ISPAD (International Society for Pediatric and Adolescent Diabetes) Updated their Guidelines for Pediatric Diabetic Ketoacidosis (DKA) in 2014
Fluids:
· Begin fluid repletion with 10-20ml/kg of 0.9% NS over 1-2 hours
· Estimate losses (mild DKA <5%, moderate 5-7%, severe ~10%) and replete evenly over 48 hours
o Use NS, Ringers or Plasmalyte for 4-6 hours
o Afterwards use any crystalloid, tonicity at least 0.45% NaCl
· Add 5% glucose to IV fluid when glucose falls below 250-300mg/dL
Insulin
· No bolus
· Low dose 0.05 - 0.1U/kg/hr AFTER initiating fluid therapy
o higher incidence of cerebral edema in patients given insulin in 1st hour
· Short acting subQ insulin lispro or aspart can be substituted for drip in uncomplicated mild DKA
· Give long acting subQ insulin at least 2 hours before stopping infusion to prevent rebound
Potassium
· If K low (< 3.3): add 40mmol/L with bolus IV fluids (20mmol/L if rate > 10ml/kg/hr)
· if K normal (3.3-5): add 40mmol/L when insulin is started
· If K high (> 5): add 40mEq/L after urine output is documented
Bicarb
· No role for bicarbonate in treatment of Pediatric DKA
o No benefit, possibility of harm (paradoxical CNS acidosis)
This study is a case control study of the association of congenital heart disease (CHD) and stroke using a base population of 2.5 million Kaiser patients in California. 412 cases of stroke were identified and compared to 1236 controls. Of these stroke patients, 11/216 ischemic strokes and 4/196 hemorrhagic strokes were attributed to CHD (both cyanotic and acyanotic lesions). CHD was found in 7/1236 controls.
Children with CHD and history of cardiac surgery had the strongest risk of stroke (31 fold over the control group). Many of these children had strokes years after their surgery. Children with CHD who did not have cardiac surgery had a trend towards elevated stroke risk, but the confidence intervals included the null. More children without CHD history presented with headache.
Bottom line: Stroke risk (both hemorrhagic and ischemic) extend past the immediate postoperative period in patients with CHD.
Pediatric Caffeine Overdose
As the in-service draws closer and the hours to study wind down, I find myself becoming more and more of a caffeine enthusiast. While a No-Doz or Diet Mt. Dew may put a little more pep in my step, the caffeine found in energy drinks, caffeine pills, and diet supplements can quickly result in an dangerous overdose in a young child.
Caffeine Overdose Presentation- Sympathomimetic Toxidrome
Available Sources of Caffeine-
Toxic Doses
Management- treat the symptoms (metabolic, cardiovascular, and neurologic)
Good Luck on the In-Service!

Of pediatric patients who have anteroposterior (AP) pelvic xrays (XR), there is a 4.6% rate of pelvic fracture or dislocation, compared to 10% in adults.
This study is a sub analysis of a prospective observational cohort of children with blunt torso trauma conducted by PECARN. 7808 patients had pelvic imaging, with 65% of them having an AP XR. The XR sensitivity ranged from 64-82% (based on age groups) for detecting fractures. All but one patient with a pelvic fracture not detected on XR had a CT scan. The CT scan detected all but 2 fractures both of which were picked up later as healing fractures on repeat pelvic XR. Some of the patients who had a missed fracture on XR were hemodynamically unstable or wound up requiring operative intervention.
The authors support the following algorithm:
-With hemodynamically unstability children, obtain a pelvic XR
-For hemodynamically stable children when the physician is planning to get a CT, there is no indication for XR
Bottom line: Consider using AP pelvic radiographs in the hemodynamically stable patient with a high suspicion for fracture or dislocation who are not undergoing CT.
Are you comfortable with Intraosseous Catheter Placement in Children during a code? A pediatric code or child in distress is also distressing to care providers. Your staff may not feel comfortable with IO access in children. Read on to be more comfortable with your options as IO access in children can be difficult, especially the chubby toddlers. The basics for a patient in distress are "IV, O2, Monitor". Access is vital to giving resuscitation medications.
Indications for IO access: Any child in whom IV access cannot readily be obtained, but is necessary.
All IOs are 15G for infusion equal to central vascular access.
Different colors indicate different sizes:
Preferred sites:
Kids-do NOT use the sternum or distal radius
The reference from NEJM has videos to review placement and different tools (manual, EZ IO, and autoinjector).
Cyanotic (right to left shunt) Congenital Heart Disease (CHD) lesions can be easily remembered with the 1,2,3,4,5 method.
1- Truncus Arteriosis (ONE trunk)
2- Transposition of the Great Vessels (TWO vessels flipped)
3- TRIcuspid Atresia
4-TETRAlogy of Fallot
5- Total Anomolous Pulmonary Venous Return (TAPVR=5 words/letters)
A few other important DUCTAL-DEPENDENT lesions: Coarctation of the Aorta, Hypoplastic Left Heart Syndrome, and Pulmonary Atresia.
Patients present to the emergency department within the first week of life in severe distress, including hypoxia, tachypnea, and hypotension. The above cyanotic CHD all reflect DUCTAL-DEPENDENT lesions, meaning they need a widely open PDA (which closes in the first week of life) to maintain sufficient oxygenation for viability.
These patients will not survive without timely intervention with prostaglandin (PGE1), so be sure to initiate this life-saving medication as soon as possible! Side effects include apnea…be prepared to intubate your neonate!
Now that respiratory season is upon us, we are faced with an increasing number of bronchiolitis children. The updated clinical practice guidelines for managing these kids were recently published and emphasize supportive care only.
Some of the key points:
-When clinicians diagnose bronchiolitis on the basis of history and physical examination, radiographic or laboratory studies should not be obtained routinely.
-Medications such as albuterol, nebulized epinephrine or steroids should not be administered routinely in children with a diagnosis of bronchiolitis.
-Nebulized hypertonic saline should not be administered to infants with a diagnosis of bronchiolitis in the emergency department
-Clinicians may choose not to administer supplemental oxygen if the oxyhemoglobin saturation exceeds 90% in infants and children with a diagnosis of bronchiolitis
-Clinicians may choose not to use continuous pulse oximetry for infants and children with a diagnosis of bronchiolitis.
Check out the full guidelines for the quality of evidence and rational behind these recommendations.
The bottom line is that not much really works, and we just need to support their respiratory effort and ensure hydration.
Dehydration is a common pediatric ED presentation. Oral rehydration (although first choice) is often not possible secondary to patient cooperation and/ or persistent vomiting. Intravenous (IV) hydration is often difficult, requiring multiple attempts especially in the young dehydrated infant.
Hyaluronan is a mucopolysaccharude present in connective tissue that prevents the spread of substances through the subcutneous space. Hyaluronidase is a human DNA-derived enzyme that breaks down hyaluronan and temporarily increases its permeability, thereby allowing fluid to be absorbed with the capillary and lymphatic systems.
In one study, patients age 1 month to 10 years were randomized to recieve 20 mL/kg bolus NS via subcutaneous (SC) or IV route over one hour, then as needed. The mean volume infused in the ED was 334.3 mL (SC) vs 299.6 mL (IV). Succesful line placement occured in all 73 SC patients and only 59/75 IV patients. There was a higher proportion of satisfaction for clinicians and parents for ease of use and satisfaction, respectively.
Bottom line: Consider subcutaneous hyaluronidase faciliated rehydration in mild to moderately dehydrated children, especially with difficult IV access.
Emergency Physician Bedside Ultrasound for Appendicitis
Why?
To reduce length of stay, improve patient care, and reduce radiation exposure in young patients.
How?
Start with pain medication so you get a better study. (Consider intranasal fentanyl for quicker pain relief and diagnostics in pediatrics.) Study results are also improved with a slim body habitus.
Place the patient supine
Use a high-frequency linear array transducer
Start at the point of maximal tenderness in the RLQ
Transverse and longitudinal planes "graded compression" to displace overlying bowel gas which usually has peristalsis (See Sivitz, et al article for images of "graded compression")
Appendix is usually anterior to the psoas muscle and iliac vein and artery as landmarks
Measure from outer wall to outer wall at the most inflamed portion of the appendix (usually distal end)
Example:
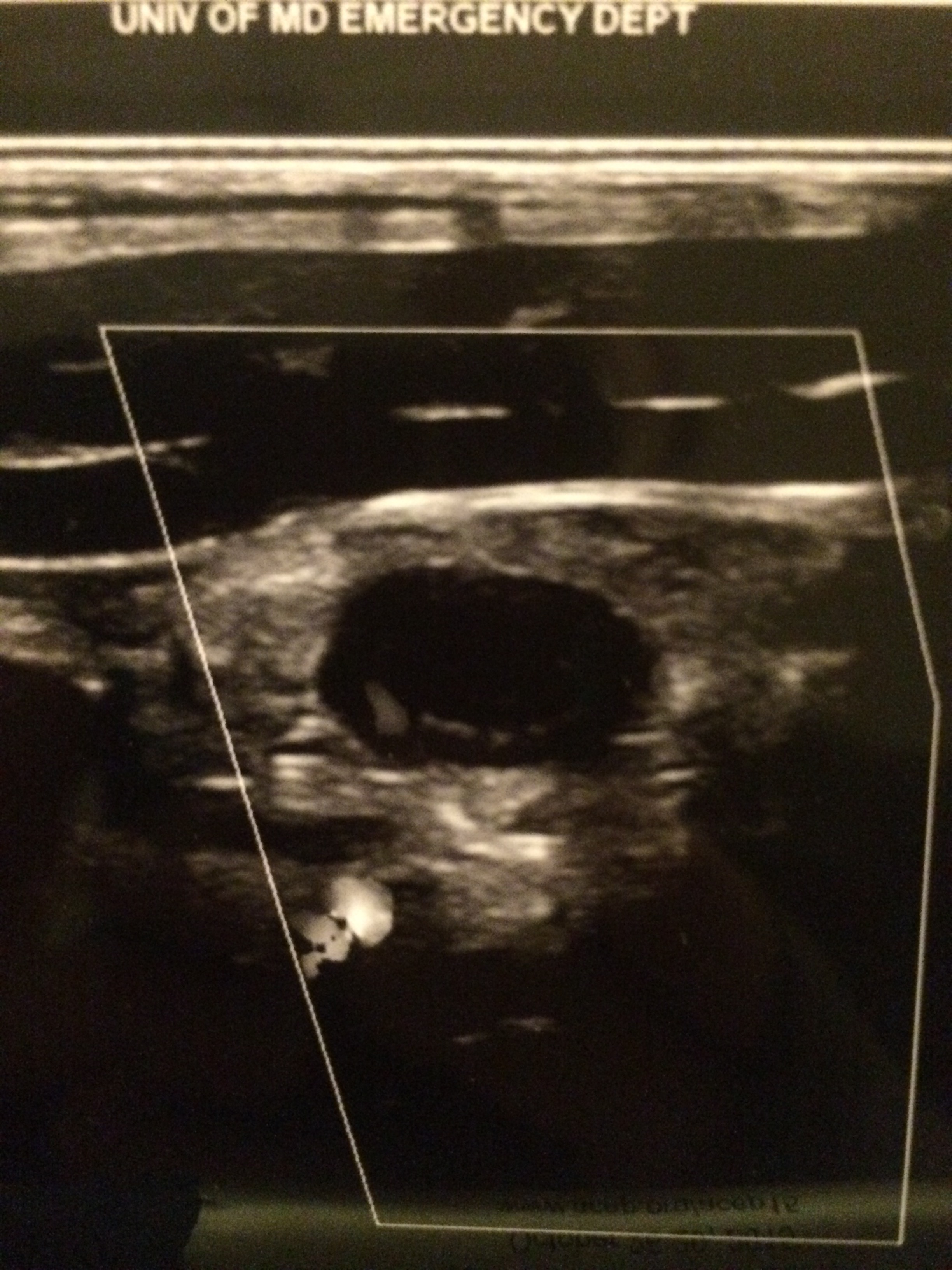
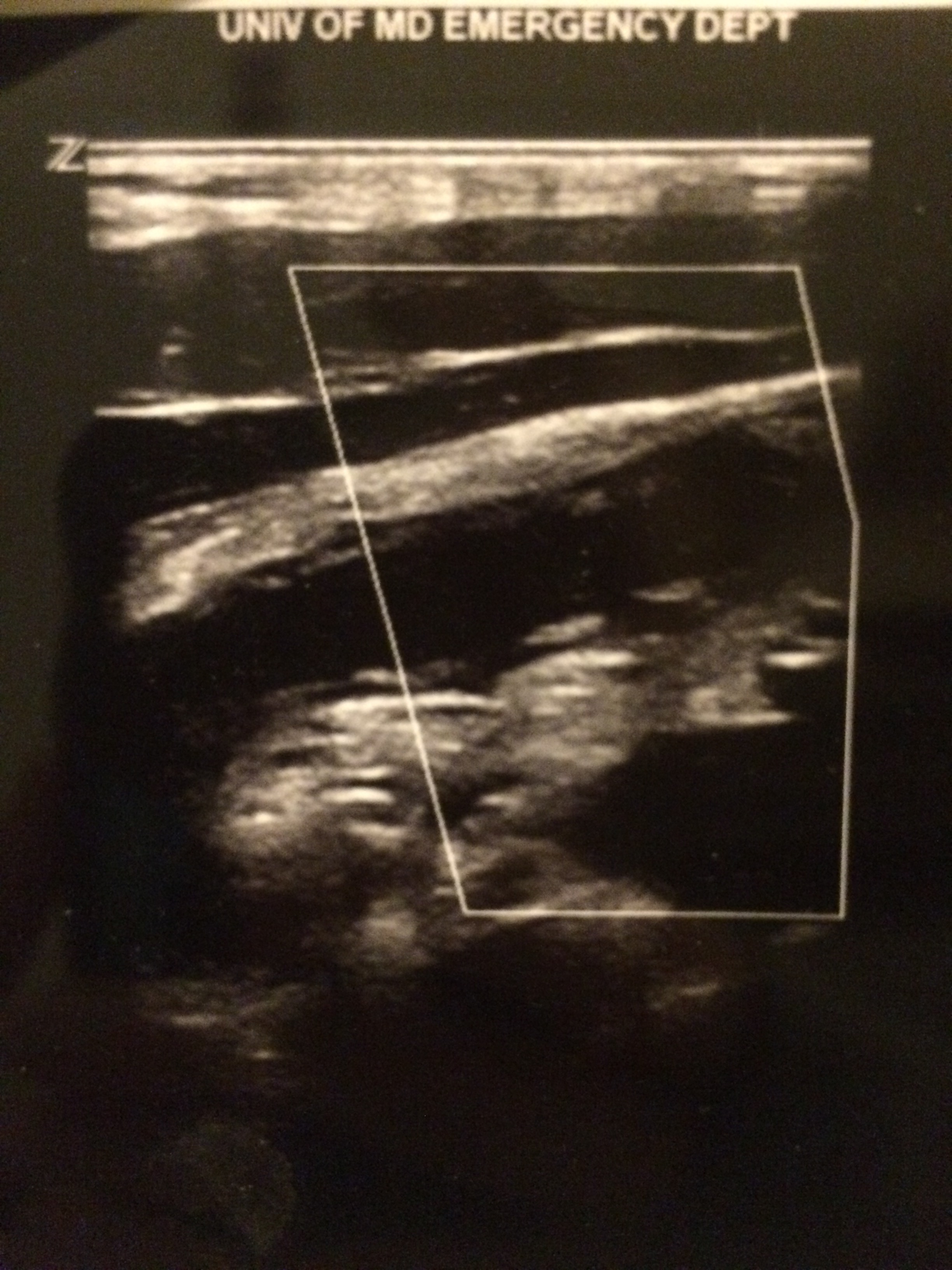
Positive study:
A non-compressible, blind-ending tubular structure in the longitudinal axis >6 mm without peristalsis (see second image above with 8.3 mm diameter measurement)
A target sign in the transverse view (see first image above)
Additional suggestive findings: appendiceal wall hyperemia with color Doppler, appendicoliths hyperechoic (white) foci with an anechoic (black) shadow, periappendiceal inflammation or free fluid
Negative study:
Non-visualization of the appendix with adequate graded compression exam in the absence of free fluid or inflammation.
Limitations for visualization and possible false negative result:
Retrocecal appendix and perforated appendix are difficult to visualize with US.
Pitfalls:
US has good specificity (93% in Sivitz et al article), but limited sensitivity (85% in Sivitz et al article), so trust your clinical judgement. You may need a MRI (pregnant/pediatrics) or CT as they have improved, but not perfect sensitivity.
The world of pediatrics is still working on catching up to adult literature in terms of lactate utilization and its implications. The study referenced looked at over 1000 children admitted to the pediatric intensive care unit. Lactate levels were collected 2 hours after admission and a mortality risk assessment was calculated within 24 hours of admission (PRISM III). Results showed that the lactate level on admission was significantly associated with mortality after adjustment for age, gender and PRISM III score.
Bottom line: In your critically ill pediatric patient, lactate may be a useful predictor of mortality.
There are numerous different causes of pediatric hemorrhagic diarrhea. Consider a pediatric patient with bloody diarrhea as being at risk for developing hemolytic uremic syndrome. Most cases of hemolytic uremic syndrome are caused by O157:H7 strains of E Coli that release Shiga-like toxin from the gut. Systemic release of the toxin causes microvascular thromboses in the renal microvasculature. The characteristic microangiopathic hemolysis results with anemia, thrombocytopenia and peripheral schistocytes seen on laboratory studies, in addition to acute renal failure.
Antibiotics have been controversial in the treatment of pediatric hemorrhagic diarrhea due to concern that they worsen toxin release from children infected with E Coli O157:H7 and thus increase the risk of developing hemolytic uremic syndrome. Numerous previous studies have provided conflicting data regarding the true risk (1). A recent prospective study showed antibiotic treatment increases the risk (2). Most recommendations warn against using antibiotics to treat pediatric hemorrhagic diarrhea unless the patient is septic.
Bottom line: Avoid treating pediatric hemorrhagic diarrhea with antibiotics
16 yo M with pleuritic right upper chest pain that started today. He is suffering from an asthma exacerbation currently in the setting of URI with cough. He is afebrile, tachycardic to 140-150s, respiratory rate 20, and sats 98% on room air. ECG was performed which incidentally diagnosed this patient WPW and he went for ablation as an outpatient. His chest x-ray showed:
Besides a bad day, what do we call this chest x-ray finding?
The NEXUS criteria is widely applied to adults who present with neck pain due to trauma. While this study did include about 2000 pediatric patients, there were not enough young children to draw definitive conclusions. For more information on the evaluation of the cervical spine, see Dr. Rice's pearl from 9/7/12. A 2003 study piloted an algorithm for cervical spine clearance in children < 8 years.
Patients were spine immobilized if: unconscious, abnormal neurological exam, history of transient neurological symptoms, significant mechanism of injury, neck pain, focal neck tenderness or inability to assess based on distracting injury (extremity or facial fractures, open wound, thoracic injuries, or abdominal injuries), physical exam findings of neck trauma, unreliable exam due to substance abuse, significant trauma to the head or face, or inconsolable children.
When the 2 pathways (see attached) were implemented, there was a decrease in time to cervical spine clearance. There were no missed injuries in the study period prior to implementation of the pathway or once it was implemented. There was no significant difference in the amount of xrays, CT scans or MRIs.