Bottom Line: Consider RCVS in the differential of thunderclap headache and in patients who present with worse than usual migraine headache.
Bottom Line: The use of neuroimaging to identify an ischemic penumbra that may benefit from thrombectomy may be considered even for patients with time of last known well beyond 6 hours.
Take Home Point: This small but interesting study looked at the incidence of isolated aphasia presenting for concern of stroke. They found that none of their patients had evidence of an infarct, suggesting that strokes affecting language without motor or sensory deficits are uncommon.
Traumatic brain injury (TBI) is associated with close to half of major trauma admissions in adults over age 65 in the U.K.
Falls accounted for 85% of all TBIs, while 45% of patients had subdural hematomas (SDH).
More than 3/4 of patients were treated conservatively, though outcomes were not significantly better than those who underwent neurosurgical intervention.
Higher age is associated with higher mortality and greater disability.
Bottom Line: Trauma in older adults is increasing and fall prevention is important in reducing significant injuries.
IV vs. Non-IV Benzodiazepines for Cessation of Seizures
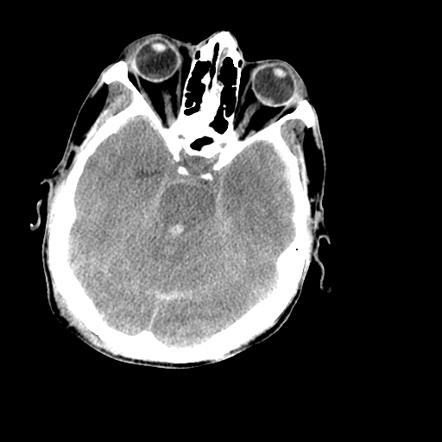
50 YOF with acute onset of worst headache of life associated with nausea and vomiting. Patient is somnolent, will rouse to noxious stimuli and complains of a headache as well as decreased vision.
What is the role of EEG for first-time seizures in the ED?
Take Home Point: A 30-minute routine EEG in the ED in adults with an uncomplicated first-time seizure revealed a substantial number of epilepsy diagnosis and can change ED management with immediate initiation of antiepileptic medication.
Bottom Line: The motor GCS and Simplified Motor Scale (SMS) have similar discrimination when compared with the total GCS, and may be easier to use.
Impact of an ED pharmacist on time to thrombolysis in acute ischemic stroke
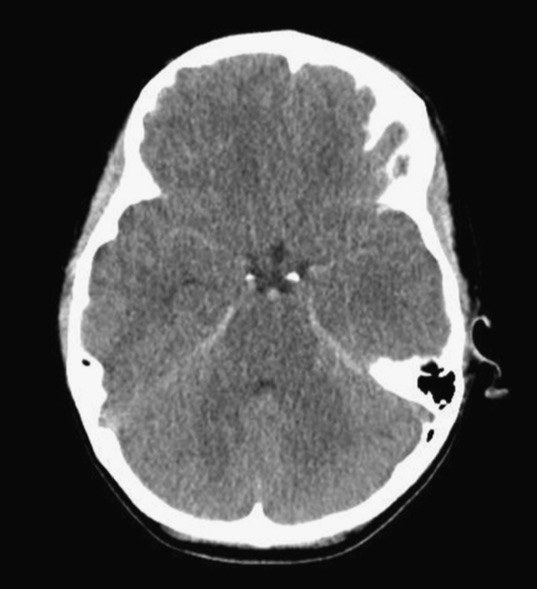
Patient found pulseless after submersion in water for 20 minutes. After ROSC, patient’s GCS was 3 and pupils are dilated and nonreactive.
Updated Guidelines for Traumatic Brain Injury
The Brain Trauma Foundation (BTF) Guidelines for the Management of Severe Traumatic Brian Injury (TBI) was recently updated and published in September 2016.
Updated recommendations include:
For the executive summary and complete guidelines, go to https://braintrauma.org/guidelines/guidelines-for-the-management-of-severe-tbi-4th-ed#/

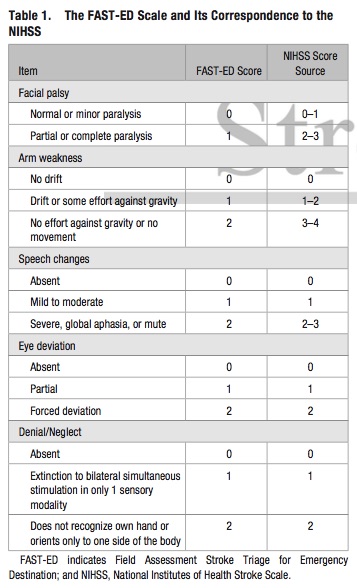
Bottom Line: Additional assessment of gaze deviation, aphasia and neglect, as included in the FAST-ED scale, increases the accuracy of predicting LVOS.