--Late awakening (>48h after sedation held) was common (78/402) in patients with cardiac arrest in prospective cohort study
--Poor prognostic signs of discontinuous (10-49% suppression) EEG and absent brain stem reflexes were independently associated with late awakening. Use of midazolam also associated with late awakening
--Late awakeners had good functional outcome when compared to early awakeners
DON'T NEUROPROGNOSTIC EARLY (OR IN ED)!
And traditional poor prognostic signs may not be as poor as previously thought!
------------------
Rey A, Rossetti AO, Miroz JP, et al. Late Awakening in Survivors of Postanoxic Coma: Early Neurophysiologic Predictors and Association With ICU and Long-Term Neurologic Recovery. Critical Care Medicine: January 2019 - Volume 47 - Issue 1 - p 85–92
--RV systolic function is negatively affected by high RV afterload
--High mean airway pressures on the ventilator (particularly in modes such as APRV [airway pressure release ventilation]) can induce RV dysfunction
*****CLICK BELOW FOR A GREAT CASE!!!*****
At the Society of Critical Care Meeting (SCCM) this month, updates to the Surviving Sepsis Guidelines were released. Recommendations include:
--Initial 30mL/kg crystalloid resuscitation with frequent reassessment of fluid responsiveness using dynamic (not static) measures [goodbye CVP/ScvO2!]
--Initiation of broad-spectrum antibiotics within ONE hour of sepsis recognition [two agents from different classes]
--Further hemodynamic assessement (e.g. echo for cardiac function) if clinical assessment does not reveal the type of shock [get out the ultrasound!]
--Recent meta-analysis comparing continuous infusion versus intermittent bolus dosing of beta-lactam antibiotics demonstrates mortality benefit (NNT = 15) in patients with severe sepsis or septic shock. (1)
--Consider beta-lactam continuous infusion on your septic patients if your hospital pharmacy allows
[Thanks to Anne Weichold, CRNP for providing the article for this pearl!]
The Neurocritical Care Society and Society of Critical Care Medicine just came out with new Guidelines for Reversal of Antithrombotics in Intracranial Hemorrhage (ICH) [1]
--PCC is now recommended over FFP in reversal of vitamin K antagonists (VKA) with elevated INR. Either should be co-administered with 10mg IV vitamin K. (Strong recommendation, moderate quality evidence)
TAKE AWAY: PCC should be probably be given over FFP in VKA-ICH when available
--In this study, PE was diagnosed in ~17% of patients hospitalized for syncope (though this represents only ~4%% of patients presenting to the ED with syncope).
--Patients with PE were more likely to have tachypnea, tachycardia, relative hypotension, signs of DVT, and active cancer -- take a good history and do a good physical exam!
--Consider risk stratifying (Wells/Geneva) and/or performing a D-dimer (i.e "rule out" PE) on your syncope patients, particularly when no alternative diagnosis is apparent.
It's Election Day in the US, so here are some interesting facts about Presidential causes of death:
George Washington likely died from epiglottitis on 12/14/1799
CLICK BELOW FOR MORE INTERESTING FACTS!
--Massive PE is defined as PE with obstructive shock (hypotension [SBP <90] or end-organ malperfusion)
--Consider venoarterial (VA) ECMO in massive PE for hemodynamic support, particularly prior to intubation
--VA ECMO may prevent intubation/mechanical ventilation, surgical intervention, systemic and local thrombolysis
TAKE HOME POINTS:
-- High chloride load is associated with adverse outcomes in large-volume resuscitation (>60mL/kg in 24h), including increased risk of death [1]
-- Avoid supraphysiologic chloride solutions (i.e. normal saline) when resuscitation volumes are likely to exceed 60mL/kg (e.g. sepsis, DKA)
--Aggressive BP management (SBP <140) in atraumatic intracerebral hemorrhage (ICH) does NOT signifcantly improve mortality or disability compared with traditional goal (SBP <180) [1]
--However, a lower goal (SBP <140) has been shown to decrease hematoma size and be safe compared to a higher goal (SBP <180) [2]
Zika virus has received significant media attention in the US due to its recent link with teratogenicity. But Zika is also associated with critical and life-threatening complications, including death. Differentiating it from other Flavivirus diseases such as Dengue or Chikungunya can be challenging.
Diagnosis
Complications
Disclaimer: Talking about seizures/status that is NOT due to eclampsia
TAKE HOME: While no AEDs are completely safe in pregnancy, treatment and stabilization of maternal status epilepticus is paramount for fetal health. Involve neurology/epileptology and OB/maternal-fetal medicine.
There are multiple vasoactive infusions available for acute hypertensive emergencies, many having serious side effect profiles or therapeutic disadvantages.
Clevidipine (Cleviprex) is rapidly-titratable, lipid-soluable dihydropyridine calcium channel blocker which has become increasingly used in the ICU in recent years [1]:
ECLIPSE trial compares clevidipine, nicardipine, nitroglycerin and nitroprusside in cardiac surgery patients. .
Clevidipine was as effective as nicardipine at maintaining a pre-specified BP range, but superior when that BP range was narrowed (also studied in ESCAPE-1 and ESCAPE2 with similar results) [2-3]
TAKE-HOME: Clevidipine is an ultra short-acting, rapidly-titratable vasoactive with favorable cost, pharmacokinetics, and side-effect profile. Consider its use in hypertensive emergencies.
What classifies "submassive PE"?
Submassive PE has early benefit from systemic thrombolysis at the cost of increased bleeding [1].
Ultrasound-accelerated, catheter-directed thrombolysis (USAT) [the EKOS catheters] has been shown to be safe, with low mortality and bleeding risk, as well as immediately improved RV dilation and clot burden [2-4]. USAT may improve pulmonary hypertension [4].
USAT is superior to heparin/anti-coagulation alone for submassive PE at reversing RV dilation at 24 hours without increased bleeding risk [5].
Long-term studies evaluating chronic thromboembolic pulmonary hypertension (CTEPH) need to be done, comparing USAT with systemic thrombolysis and surgical thombectomy.
Take-home: In patients with submassive PE, USAT should be considered over systemic thombolysis or anti-coagulation alone.
The EuroTherm3235 Trial was a randomized, multi-center trial to study hypothermia (32-35oC) in severe, traumatic brain injury1:
--The role of antibiotics in acute exacerbations of COPD remains controversial in many settings. However, a recent Cochrane review concludes that antibiotics have "large and consistent" benefit in ICU admissions [1]:
--However, patients on antibiotics had increased side effects, are at risk for increased drug-drug interaction (think azithromycin/levofloxacin), and the effect on multi-drug resistance is unclear.
--GOLD Guidelines are a bit more liberal with their recommendations for antibiotics [2], recommending antibiotics based on symptoms or in patients needing mechanical support.
--TAKEAWAY -- if your patient needs BiPAP or ICU, they should also get antibiotics!
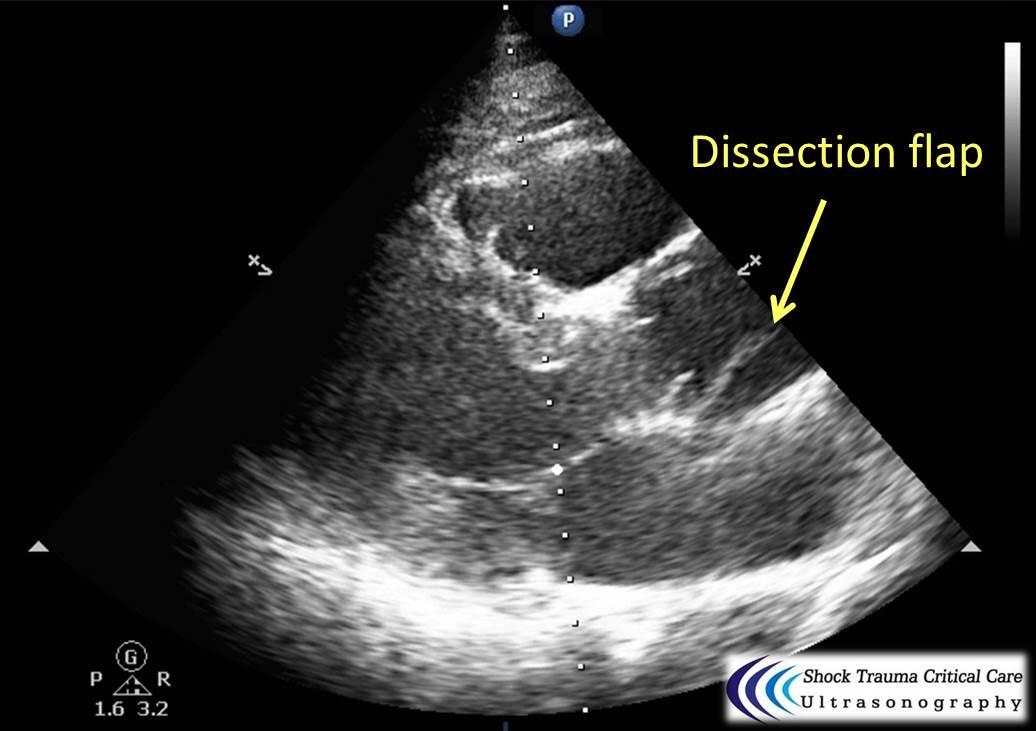
Classically, aortic dissection presents as tearing or ripping chest pain that radiates to the back in a HYPERtensive patient.
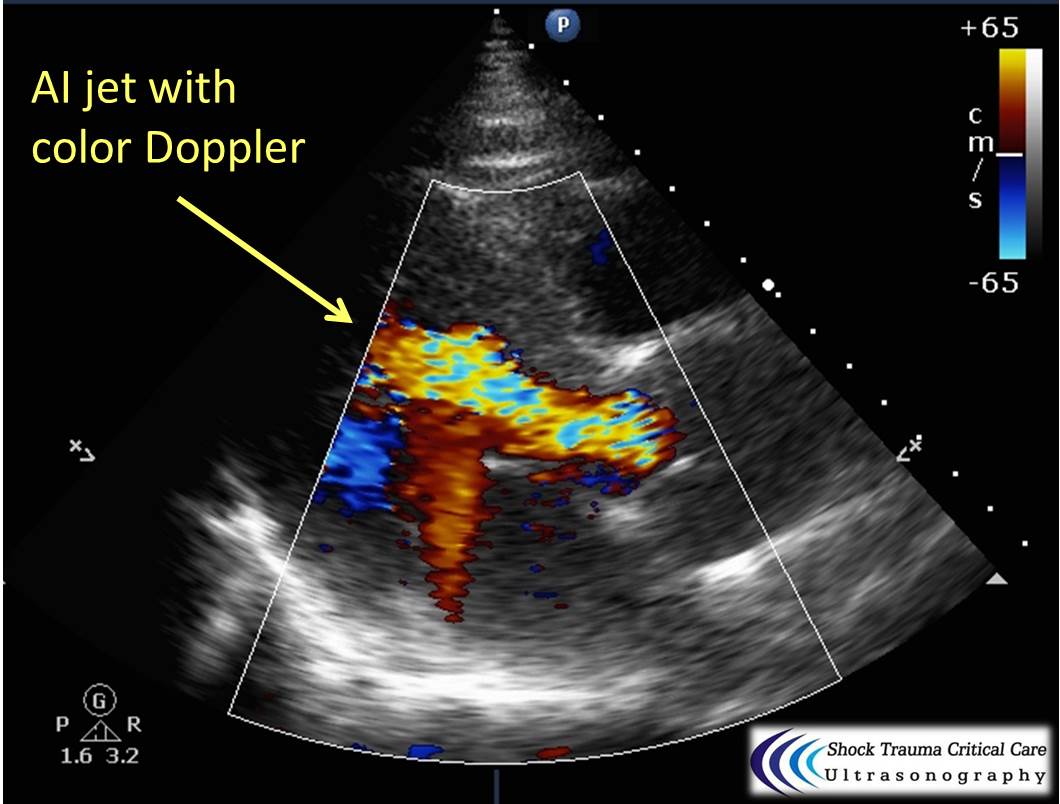
However, type A aortic dissections can quickly become HYPOtensive due to any the primary cardiac complications from retrograde dissection into:
Bedside echo can't rule out aortic dissection, but it can help rule in the diagnosis (figure 1) or complications (figure 2) at times.
Your ESLD patient is hypotensive with a tense abdomen, and he needs a paracentesis!
--ALWAYS use ultrasound to localize a fluid pocket [Fig 1]! Take the time to use color Doppler to look for underlying abdominal wall varices [Fig 2]. Cirrhotic patients frequently have abnormal abdominal wall vasculature [1-2].
--Hemorrhage from paracentesis is exceedingly rare, and reversal of mild coagulopathy probably isn't that important [3-4].
--In hypotensive patients, consider placement of a small pigtail catheter for slow, continuous drainage (e.g. 8.3F pericardiocentesis catheter) instead of large-volume paracentesis. Non-tunneled catheter infection risk goes up after 72h [5].
--Albumin replacement improves mortality and incidence of renal failure in patients with SBP or other infection [6-7].
Ever forget all the things that make up MUDPILES in your AG acidosis differential?
Instead, consider the less-complicated mnemonic "KILR"!
K Ketoacidosis (diabetic, alcoholic, starvation)
I Ingestion (salicylate, acetaminophen, methanol, ethylene glycol, CO, CN, iron, INH)
L Lactic acidosis (infection, hemorrhage, hypoperfusion, alcohol, metformin)
R Renal (uremia)
Once you rule out the KLR causes, begin to consider ingestion or a tox source as your source. Remember that many of the listed ingestions can also cause a lactic acidosis.