24-year-old male with a history of Wagner's Granulomatosis, currently on Cellcept (Mycophenolate Mofetil) and high dose prednisolone, presented with two days of sore throat, malaise and the lesions shown in the picture. What is the diagnosis?


A 36-year-old male, who recently immigrated from Africa, presented to the ED with fever, rash, cough and shortness of breath. He was noted to be febrile to 39.0 C. The rash is disseminated but present mainly in his trunk as shown in the picture.

30 Year-old female presents to the ED for a rash. The rash started suddenly, mainly in her extremities and it is painful. The patient denied having fever or chills. Her past medical history is unremarkable. She admits to using cocaine frequently. The rash is shown in the picture.

A 15 months old male with no past medical history, presenting with two days of decreased oral intake and decreased urine output. The exam was notable for minimal tenderness of abdomen. During an oral fluid challenge in the ED, the patient had a single episode of bilious vomiting. The ED physician ordered an ultrasound study and the results are shown below. What is the diagnosis?

30 year old female presents with a painful finger for 1 week. Finger exam showed the following. What is the diagnosis ?

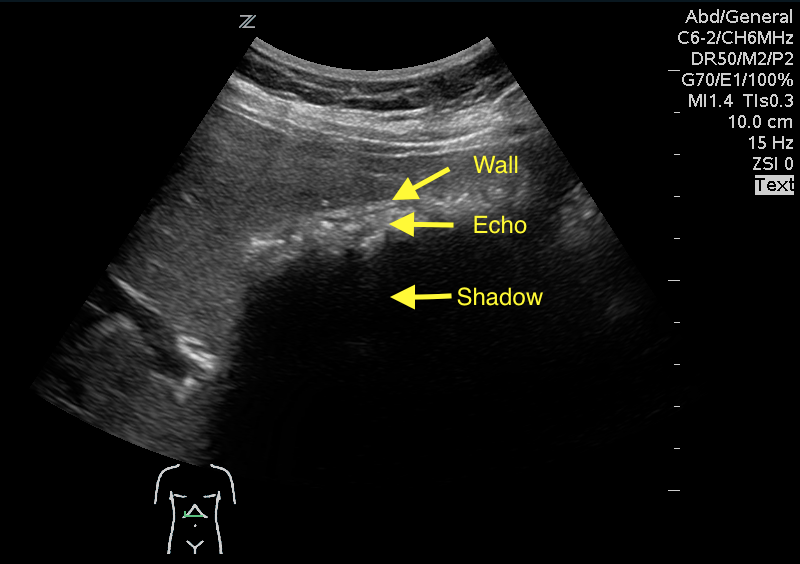
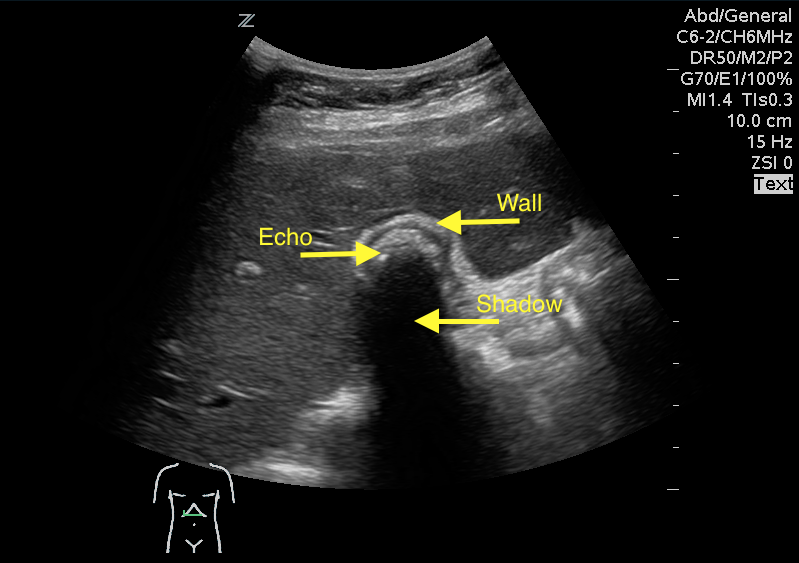
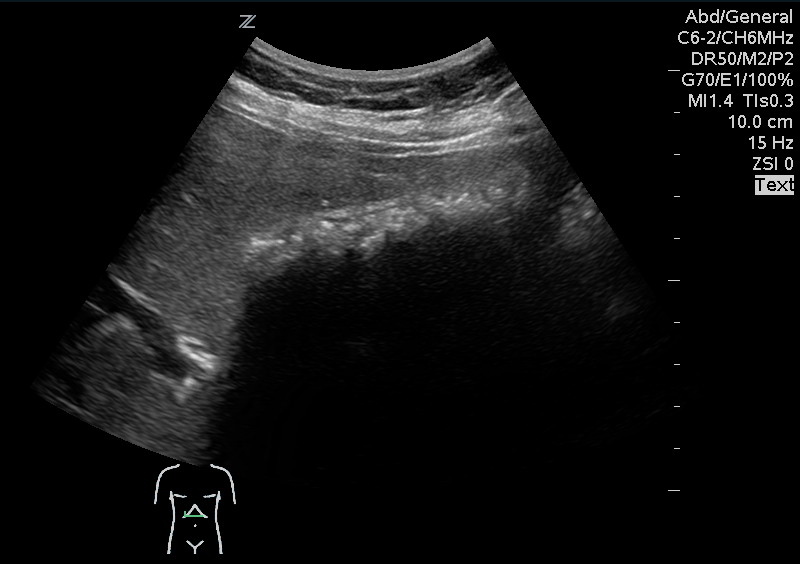
A 41 year old female presenting with intermittent RUQ abdominal pain for 1 week. An ultrasound of the right upper quadrant was performed. What is the diagnosis ?

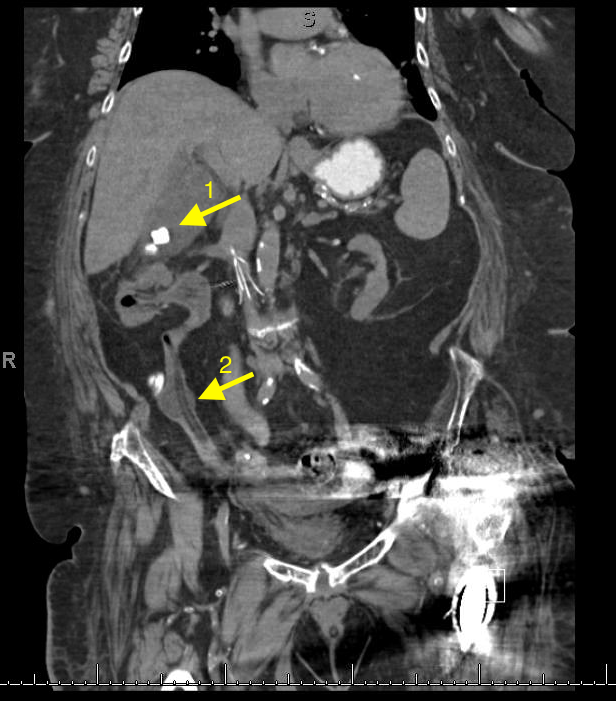
A 67 year old female with history of CVA, presented from a nursing home with RUQ abdominal pain and inablitiy to tolerate PO for 3 days. A CT scan of her abdomen was obtained. What is the diagnosis ?