Category: Orthopedics
Keywords: concussion, sports, head injury (PubMed Search)
Posted: 9/10/2023 by Brian Corwell, MD
(Updated: 6/17/2026)
Click here to contact Brian Corwell, MD
Sport related concussion has been estimated to affect almost 2 million children and adolescents in the United states annually
Patients who take longer than four weeks to recover are considered to have persistent post concussive symptoms
This diagnosis is associated with poor educational, social and developmental outcomes in pediatric patients
Following sport related concussion, patients are recommended to have an individualized aerobic exercise program
Prior studies have found that sub symptom threshold aerobic exercise safely and significantly speeds recovery from sport related concussion.
Purpose: This study attempted to answer whether there is a direct relationship between adherence to a personalized exercise prescription and recovery or if initial symptom burden effects adherence to the prescription.
Design: Male and female adolescents aged 13 to 18 years old presenting within 10 days of injury and diagnosed with sport related concussion.
Almost all participants (94%) sustained concussion during interscholastic games or practices.
As it is known that physician encouragement can influence patient adherence to medical interventions, treating physicians in the study were blinded to study arm assignment.
Patients were given aerobic exercise prescriptions based on their heart rate threshold at the point of exercise intolerance on a graded treadmill test
Adherence to prescription was determined objectively with heart rate monitors. No participants exercised above their prescribed heart rate intensity.
Patients who completed at least 2/3 of their aerobic exercise prescription were considered to be adherent
Results: 61% of adolescents met the adherence criterion
Adherent patients were more symptomatic and were more exercise intolerant (worse initial exercise tolerance) at their initial visit.
These patients were also more adherent than those with fewer symptoms and with better exercise tolerance. This likely indicates a stronger motivation for those more symptomatic patients to engage in a potentially effective intervention.
Adherent patients recovered faster than those who were not adherent (median recovery time 12 days versus 21.5 days (P = 0.016)
Adherence during week one was inversely related to recovery time and to initial exercise tolerance but not to initial symptom severity
Conclusion: Adherence to individualized sub symptom threshold aerobic exercise within the first week of sport related concussion is associated with faster recovery. The initial degree of exercise intolerance (but not initial symptom severity) affects adherence to aerobic exercise prescription in an adolescent population with sport related concussion
Chizuk HM, et al. Adolescents with Sport-Related Concussion Who Adhere to Aerobic Exercise Prescriptions Recover Faster. Med Sci Sports Exerc. 2022 Sep 1;54(9):1410-1416.
Category: Orthopedics
Keywords: elbow, UCL, throwing injury (PubMed Search)
Posted: 8/26/2023 by Brian Corwell, MD
(Updated: 6/17/2026)
Click here to contact Brian Corwell, MD
29 yo baseball pitcher presents with right medial elbow pain. He felt a painful “pop” and could not continue to throw (due to loss of speed and control). Also notes mild paresthesias in 4th and 5th digits.
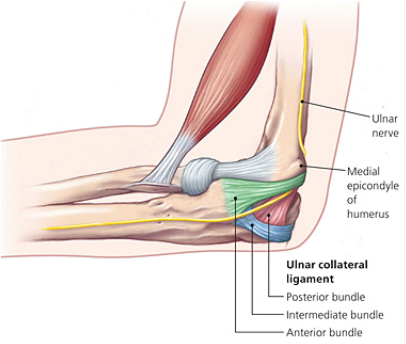
Ulnar collateral ligament (UCL) injury
Sprain of the UCL of the elbow can occur either as an acute injury or as the result of chronic excessive valgus stress due to throwing. This injury is seen in javelin throwers and baseball pitchers. Most recently, Angels superstar Shohei Ohtani suffered a torn UCL.
While traditionally this injury pattern was thought to occur in older, high-level pitchers (high velocity throwing), we are increasingly seeing this in younger athletes.
The repeated valgus stress of pitching leads to micro tearing and inflammation of the ligament. Over time, this leads to scarring and calcification and then ligament rupture.
This injury is more likely to happen in pitchers who “open up too soon” in their throwing motion. Fatigue related changes seen first in leg and core mechanics cause pitchers to open up earlier, increasing stress to the shoulder and the UCL of the elbow. Other risk factors include high velocity pitching, insufficient recovery time, and chronic overuse. The importance of proper pitching mechanics is very important as players whose pitching motion produces greater elbow valgus loads and shoulder external rotation torque are at increased risk for UCL tears.
Approximately one half of the torque generated during a fastball pitch is transmitted to the UCL. Well developed muscles about the elbow can dissipate enough energy that acute tearing is rare.
The athlete with a UCL sprain will complain of medial elbow pain that increases during the acceleration phase of throwing.
On examination, there is localized tenderness directly over the UCL:
http://www.texasshouldersurgeon.com/uploads/6/3/5/8/63580047/1446137856.png
Stress testing of the UCL causes both pain and demonstrates laxity.
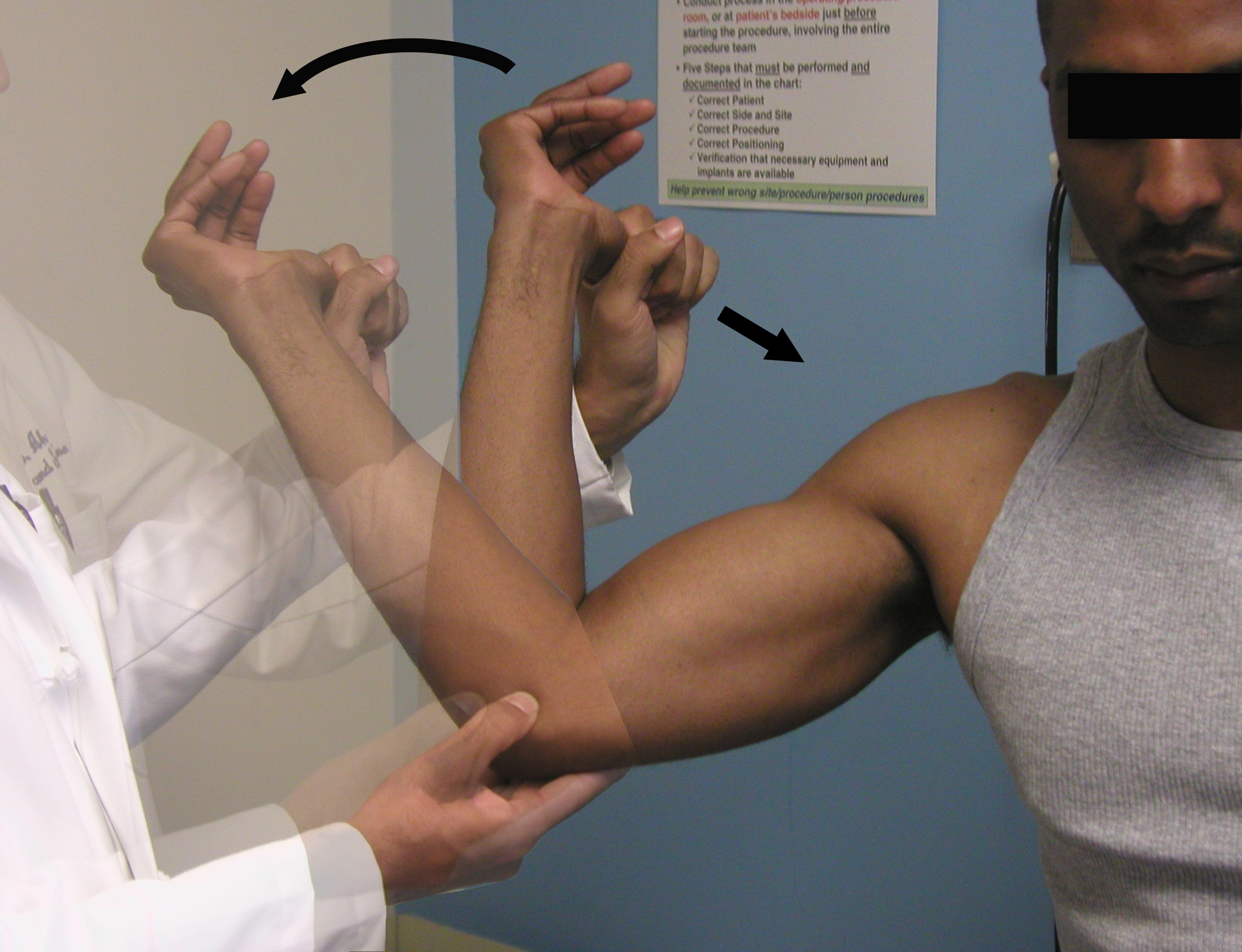
Moving Valgus Stress Test:
Place elbow in the “90/90” position. Apply a valgus stress while ranging elbow through full arc of flexion and extension. A positive test will reproduce apprehension, pain or instability at the UCL origin between 70 and 120 degrees.
https://www.youtube.com/watch?v=OnkkHpG3Dqg&ab_channel=RussHoff
Category: Administration
Keywords: Exercise, health, cardiovascular mortality (PubMed Search)
Posted: 8/12/2023 by Brian Corwell, MD
(Updated: 6/17/2026)
Click here to contact Brian Corwell, MD
The WHO and the US Department of Health and Human Services, among other groups, recommend between 150-300 minutes of moderate intensity or 75 to 150 minutes of vigorous intensity physical activity per week.
This could add up to almost 45 minutes a day!
Who has the time for that?
This is an extremely challenging goal with work and other life responsibilities.
Some recent studies asked whether routinely cramming the recommended weeks’ worth of physical activity into a couple of days, weekend warriors (WW), leads to the same life-extending benefits as distributing the exercise load throughout the week.
In a retrospective analysis of almost 90,000 individuals (56% women), providing a week of accelerometer-based physical activity data: Three activity patterns were compared: active weekend warrior (active WW, ≥150 minutes with ≥50% of total achieved in 1-2 days), active regular (≥150 minutes and not meeting active WW status), and inactive (<150 minutes).
A weekend warrior (WW) pattern of physical activity was associated with similarly lower risks of cardiovascular outcomes (incident atrial fibrillation, myocardial infarction, heart failure, and stroke) compared with more evenly distributed physical activity.
Another large prospective cohort study of over 350,000 US adults (51% women) did not find any significant difference in mortality rates between weekend warriors and regularly active participants. Compared with physically inactive participants, active participants (both weekend warrior and regularly active) had lower all-cause and cause-specific mortality rates.
Take home: Any exercise is better than none. Adults who perform 150 minutes or more of moderate to vigorous physical activity (or 75 minutes of vigorous activity) per week may experience similar health benefits whether the sessions are spread throughout the week or concentrated in a weekend.
Note: Being a weekend warrior can increase the risk of MSK complications and injury..
Future studies should include the use of wearable devices and not rely on self-reporting exercise behavior.
1. Khurshid S, Al-Alusi MA, Churchill TW, Guseh JS, Ellinor PT. Accelerometer-Derived “Weekend Warrior” Physical Activity and Incident Cardiovascular Disease. JAMA. 2023;330(3):247–252.
2. dos Santos M, Ferrari G, Lee DH, et al. Association of the “Weekend Warrior” and Other Leisure-time Physical Activity Patterns With All-Cause and Cause-Specific Mortality: A Nationwide Cohort Study. JAMA Intern Med. 2022;182(8):840–848.
Category: Orthopedics
Keywords: shoulder pain, labrum tear (PubMed Search)
Posted: 7/22/2023 by Brian Corwell, MD
(Updated: 6/17/2026)
Click here to contact Brian Corwell, MD
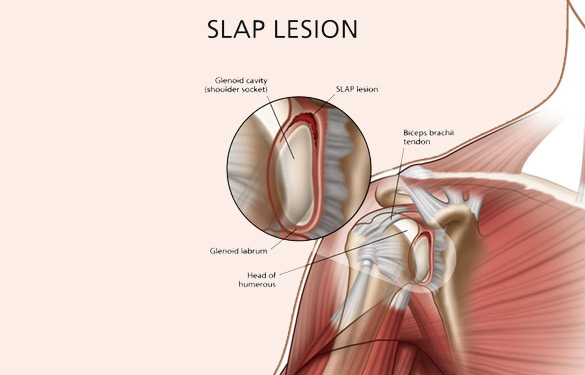
SLAP tear/lesion – Superior labral tear oriented anterior to posterior
Glenoid labrum – A rim of fibrocartilaginous tissue surrounding the glenoid rim, deepening the “socket” joint.
Integral to shoulder stability.
https://aosm.in/storage/2019/05/ch-shoulder-slap.jpg
O’Brien’s test aka active compression test for superior labral pathology.
2 parts – generally performed with the patient standing.
The patient’s shoulder is raised to 90 degrees with full elbow extension and approximately 30 degrees of adduction across the midline.
Resistance is applied, using an isometric hold.
Test in both full internal and external rotation
-This alters the position and rotation of the humerus against the glenoid
A positive test is when pain is elicited when the shoulder is in internal rotation with forearm pronation (thumb to floor) and much less or no pain when in external rotation (supination).
Note: AC joint pain may test similarly but will localize to different area of shoulder
The presence of similar, reproducible deep and diffuse glenohumeral joint pain is most indicative of a true positive test.
https://i0.wp.com/musculoskeletalkey.com/wp-content/uploads/2020/03/f50-02-9780323287845.jpg?w=960
Category: Orthopedics
Keywords: blurry vision, head trauma (PubMed Search)
Posted: 7/8/2023 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Multiple vision disorders may occur after concussion including injury to the systems that control binocular vision including: Convergence insufficiency and Accommodation insufficiency
In order to obtain a single binocular vision, simultaneous movement of both eyes in opposite directions is required.
To look at an object close by such as when reading, the eyes must rotate towards each other (convergence).
Convergence insufficiency is the reduced ability to converge enough for near vision and is a common visual dysfunction seen after concussion.
One of both eyes may also turn outward.
May lead to complaints with reading such as diplopia, blurry vision, eyestrain, and skipping words or losing one's place.
Patient or parent may also report other difficulties such as becoming more easily fatigued when reading, needing to squint and/or having disinterest in reading.
Take home: consider testing convergence in patients with some of these complaints in setting of acute or subacute head trauma.
Master CL, Bacal D, Grady MF, Hertle R, Shah AS, Strominger M, Whitecross S, Bradford GE, Lum F, Donahue SP; AAP SECTION ON OPHTHALMOLOGY; AMERICAN ACADEMY OF OPHTHALMOLOGY; AMERICAN ASSOCIATION FOR PEDIATRIC OPHTHALMOLOGY AND STRABISMUS; and AMERICAN ASSOCIATION OF CERTIFIED ORTHOPTISTS. Vision and Concussion: Symptoms, Signs, Evaluation, and Treatment. Pediatrics. 2022 Aug 1;150(2):e2021056047.
Category: Administration
Keywords: concussion recovery (PubMed Search)
Posted: 6/24/2023 by Brian Corwell, MD
(Updated: 6/17/2026)
Click here to contact Brian Corwell, MD
How much screen time after concussion?
Adolescents spent more than 7 hours daily on screen time during the pandemic.
Historically, experts recommended screen time abstinence to various degrees after concussion.
Prior study: RCT of concussion patients (ages 12 to 25) found that those who abstain from screen time for the first 48 hours recovered 4.5 days sooner than those who were permitted screen time.
Population: 633 children and adolescents with acute concussion and 334 with orthopedic injuries aged 8 to 16, recruited from 5 Canadian pediatric emergency departments.
Post concussion symptoms were measured at 7 to 10 days, weekly for three months, and biweekly for three to six months post injury. Screen time was measured.
Results: Screen time was a significant predictor of post concussion symptom recovery with both parent reported somatic and self-reported cognitive symptoms.
There may be an effect of low to moderate screen time (Goldilocks effect) demonstrating that those in the 25th to 50th percentiles had less severe symptoms than those on the higher end of screen time use or those who minimally use of screens!
Low and high screen time were both associated with relatively more severe symptoms in the concussion group compared to the orthopedic injury group during the first 30 days post recovery but not after 30 days.
Conclusion: The association of early screen time with post concussion symptoms is not linear. Recommending moderation in screen time may be the best approach to clinical management.
Children need to strike a balance between avoiding boredom, deconditioning, isolation, and overexerting themselves physically or cognitively.
Cairncross M, al. Early Postinjury Screen Time and Concussion Recovery. Pediatrics. 2022
Category: Orthopedics
Keywords: shoulder, Adhesive capsulitis (PubMed Search)
Posted: 6/10/2023 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Adhesive capsulitis aka frozen shoulder
Definition: Gradual development of global limitation of both active and passive shoulder motion, characterized by severe pain and lack of radiographic findings
Idiopathic loss of BOTH active and passive motion (significant reduction of at least 50%)
Motion is stiff and painful especially at the extremes.
Occurs due to thickening and contracture of the shoulder capsule.
Affects up to 8-10% of people of working age.
Affects patients between the ages of 40 and 60.
Peak age mid 50s
Onset before 40 is rare (consider other diagnosis).
Affects women more than men.
Diabetes is the most common risk factor.
Patients with DM, suffer a more prolonged course and are more resistant to therapy
Also associated with thyroid disease and prolonged immobilization
Increased risk following trauma to shoulder region (rotator cuff tear, following shoulder surgery, fracture of proximal humerus)
Presents unilaterally (other shoulder may become involved in next 5 years)
Slight increased risk of non-dominant shoulder
Category: Orthopedics
Keywords: overuse injury, wrist (PubMed Search)
Posted: 5/25/2023 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Intersection syndrome
Intersection syndrome is an overuse injury of the forearm.
Pain is located approximately 2 finger breaths (4cm) proximal to the wrist joint.
https://www.sportsmedreview.com/wp-content/uploads/2020/11/intersectionsyndrome.png
Mechanism: friction is caused by repetitive wrist extension activities
Commonly: Rowing, skiing, tennis, canoeing and weightlifting
Friction may cause crepitus with finger/wrist extension.
Tenderness, mild swelling may be present
Category: Orthopedics
Keywords: Baker's cyst, knee, effusion (PubMed Search)
Posted: 5/13/2023 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
A Baker's cyst is a common incidental finding on ultrasound reports and bedside physical exam.
Clinically, these cysts are commonly found in association with intra-articular knee disorders. Most commonly: osteoarthritis, RA and tears of the meniscus.
Sometimes Baker's cysts are a source of posterior knee pain.
In an orthopedic clinic setting, Baker’s cysts are frequently discovered on routine MRI in patients with symptomatic knee pain. They tend to occur in adults from ages 35 to 70.
Over 90% of Baker’s cysts are associated with an intraarticular knee disorder. While most frequently associated with OA and meniscal tears, other knee pathologies that have been associated include inflammatory arthritis and tears of the anterior cruciate ligament.
DDX: DVT, cystic masses (synovial cyst), solid masses (sarcoma) and popliteal artery aneurysms.
Based on cadaveric studies, a valvular opening of the posterior capsule, proximal/medial and deep to the medial head of the gastrocnemius is present in approximately 50% of healthy adult knees.
Fluid flows in one way from knee joint to cyst and not in reverse. This valve allows flow only during knee flexion as it is compressed shut during extension due to muscle tension.
Most common patient complaint is that of the primary pathology, meniscal pain for example. At times, symptoms related to the cyst are likely due to increasing size as they may report fullness, achiness, stiffness.
In one small study, the most common symptoms were 1) popliteal swelling and 2) posterior aching. Patients may complain of loss of knee flexion from an enlarged cyst that can mechanically block full flexion.
If the Baker cyst is large enough the clinician will feel posterior medial fullness and mild tenderness to palpation. The cyst will be firm and full knee extension and softer during the flexion (Foucher’s sign).
This may help with differentiation from other popliteal masses (hematoma, soft tissue tumor, popliteal artery aneurysm).
With cyst rupture, severe pain can simulate thrombosis or calf muscle rupture, (warmth, tenderness, and erythema). A ruptured cyst can also produce bruising, which may involve the posterior calf starting from the popliteal fossa and extending distally towards the ankle.
Treatment: initial treatment for symptomatic Baker cysts is nonoperative unless vascular or neural compression is present (very unlikely)
Treatment involves physical therapy to maintain knee flexibility. A sports medicine physician may perform an intraarticular knee corticosteroid injection as this has been found to decrease size and symptoms of cysts in two-thirds of patients.
For patients that fail above, refer for surgical evaluation. Inform patients that they are not undergoing ED drainage of this symptomatic cyst due to the extremely high rate of recurrence which, as a result of the ongoing presence of the untreated intraarticular pathology, results in the recurrent effusion.
Category: Orthopedics
Keywords: lower back pain, analgesia, NSAIDs (PubMed Search)
Posted: 4/8/2023 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Acute lower back pain is a very common emergency department presenting complaint. Over the last several years there has been impetus to move away from opioids in the management of lower back pain.
A recent systematic review investigated the pharmacologic management of acute low back pain. This review looked at RCTs investigating the efficacy of muscle relaxants, NSAIDs, and acetaminophen for the treatment of acute nonspecific lower back pain of fewer than 12 weeks duration in patients > 18 years of age. Studies that investigated the use of opioids were not considered.
18 RCTs, totaling 3478 patients were included. 54% were women. The mean patient age was 42.5 ± 7.3 years. The mean length of follow-up was 8.0 ± 5.6 days. The mean duration of symptoms before treatment was 15.1 ± 10.3 days.
Results: Muscle relaxants and NSAIDs were effective in reducing pain and disability in acute LBP at approximately 1 week.
The combination of NSAIDs and acetaminophen was associated with a greater improvement than the sole administration of NSAIDs.
However, acetaminophen alone did not promote any significant improvement. Placebo administration was not effective.
Limitations: Most patients with acute LBP experience spontaneous recovery or at least reduction of symptoms, therefore, the real impact of most medications is uncertain. The present study wasn't able to distinguish among different classes of NSAIDs. A best practice treatment protocol cannot be extrapolated from this study.
Take home: In my practice, patients are treated with NSAIDs and Acetaminophen first line. I also include Licocaine patches for all patients. If there is a contraindication to NSAIDs, I treat with muscle relaxants alone.
This study highlights the lack of benefit of acetaminophen as mono therapy (which has been noted in other studies).
Baroncini A, et al. Nonopioid pharmacological management of acute low back pain: A level I of evidence systematic review. J Orthop Res. 2023 Feb 22. doi: 10.1002/jor.25508.
Category: Orthopedics
Keywords: knee pain, running injury (PubMed Search)
Posted: 3/25/2023 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
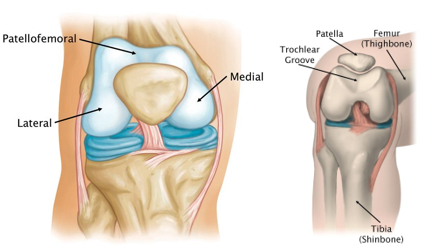
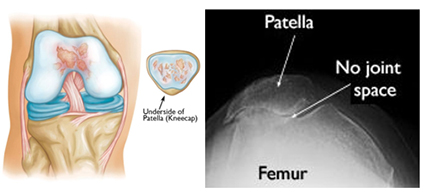
Patellofemoral anatomy and disease (part 1)
During normal knee flexion, the patella slides within the trochlear grove. Both (patella and the trochlear groove) are lined with articular cartilage at the patellofemoral articulation.
https://www.stvincentsboneandjoint.com.au/images/patellofemoral-joint2.jpg
Multiple forces act on the patella which can affect proper tracking: Proximately, by the quadriceps tendon, distally, by the patellar tendon, medially, by the medial retinaculum/vastus medialis and laterally by the lateral retinaculum and the vastus lateralis.
Patellofemoral OA can occur when this cartilage starts to wear and can be seen in skyline/sunrise/notch or equivalent views. OA here rarely occurs in isolation (<10%) and is usually part of medial or lateral knee OA.
https://www.stvincentsboneandjoint.com.au/images/patellofemoral-joint3.jpg
Patellofemoral pain is usually from overuse/training overload or malalignment.
Contributors to overuse involve total joint load which may have influence from training volume (total miles), intensity (competitive sports) in addition to BMI (>25) in addition to overall fitness level.
Malalignment aka abnormal patellar tracking involves both static (leg length discrepancy, hamstring tightness, etc.) and dynamic components (hip weakness, gluteus medius weakness, excessive foot pronation, etc.).
Patients with anterior knee pain should have activity modification, ice, NSAIDs (not steroids) and long-term engagement in physical therapy (>6 months) with a focus on flexibility and strengthening of lower extremity kinetic chain including the vastus medialis, gluteus medius, hip external rotators and core.
Also, consider looking for hyper supination or pronation. Foot orthotics can be of help with this.
Category: Orthopedics
Keywords: wrist pain (PubMed Search)
Posted: 2/25/2023 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
21-year-old college softball player presents for evaluation of Left hand/wrist pain following batting practice.
She states her pinky is “tingly”
On exam, there is tenderness over her volar ulnar wrist.
You obtain an X-ray.
https://prod-images-static.radiopaedia.org/images/52314027/a662d8f338ec08ba56178463638d25_jumbo.jpeg
What’s the diagnosis?
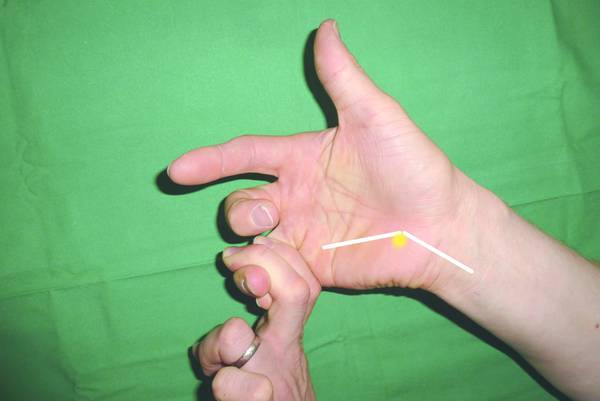
Hook of the hamate fractures are often associated with sports that require a firm hand grip such as baseball, softball, tennis, golf. These sports cause repeated stress against the hamate bone from the gripped sporting equipment. A frequent mechanism is grounding a golf club or from the act of checking a baseball bat swing.
On physical exam, the most common finding is focal tenderness over the hook of the hamate.
Another test with high sensitivity is a hook of the hamate pull test
Place the patient's hand in ulnar deviation and ask patient to flex the DIP joints of the 4th and 5th digits against resistance.
https://musculoskeletalkey.com/wp-content/uploads/2016/06/9783131746214_006_002.tif_epub1.jpg
Imaging: PA and lateral wrist views are frequently negative despite being the first line recommended imaging for wrist pain/trauma.
A carpal tunnel view has much better sensitivity to visualize the hook of the hamate.
Base fractures (less common than hook) may also be missed on carpal tunnel view and require advanced imaging using CT.
Place patient in ulnar gutter splint and arrange follow up with hand surgery.
Overall, this is an uncommon though frequently missed injury. Consider the above mentioned physical exam and imaging recommendations to improve diagnostic accuracy.
Category: Orthopedics
Keywords: concussion recovery, head injury, post concussive syndrome (PubMed Search)
Posted: 2/11/2023 by Brian Corwell, MD
(Updated: 6/17/2026)
Click here to contact Brian Corwell, MD
Prolonged post-concussion symptoms are loosely defined as those lasting more than three or four weeks versus typical recovery, typically between 10-14 days.
Athletes who take longer than "typical” to recover have a challenging road of uncertainty. Medical providers are asked to make informed decisions about “normal” and expected return based on limited information.
Evaluating both athlete and parental expectations is challenging, especially when navigating difficult conversations about medical disqualification and permanently discontinuing their sport.
A 2016 study of approximately 50 patients with sports-associated concussion who had persistent symptoms lasting greater than one-month found that a collaborative multidisciplinary treatment approach was associated with significant reduction in post concussive symptoms at six months versus usual treatment.
A recent 2023 study in Neurology provides additional good news for athletes who are slow to recover from sports associated concussion. Approximately 1750 concussed collegiate athletes (diagnosed by team physician) were enrolled. In this study, slow recovery was defined as taking more than 14 days for symptoms to resolve OR taking more than 24 days to return to sport.
Approximately 400 athletes met the criteria for slow recovery (23%).
Male athletes participated primarily in football, soccer, and basketball.
Female athletes participated primarily in soccer, basketball, and volleyball.
Of the athletes who took longer than 24 days to return to play:
77.6% were able to return to play within 60 days of injury,
83.4% returned to play within 90 days, and
10.6% did not return to play at 6 months.
Slow to recover athletes averaged 35 days after injury for return to play.
This study provides valuable information for medical providers: There is an overall favorable prognosis for slow to recover concussed athletes for return to school and sport.
McAllister TW,et al; Concussion Assessment, Research and Education (CARE) Consortium. Characteristics and Outcomes of Athletes With Slow Recovery From Sport-Related Concussion: A CARE Consortium Study. Neurology. 2023 Jan 18:10.1212
Category: Misc
Keywords: hydration, mortality (PubMed Search)
Posted: 1/28/2023 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
In a recent study in The Lancet, researchers at NIH attempted to test the hypothesis that optimal hydration may slow down the aging process.
A large proportion of people do not consume the recommended fluid amounts. This has likely become worse with our masking during the pandemic.
Previous studies in a mouse model showed that water restriction, increasing serum sodium by 5 mmol/l, shortened the mouse lifespan by 6 months which corresponds to about 15 years of human life.
Population: Data from Atherosclerosis Risk in Communities (ARIC) study: an ongoing population-based prospective cohort study in which 15,792 45-66 year-old black (African American) and white men and women were enrolled from four US communities in 1987–1989 and followed up for more than 25 years.
Variables: 15 biomarkers and serum sodium (as a proxy for the hydration habits of study participants).
They attempted to exclude people whose serum sodium could be affected by factors other than the amount of liquids they consume. After these exclusions, 11,255 participants remained in the datase.
Authors also calculated ones biologic age by sampling 15 biomarkers characterizing performance of multiple organ systems and processes: cardiovascular (systolic blood pressure), renal (eGFR, cystatin-C, urea nitrogen, creatinine, uric acid), respiratory (FEV), metabolic (glucose, cholesterol, HbA1c, glycated albumin, fructosamine), immune/inflammatory (CRP, albumin, beta 2-microglobulin).
Conclusions: The analysis showed that middle age serum sodium >142 mmol/l is associated with a 39% increased risk to develop chronic diseases (hazard ratio [HR] = 1.39, 95% confidence interval [CI]:1.18–1.63) and >144 mmol/l with 21% elevated risk of premature mortality (HR = 1.21, 95% CI:1.02–1.45). People with serum sodium >142 mmol/l had up to 50% higher odds to be older than their chronological age (OR = 1.50, 95% CI:1.14–1.96).
Limitations: Observational study. No firm conclusions without intervention studies.
Summary: Serum sodium concentration exceeding 142 mmol/l is associated with increased risk to be biologically older, develop chronic diseases and die at younger age.
Take home: Drink more water
Dmitrieva NI, Gagarin A, Liu D, Wu CO, Boehm M. Middle-age high normal serum sodium as a risk factor for accelerated biological aging, chronic diseases, and premature mortality. EBioMedicine. 2023 Jan;87:104404.
Category: Misc
Keywords: Aging, mortality, physical activity (PubMed Search)
Posted: 1/14/2023 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Humor me and imagine that your birth certificate vanished, and your age was based on the way you feel inside. How old would you say you are (subjective age) versus your actual age?
In a few studies, those individuals reporting a younger subjective age had a lower risk of depression, greater mental well-being, better physical health, and a lower risk of dementia. These individuals also had improved episodic memory and executive functioning. Subjective age also predicts incident hospitalization.
Three longitudinal studies tracked more than 17,000 middle aged and elderly individuals.
Over a 20-year period, researchers tracked: Subjective age, demographic factors, disease burden, functional limitations, depressive symptoms, and physical inactivity.
Researchers found that those who felt approximately 8, 11, and 13 years older than their actual age had an 18%, 29%, and 25% higher risk of mortality, respectively. They also had a greater disease burden even after controlling for demographic factors such as education, race and marital status. Multivariable analyses showed that disease burden, physical inactivity, functional limitations, and cognitive problems, but not depressive symptoms, accounted for the associations between subjective age and mortality.
This study provides evidence for an association between an older subjective age and a higher risk of mortality across adulthood. These findings support the role of subjective age as a biopsychosocial marker of aging. This may allow for early intervention for select individuals who may have a higher association with poor health outcomes.
Your subjective age can better predict your overall health than the date on your birth certificate.
Stephan Y, Sutin AR, Terracciano A. Subjective Age and Mortality in Three Longitudinal Samples. Psychosom Med. 2018 Sep;80(7):659-664.
Category: Pharmacology & Therapeutics
Keywords: dietary supplements, complementary nutritional products (PubMed Search)
Posted: 12/24/2022 by Brian Corwell, MD
(Updated: 6/17/2026)
Click here to contact Brian Corwell, MD
Over half of U.S. adults in the United States consume dietary supplements.
Study design: A quality improvement study using data from the FDA’s Center for Drug Evaluation and Research, Tainted Products Marketed as Dietary Supplements
Dates: 2007 through 2016.
Results: Unapproved pharmaceutical ingredients were identified in 776 dietary supplements.
146 different dietary supplement companies were involved.
Most of these products were marketed for sexual enhancement (353 [45.5%]), weight loss (317 [40.9%]), or muscle building (92 [11.9%].
157 adulterated products (20.2%) contained more than 1 unapproved ingredient.
A 2015 NEJM study estimated that 23,000 ED visits per year are attributed to adverse effects associated with dietary supplements.
Estimated 2154 hospitalizations annually.
Frequently involve young adults between 20 and 34 years of age in addition to unsupervised children.
Excluding children, almost 66% of ED visits involve herbal or complementary nutritional products and 31.8% involved micronutrients.
Products for weight loss or increased energy were commonly implicated.
Finally, herbal and dietary supplements now account for 20% of cases of hepatotoxicity in the US.
The major implicated agents include anabolic steroids, green tea extract, and multi-ingredient nutritional supplements.
Anabolic steroids (marketed as bodybuilding supplements) typically induce a prolonged cholestatic, self-limiting liver injury.
Green tea extract and many other products, in contrast, tend to cause an acute hepatitis like injury.
Tucker J, et al. Unapproved Pharmaceutical Ingredients Included in Dietary Supplements Associated With US Food and Drug Administration Warnings. JAMA Netw Open. 2018;1(6).
Geller et al. Emergency Department Visits for Adverse Events Related to Dietary Supplements. N Engl J Med 2015;373: 1531-1540.
Navarro VJ, et al. Liver injury from herbal and dietary supplements. Hepatology. 2017 Jan;65(1):363-373.
Category: Orthopedics
Keywords: exercise, death, physical activity (PubMed Search)
Posted: 12/10/2022 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
"The Tortoise and the Hare" fable has been used as a metaphor for the epidemiological differences between slower, low-intensity exercise versus faster, high-intensity physical activity.
"Current physical activity recommendations are predicated on the idea that both the hare and the tortoise can win the race for better health, but the provocative studies give an edge to the hare's higher-intensity approach,"
Regular physical activity is associated with significant health benefits, including decreased risk of cardiovascular disease, cancer, and all-cause mortality.
Traditional research has focused on exercise volume (150 minutes/week) over intensity.
Two recent studies looked at the benefits of shorter bouts of vigorous activity at higher intensities.
A recent large population-based cohort study of middle-aged adults used objective measurement of activity (wrist accelerometer) over self-reporting to investigate the role of exercise intensity and CV health.
Higher intensity physical activity is associated with lower rates of incident CVD.
This makes theoretical sense as greater stimulation will result in greater physiologic CV adaptations resulting in overall improved CV fitness.
For example. the authors extrapolate that an ambling 14-minute stroll has roughly the same cardiovascular benefits as an up-tempo 7-minute walk at a brisk pace.
Increasing the total amount of activity is not the only means of achieving health goals which can be met with raising overall intensity.
Vigorous physical activity is a time-efficient means to achieve overall health benefits of exercise.
A recent study (Ahmadi et al., 2022) involved 71,893 older adults with a mean age of 62.5. Authors found that quick bursts of vigorous physical activity throughout the day can lower older adults' risk of premature death by 16% to 27%, depending on daily frequency and weekly totals (from 15-20 min/week up to 50-57 min/week).
For example, doing one two-minute burst of high-intensity exercise every day for a total of 14 minutes per week was associated with an approximately 18% lower risk of all-cause mortality. The authors also found that doing as little as one to nine minutes per week of vigorous activity in quick bursts versus doing no vigorous activity was associated with significantly lower all-cause mortality risk over five years.
Exercise may not need to be a planned hour-long session at the gym for our middle-aged and older population. Accruing small amount sporadically over the day/week is an attractive option to reap the CV benefits of exercise. Existing exercise guidelines will need to be modified with future research to pinpoint the optimal exercise intensity and duration for adults in different stages of life.
Dempsey et al., 2022. Physical activity volume, intensity, and incident cardiovascular disease, European Heart Journal, Volume 43.
Ahmadi et al., 2022. Vigorous physical activity, incident heart disease, and cancer: how little is enough?, European Heart Journal, Volume 43, Issue 46
Category: Orthopedics
Keywords: Pet ownership, cardiovascular health, risk reduction (PubMed Search)
Posted: 11/25/2022 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Dog ownership has become more common especially during the pandemic.
Almost 70% of US households own a pet and almost half own ≥1 dogs.
There are many health benefits associated with dog ownership including: reduced risk of asthma and allergic rhinitis in children exposed to pets during early ages, improvement in symptoms of PTSD, overall wellbeing & alleviation of social isolation in elderly individuals and increased physical activity.
The main positive impact of dog ownership seems to be in relation to cardiovascular risk including an association with lower blood pressure levels, improved lipid profile, and diminished sympathetic responses to stress.
Study: A systematic review and meta-analysis (10 studies, over 3 million participants) to evaluate the association of dog ownership with all-cause mortality, with and without prior cardiovascular disease, and cardiovascular mortality. Mean follow up 10 years.
Results: Dog ownership was associated with a 24% risk reduction for all-cause mortality as compared to non-ownership (relative risk, 0.76; 95% CI, 0.67–0.86) with 6 studies demonstrating significant reduction in the risk of death.
In individuals with prior coronary events, dog ownership was associated with an even more pronounced risk reduction for all-cause mortality (relative risk, 0.35; 95% CI, 0.17–0.69). When authors restricted the analyses to studies evaluating cardiovascular mortality, dog ownership conferred a 31% risk reduction for cardiovascular death (relative risk, 0.69; 95% CI, 0.67–0.71).
The cause of this benefit is unclear. Though some activities such as the act of petting a dog has been observed to lower blood pressure levels, the mechanism for the longer survival is likely through enhanced physical activity provided by dog walking.
Conclusion: Dog ownership is associated with reduced all-cause mortality likely driven by a reduction in cardiovascular mortality. Dog ownership as a lifestyle intervention may offer significant health benefits, particularly in populations at high-risk for cardiovascular death.
Finally, meet Winston, a French bulldog who, last night, won the National Dog Show!
Category: Orthopedics
Keywords: musculoskeletal pain, analgesia, opioids (PubMed Search)
Posted: 11/12/2022 by Brian Corwell, MD
(Updated: 6/17/2026)
Click here to contact Brian Corwell, MD
Opioids & NSAIDs for MSK pain in the ED: Effectiveness and Harms
Study selection: A recent systematic review in Annals of Internal Medicine attempted to evaluate the effectiveness and harms of opioids for musculoskeletal pain in the emergency department.
Included were RCTs of any opioid analgesic as compared with placebo or a nonopioid analgesic.
Conditions studied: bone injuries, soft tissue injuries, spinal pain, and mixed presentations.
Out of 2464 articles, they included 42 trials (n=6128).
Effectiveness data: Opioids were statistically but not clinically more effective in reducing pain in the short term (approximately 2 hours) versus placebo and Tylenol but were not clinically or statistically more effective than NSAIDs.
Take home: Opioids and NSAIDs may have about the same pain outcomes.
Harm data: The results on harms were very mixed. Overall, there were fewer harms with NSAIDs than opioids. However, many studies showed less of a difference. The benefit with NSAIDs due to fewer harms may be less in patients with mixed musculoskeletal conditions.
Opioids may carry higher risk for harms than placebo, Tylenol, or NSAIDs. Authors also found that an increased opioid dose may increase harms from opioids.
Limitations: Limited data on long-term outcomes and longer-term pain management
Jones CMP, Lin CC, et al. Effectiveness of Opioid Analgesic Medicines Prescribed in or at Discharge From Emergency Departments for Musculoskeletal Pain: A Systematic Review and Meta-analysis. Ann Intern Med. 2022 Oct 18.
Category: Orthopedics
Keywords: hip, dislocation, DDH (PubMed Search)
Posted: 10/22/2022 by Brian Corwell, MD
(Updated: 6/17/2026)
Click here to contact Brian Corwell, MD
Developmental dysplasia of the hip (DDH)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}