Primary headaches (not secondary to a life-threatening disease) can be challenging to manage. Remember the following pearls:
Things that DO NOT work: IV fluids, 5-HT3 Antagonists (aka Zofran), diphenhydramine (aka Benadryl), opioids
Things that KINDA work: oxygen for all headaches, sphenopalatine ganglion block (4% lido spray)
Things that PREVENT recurrence: dexamethasone for migraine headaches
Bottom Line: Underdosing of benzodiazepines in status epilepticus may contribute to treatment failure.
Bottom Line: Use of IO allows more rapid administration of 23.4% NaCl with no immediate serious complications.
Bottom Line: The rate of serious neurologic conditions missed at an initial ED visit is low. However, the potential harm of misdiagnosis can be substantial.
Back pain with lower extremity symptoms can be concerning for cauda equina. Some pointers regarding the H&P:
None of these symptoms independently predicts cauda equina syndrome with an accuracy greater than 65%.
Bottom Line: do not depend on any one finding to reliably exclude or confirm cauda equina.
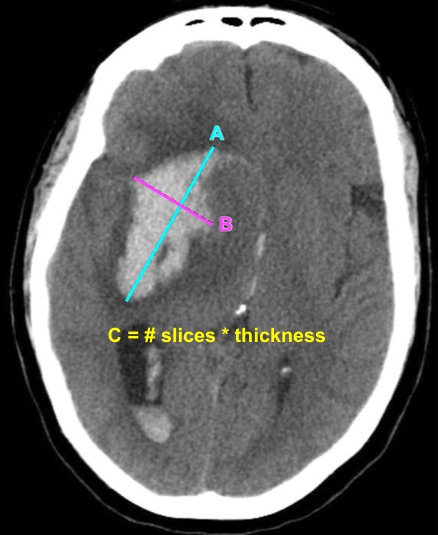
Bottom Line: EPs can reliably estimate ICH volume using the ABC/2 formula. Communicating ICH volume to neurosurgical and neurocritical care consultants can help direct treatment decisions.
A previous pearl discussed medication-overuse headache (MOH).
MOH is also known as analgesic rebound headache, drug-induced headache or medication-misuse headache.
It is defined as headache… occurring on 15** or more days per month in a patient with a preexisting headache disorder who has been overusing one or more acute treatment drugs for headache with symptoms for three or more months.
The diagnosis is clinical, and requires a hx of chronic daily headache with analgesic use more than 2-3d per week.
The diagnosis of MOH is supported if headache frequency increases in response to increasing medication use, and/or improves when the overused medication is withdrawn.
The headache may improve transiently with analgesics and returns as the medication wears off. The clinical improvement after wash out is not rapid however, patients may undergo a period where their headaches will get worse. This period could last in the order of a few months in some cases.
The meds can be dc’d cold turkey or tapered depending on clinical scenario.
Greatest in middle aged persons. The prevalence rages from 1% to 2% with a 3:1 female to male ratio.
Migraine is the most common associated primary headache disorder.
** Each medication class has a specific threshold.
Triptans, ergot alkaloids, combination analgesics, or opioids on ten or more days per month constitute medication overuse.
Use of simple analgesics, including aspirin, acetaminophen and NSAIDS on 15 or more days per month constitutes medication overuse.
Caffeine intake of more than 200mg per day increases the risk of MOH.
Consider MOH in patients in the appropriate clinical scenario as sometimes doing less is more!
Bottom Line: Consider using pre-procedural ultrasound-assistance for all lumbar punctures.
Diplopia can be a challenging complaint to address in the ED. Although not all patients will require imaging, use the simplified table below to help guide the imaging study needed:
| Clinical Situation | Suspected Diagnosis | Imaging Study | |
| Diplopia + cerebellar signs and symptoms | Brainstem pathology | MRI brain | |
| 6th CN palsy + papilledema | Increased intracranial pressure (e.g. idiopathic intracranial hypertension or cerebral venous thrombosis) | CT/CTV brain | |
| 3rd CN palsy (especially involving the pupil) | Compressive lesion (aneurysm of posterior communicating or internal carotid artery) | CT/CTA brain | |
| Diplopia + thyroid disease + decreased visual acuity | Optic nerve compression | CT orbits | |
| Intranuclear ophthalmoplegia | Multiple sclerosis | MRI brain | |
| Diplopia + facial or head trauma | Fracture causing CN disruption | CT head (dry) | |
| Diplopia + multiple CN involvement (3,4,6) + numbness over V1 and V2 of trigeminal nerve (CN5) +/- proptosis | Unilateral, decreased visual acuity | Orbital apex pathology | CT orbits with contrast |
| Uni- or bi-lateral, normal visual acuity | Cavernous sinus thrombosis | CT/CTV brain | |
C.N.: cranial nerve
Bottom Line: ED triage nurses can safely use the Canadian C-Spine Rule. This approach can improve patient care and decrease length of stay in the ED.
Manifestations due to neurosyphilis present as one of 3 categories: stroke due to arteritis, masses in the brain (granulomata), and chronic meningitis.
Although serum VDRL/TPPA tests will be positive in almost all patients, it’s important to remember that the diagnosis requires the presence of ALL of the following criteria:
1. positive treponemal (e.g. FTA-ABS, TP-PA) AND nontreponemal (e.g. VDRL, RPR) serum test results
2. positive CSF VDRL OR positive CSF FTA-ABS test result
3. one CSF laboratory test abnormality, such as pleocytosis (cell count >20/μL) or high protein level (>0.5 g/L)
4. clinical symptoms
This is important because the treatment of neurosyphilis is distinctly different from other forms, as it requires admission for IV antibiotics for at least 10 days.
Bonus Pearl: CSF RPR is unreliable as it is more likely to be falsely positive than other specific CSF testing.
Does using a combination of aspirin and clopidogrel decrease your patient’s risk of recurrent stroke after a minor ischemic stroke or high risk TIA event?
Bottom Line: The use of DAPT in minor ischemic stroke and high risk TIA reduces the risk of recurrent stroke. However, the duration of DAPT may affect the risk of major hemorrhage.
Bottom Line: LMWH appear to be similar in efficacy and safety compared with UFH for the management of CVT.
An infarct of the spinal cord is technically considered a stroke
The most common risk factor is a recent aortic surgery. Can also occur with straining and lifting (rare)
Patients will present with symptoms of spinal cord involvement with a hyperacute onset (less than 4 hours)
Although the “classic” presentation is anterior cord syndrome (flaccid paralysis, dissociated sensory loss (pinprick and temperature), preserved dorsal column function), patients may present with loss of all functions below the level of infarct due to spinal shock, confusing the clinical picture.
The most common level is T10
Medical decision-making capacity refers to the patient’s ability to make informed decisions regarding their care, and emergency physicians are frequently required to assess whether a patient possess this capacity. Patients with acute or chronic neurological diseases (such as dementia) may lack this capacity, and this should be identified, especially in life-threatening situations. The patient must have the ability to:
communicate a consistent choice
understand (and express) the risks, benefits, alternatives and consequences
appreciate how the information applies to the particular situation
reason through the choices to make a decision
There are numerous tools that may help with this assessment, but none has been validated in the ED. Be careful of determining that the patient lacks capacity just because of the diagnosis they carry.
BONUS PEARLS:
Capacity is a fluid concept; a patient may have the capacity to make simple decisions but not more complex ones. Capacity may also change over time
Psychiatry consultation to determine capacity is not obligatory but may be utilized for a second opinion.
Bottom Line: Consider obtaining neuroimaging in patients presenting with syncope only if clinical features suggest probable neurological syncope.