A 22 year old normally healthy male presents with tachycardia (HR 140), dilated pupils (7 mm), dry flushed hot skin, and confusion/agitation. His mother states he has a 1 day history of “talking out of his head not making sense”, “seeing things that aren’t there”, and “speaking to video game characters”. He has suprapubic tenderness with markedly distended bladder on exam revealing over 1 liter of urine on bladder scan. She found a small bottle containing a large amount of small 2-3 mm black seeds in his room and suspects he ingested them. What treatment options would you consider?

Bottom Line: Multiple modalities of intervention may be needed to combat various aspects of salicylate toxicity. These include gastric decontamination, fluid hydration, dextrose admiinistration, aggressive serum alkalinization, establishment of normokalemia and hemodialysis. Intubation and chemical restraint should be avoided if possible.

Bottom Line:
Kratom is an herbal extract used as an alternative medicine and recreational substance with marked increase in use over recent years. Kratom contains a complex mixture of psychoactive ingredients with effects at multiple receptors (mu, serotonin, dopamine, and alpha-adrenergic receptors) and causes stimulant effects at lower doses and opioid effects at higher doses. Depending on the predominant clinical effects, treatment with naloxone, benzodiazepine, and labetalol have been reported.

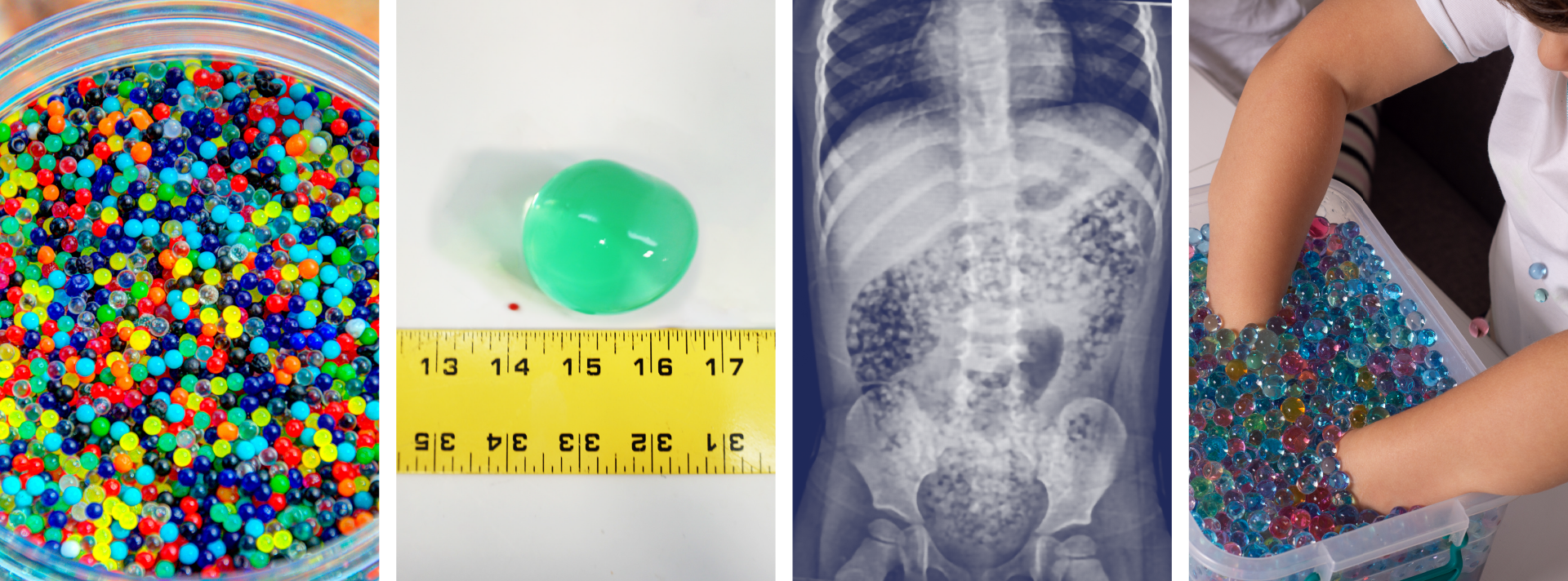
Water beads are a colorful, fun, popular, and widely available product found in children’s toys, stress squeeze balls, arts and crafts supplies, plant hydration products, air fresheners, and first aid ice packs.
These jelly-like small super-absorbent polymer balls are similar to the material found in diapers and absorb water expanding 100-800 percent of original size.
Pediatric ingestion is by far the most common poisoning exposure route but insertion into ears and nose and aspiration can occur and has led to serious adverse effects. More than 8000 water bead-related ingestion injuries have been treated in U.S. Emergency Departments.
Over the past 10 years, U.S. Poison Centers reported 19,660 exposures with 55% occurring in 2023 alone. In the majority of cases, no clinical effects (~88%) were seen, however in >11% of cases mild to moderate effects (abdominal discomfort, nausea, and vomiting) were reported and severe effects including complete bowel obstruction, necrosis, and surgical intervention in 0.11%. The Consumer Product Safety Commission reported at least one death of a 10-month-old girl in 2023 due to water bead ingestion.
Ingested water beads quickly pass into the small intestines where they continue to expand over the next few days and can become large enough (especially in children less than 2 year of age) to be unable to pass through the ileocecal valve causing small bowel obstruction requiring surgical intervention.
There is little data to guide management after ingestion. The majority of cases have no clinical effects and home observation is appropriate for asymptomatic for patients greater than 2 years. Recommendations from a report of case series and literature review , in patients less than 2 years of age with evidence of ingestion and symptomatic patients include hospitalization, imaging with US or CT, and close monitoring. CT, ultrasound, and endoscopy are not 100% reliable and often do not visualize these intraluminal foreign bodies.
In December 2025, the CPSC approved new federal safety standards for water beads toys setting limits on maximum expansion size of beads and amount of allowable acrylamide.
Cyanide is one of the deadliest known poisons causing immediate toxic effects and lethality within seconds to minutes. Exposures are rare, most commonly by inhalational route (HCN gas) from structural fires due to combustion of synthetic materials or from ingestion of cyanide salts. Cyanide toxicity can also occur from dermal or parental (sodium nitroprusside) exposure.
The preferred first line antidote is hydroxycobalamin (vitamin B12) available as Cyanokit, which has higher affinity for cyanide than cytochrome oxidase and binds to form harmless cyanocobalamin and is renally excreted. Limited studies reveal good survival rates in noncardiac arrest patients. Hydroxycobalamin has minimal side effects (red skin and urine, increased BP) and is well-tolerated with safer and simpler mechanism of action than Nithiodote (original antidote), containing sodium nitrite (CN preferentially binds methemoglobin to form cyanomethemoglobin) and thiosulfate (provides sulfur to convert cyanide to thiocynate for excretion). Sodium nitrite has numerous adverse effects causing hypotension and methemoglobin (contraindicated in smoke inhalation victims due to concern for carbon monoxide poisoning, G6PD deficiency, preexisting amenia), and hypersensitivity reactions. Sodium thiosulfate has less side effects and augments cyanide excretion but is considered less effective due to its slow onset, short half-life, low volume of distribution, and poor intracellular penetration.
As of August 2025, the American Society of Health -System Pharmacists (ASHP) Drug Shortage lists Cyanokit as “limited availability” in the U.S. as manufacturing was suspended due to investigation of ongoing quality defect with concern for sterility and endotoxin content. Impacted batches were released and their numbers are listed in an FDA bulletin (see references). Healthcare providers should weigh the potential benefit of using Cyanokit against the risk of infection. Infusion set with 0.2 micron in line filter can be temporarily used for administration of Cyanokit 5 mg hydroxycobalmin to prevent potential infection.
Volatile inhalants such as glue, lighter fluid, spray paint are abused by "sniffing" (from container), "huffing" (poured into rag), or "bagging" (poured into bag). "Dusting" is the abuse of canned air dust removal products. These inexpensive easliy accessible products are so dangerous that manufacturers include product warnings regarding lethal consequences from misuse and even may indicate that a bitterant is added to discourage use. Common duster gases include the halogenated hydrocarbons, 1,1-difluoroethane or 1,1,1-trifluroethane which are highly lipid soluble and rapidly absorbed by alveolar membranes and distributed to CNS. Desired effect of euphoria and disinhibition rapidly occur but unwanted side effects include confusion, tremors, ataxia, pulmonary irritation, asphyxia and, rarely, coma.
"Sudden sniffing death" is seen within minutes to hours of use and is due to ventricular arrhythmias and cardiovascular collapse. Available experimental evidence postulates the following mechanisms: Inhibition of cardiac sodium, calcium, and repolarizing potassium channels hERG and I(Ks) causing reduced conduction velocity and altered refractory period leading to reentry arrythmias or myocardial "sensitiization" to catecholamines resulting in after depolarizations and enhanced automaticity. Treatment should include standard resuscitation measures but refractory arrythmias to defibrillation have been reported and use of amiodarone and beta blockers should be considered.
Bottom Line:

Drug-induced hypoglycemia is an important cause of hypoglycemia which should be considered in any patient presenting with altered mental status. In one study, drug-induced hypoglycemia represented 23% of all hospital admissions attributed to adverse drug events. Risk factors for developing hypoglycemia include older age, renal or hepatic insufficiency, concurrent use of insulin or sulfonylureas, infection, ethanol use, or severe comorbidities. The most commonly cited drugs associated with hypoglycemia include:
*In Glipizide users, there was 2-3 fold higher odds of hypoglycemia with concurrent use of sulfamethoxale-trimethoprim, fluconazole, and levofloxacin compared with patients using Cephalexin.
**Tramadol potentially induces hypoglycemia by effects on hepatic gluconeogenesis and increasing insulin release and peripheral utlizilation. Was seen in elderly at initiation of therapy within first 30 days.
BOTTOM LINE:
Take care in prescribing drugs known to increase risk of hypoglycemia in elderly patients, with comorbidities, or those already taking medications associated with hypoglycemia.
Scromboid (histamine fish poisoning) can be easily misdiagnosed since its' clinical presentation can mimic that of allergy. Seen most frequently in the summer and occurring with Scombroideafish (tuna, mackerel, bonito, skipjack) but also with large dark meat fish (sardines and anchovies) and even more commonly with nonscromboid fish such as mahi mahi and amber jack. In warm conditions when fish is improperly refrigerated, bacterial histidine decarboxylase converts muscle histidine into histamine which quickly accumulates. Histamine is heat stable and not destroyed with cooking.
Bottom Line:
Scromboid poisoning is due to histamine ingestion and is often misdiagnosed as allergic reaction. It is preventable with proper fish storage.
The primary tenet of poisoning treatment is to separate the patient from the poison. Gastric decontamination has been the cornerstone of poisoning treatment throughout history and methods include induced emesis, nasogastric suctioning, EGD or gastrostomy retrieval, activated charcoal, and whole bowel irrigation. Current guidelines for gastic decontamination are limited to few clinical situations. The detection of residual life threatening poisons in the stomach would be of value in predicting who might benefit from gastric decontamination in overdose.
Plain radiographs have variable sensitvity in detecting radioopaque pills. Computed tomography (CT) has been successful and gained wide acceptance in the detection of drug in body packers. In a recent study, authors studied the usefulness of non-contrast abdominal computed tomography for detection of residual drugs in the stomach in patients presenting over 60 minutes from acute drug overdose:
BOTTOM LINE:
Non-contrast CT may help to predict which patients would benefit from gastric decontamination in acute life-threatening drug poisonings.
Most clinicians are familiar with use of methylene blue for the treatment of methemoglobinemia, as a urinary analgesic, anti-infective, and anti-spasmodic agent, or for its use in endoscopy as a gastrointestinal dye, but this compound also has a role as a rescue antidote in life threatening poisonings causing refractory shock states and other shock states.
Bottom Line:
Methylene blue should be considered when standard treatment of distributive shock fails.
CHS Treatment:
Bottom line: Patient education should be provided on the paradoxical and recurrent nature of the symptoms of CHS to discourage relapse of use often stemming from false preception of beneficial effects of cannabis on nausea.
A 19 year old male presents confused and very agitated complaining of seeing things and stomach pain. His friends report he ingested a naturally occurring plant to get high a few hours ago but is having a "bad trip". His physical exam :
Temp 100.3, HR 120, RR 14, BP 130/88. Pulse Ox 98%.
Skin: Dry, hot , flushed
HEENT: Marked mydriasis 6mm
Lungs: Clear
Heart: Tachycardic
Abdomen: Distended tender suprapubic with absent bowel sounds,
Neuro: Extremely agitated pacing, no muscular rigidity.
What has he ingested and what is the treatment?
A 68 year old male presents to the ED complaining of weakness to his legs. He states today his yard chores took him over 2 hours to complete instead of the usual 15-20 minutes due need to take frequent breaks for rest due to leg pain. He denied any chest pain or shortness of breath. Past medical history included hypercholesteremia, HTN, and CAD. He is taking aspirin and recently started on rosuvastatin.
His physical exam was unremarkable.
Results showed normal EKG and CBC. Bun was 70, Creatinine was 3.4, and CPK of 1025.
This patient has statin induced rhabdomyolysis and acute renal failure.
Take Home Points:
Sulfonylureas are commonly used oral hypoglycemic agents for type II diabetes. Agents on the market include glipizide (Glucotrol), glyburide (Micronase, Glynase, Dibeta) and glymepiride (Amaryl). These agents exert their effect by stimulation of insulin release from the pancreatic beta islet cells. Following overdose, hypoglycemia is usually seen within a few hours of ingestion and can be prolonged and profound. First line treatment for rapid correction of severe hypoglycemia is administration of an intravenous bolus of concentrated dextrose. However, use of dextrose infusion in attempt to maintain euglycemia is problematic as it can cause further release of insulin and rebound hypoglycemia. Octreotide ia a long acting synthetic somatostain analogue, blocks insulin secretion and has been shown to prevent recurrence of hypogylcemia better than placebo.
Bottom Line:
Methylene Blue is a dye that was synthesized in the late 1800s as an antimalarial drug. After the emergence of chloroquine its use loss favor partly due to unpopular side effects of temporarily turning the urine, other body fluids, and the sclera blue. Methylene blue is primarily known as a highly effective fast acting antidote for methemboglobinemia. Over the past few years, it has become an important therapeutic modality with expanding uses in cardiac surgery and critical care. As a potent inhibitor of nitric oxide mediated guanylate cyclase induced endothelium vascular smooth muscle relaxation, it has been shown to be effective in increasing arterial blood pressure and cardiac function in several clinical states, such as septic shock and calcium channel blocker poisoning.
BOTTOM LINE:
Methylene blue should be considered for treatment of refractory shock from calcium channel and beta blocker poisoning.
Clinical improvement in refractory hypotension and reduction of vasopressor dose has been described in several poisoning cases.
Recommended dose is 1–2 mg/kg injection with effects seen within 1 hour.
Despite initial excitement for the use of intravenous lipid emulsion (ILE) therapy as an antidote for serious poisonings due to lipohphilic drugs there remains an absence of evidence combined with an incomplete understanding of its efficacy, mechanisms of action, safety, and analytical interferences to recommend its use except in a few clinical scenarios.
The lipid emulsion workgroup performed a comprehensive analysis of four systematic reviews and based recommendations from consensus of expert panelists from the American Academy of Clinical Toxicology, the European Association of Poison Centres and Clinical Toxicologists, the American College of Medical Toxicology, the Asia Pacific Association of Medical Toxicology, the American Association of Poison Control Centers, and the Canadian Association of Poison Control Centers. Toxins evaluated had to have a minimum of three human cases reported in the literature.They concluded that ILE could be indicated for the following clinical situations:
The Bottom Line:
The use of Intravenous Lipid Emulsion in severe poisoning is recommended only for a few poisoning scenarios and was based on very low quality of evidence, and consideration of risks and benefits, adverse effects, laboratory interferences as well as related costs and resources.
Bradycardias caused by poisoning are due to the toxin's effects on cardiovascular receptors and cellular channels and transport mechanisms and are often refractory to standard ACLS drugs. The most common drug classes responsible for bradycardias are calcium channel and beta blockers and digoxin (cardiac glycosides). Sodium channel blockers, clonidine, and opiates also can cause bradycardias. Antidotes are as follows:
** ILE is recommended only in life threatening poisonings where other accepted therapies have been use first or in cardiac arrest clinical scenarios.


