
Bottom Line: EPs can reliably estimate ICH volume using the ABC/2 formula. Communicating ICH volume to neurosurgical and neurocritical care consultants can help direct treatment decisions.
Bottom Line: Consider using pre-procedural ultrasound-assistance for all lumbar punctures.
Bottom Line: ED triage nurses can safely use the Canadian C-Spine Rule. This approach can improve patient care and decrease length of stay in the ED.
Does using a combination of aspirin and clopidogrel decrease your patient’s risk of recurrent stroke after a minor ischemic stroke or high risk TIA event?
Bottom Line: The use of DAPT in minor ischemic stroke and high risk TIA reduces the risk of recurrent stroke. However, the duration of DAPT may affect the risk of major hemorrhage.
Bottom Line: LMWH appear to be similar in efficacy and safety compared with UFH for the management of CVT.
Bottom Line: Consider obtaining neuroimaging in patients presenting with syncope only if clinical features suggest probable neurological syncope.