The Salter Harris Classification System is used in pediatric epiphyseal fractures. The higher the type of fracture the poorer the prognosis
Some common exam facts about Salter Harris Fractures are:
The Classification system as listed by Type:
A image of the fractures can be found on FP Notebook at http://www.fpnotebook.com/_media/OrthoFractureSalterHarris.jpg
http://www.gentili.net/signs/images/400/spinescottyparsdefectdrawing.JPG
The Scotty dog’s head (superior articular facet), nose (transverse process), eye (pedicle), neck (pars interarticularis), and body (lamina) should be easily identified on the oblique radiograph.
Odontoid Fractures:
There are three types of C2 odontoid fractures:

Calcaneus Fractures:
Calcaneus fractures can easily be missed on plain films and the true extent of the injury might not be appreciated until a CT is done. However, you can increase your change of picking up a calcaneal fracture by evaluating Bohler's Angle.
Lateral radiographs of the foot are needed to evaluate the Bohler angle. This is the angle made by drawing a line from anterior process of the calcaneus to the peak of the posterior articular surface and a second one drawn from the peak of the posterior articular surface to the peak of the posterior tuberosity. (See Picture) The average angle is 25-40°. Angles less than 25' are strongly suggestive of a fracture and the patient should probably get a CT of their foot if there is clinical suspicion.
Wound Care:
Patients and many providers want to irrigate or wash a wound with an antiseptic solution in order to decrease the risk of infection. Most studies have shown that irrigation whether with tap water or sterile water is effective enough in reducing bacterial counts in a wound so does adding an antiseptic solution offer any additional benefit.
It turns out that hydrogen peroxide, and iodine based solutions can actually hinder wound healing as they causes delays in the migration and proliferation of fibroblasts at concentrations that are not even bactericidal. Chlorhexidine, and silver containing antiseptics [i.e.: silver sulfadiazine and silver nitrate] are bactericidal at concentrations that do not affect fibroblasts.
So in the end, if you feel the need to use an antiseptic, use chlorhexidine or a silver containing antiseptic. The use of hydrogen peroxide and iodine based solutions should be abandoned as they are not even bactericidal at concentrations that have profound affects on the fibroblasts.
Septic Arthritis versus Arthritis:
Though CRP and ESR levels are significantly higher in patients that have septic arthritis, a 1998 study showed that there is extensive overlap between patients with septic arthritis crystal assoicated arthritis that both CRP and ESR have low sensitivity, specificity and predictive values. Peripherial WBC counts did not differ between the two disease processes..
The morale of the story: If you are suspecting septic arthritis you need to perform an arthorcentesis to analysis the synovial fluid. Systemic biomarkers can not support one diagnosis over the other.
Osteomyelitis:
Radial Head Fractures:
Radial head fractures can often be difficult to visualize on plain films especialing Mason Type 1 fractures (see prior pearl on classification system) which are nondisplaced. Often the only sign of a fracture will be a posterior fat pad sign which is always considered to be pathologic. The posterior fat pad lies outside the synovium of the elbow joint and is normally hidden in the fossa of the distal humerus preventing it from being seen on lateral films of a normal elbow. Trauma to the elbow that results in a intraarticular fracture (typically a radial head fracture) produces an intra-articular hemorrhage that distends the synovium and displaces the fat out of the fossa, producing the typical triangular radiolucent shadow posterior to the distal end of the humerus.

Conservative Treatment of Back Pain:
Muscle relaxanats and benzodiazipnes are often used in the non-operative management of sciatica and non-specific low back pain. In fact, a 2003 Cochrane review concluded that muslce relaxanats were effective in the management of non-specific low back pain. However, a recent analysis of randomized trials reported little efficacy or only minor benefits with the use of benzodiazapines in treatment of low back pain.
A recent prospective, randomized, placebo-controlled, double-blinded trial conducted in Germany that enrolled a total of 60 patients found that the use of diazepam was equivilant to placebo in the reduction of distance of referred pain at day 7 of treatment. Diazepam was also noted on average to increase the length of stay of those patients hospitalized by 2 days (median hospital days of 8 for placebo versus 10 for diazepam), and the probablility of pain reduction on a visual analog scale by more than 50% was twice as high in the placebo group (p< 0.0015). Placebo reduced the patients pain more than diazepam.
Though the sample size was small; this study should really make one reevaluate the use of diazepam in the treatment of back pain. Early movement and discouraging bed rest have been associated with decreased back pain, so one mechanism by which benzodiazepines may make things work is by causing enough sedation to prevent early movement.
Carpal Tunnel Syndrome (CTS):
Prosthetic hip dislocations are a common occurance in the Emergency Department. After you have gotten the hip back in place there are several ways to prevent the hip from coming out again. An abductor pillow will work but it confines the patient to bed. A better option to prevent further hip dislocations until the patient can get an appropriate brace made or reparative surgery is to place the patient in a straight leg knee immoblizer. It is nearly impossible to dislocate your hip if your knee is fully extended.
So after reduction of their simple hip dislocation (i.e: no fractures) place the patient in a straight leg knee immobolizer and they can followup with their orthopedist as an outpatient.
Review of the Appearance of Ossification Centers in Children's Elbows
Determing if a child's elbow has a fracture or if you are looking at an ossification center is easier if you remember the mnemonic CRITOE. This is the order that the ossification centers appear:
Knee Dislocation:
Pelligrini-Stieda Lesion:
A Pelligrini-Stieda lesion is shown in the radiograph below. This lesion was originally described in 1905, and is associated with a tear of the Medial Collateral Ligament. Heterotrophic calcification forms causing chronic pain, which typically needs to be surgically excised.
So for the students out there, it is possible to diagnosis an MCL tear on plain radiographs. Just not very often.

The Segond Fracture:
An benign appearing avulsion fracture of the lateral tibeal plateau that is marker for more significant injuries such as:
If this avulsion fracture is seen consider immobilzing the patients knee until they can follow up with Orthopedics and/or get an MRI to determine if additional injuries are present.

A recent study by Smith et al showed that the general abdomen/pelvic CT scan in trauma patients obtained with 5mm slices is a better screening test for spine fractures than plain films. They also showed that when compared to dedicated reconstructed thoracolumbar CT scan (2mm slices focused on the spine) it did not miss any clinically significant fractures.
The statistic for plain radiographs and the nonreconstructive CT scan are shown below.
| | Plain Radiographs | Nonreconstructive CT Scan | ||
| | Lumbar | Thoracic | Lumbar | Thoracic |
| Sensitivity % [95% CI] | 47 [33 to 62] | 13 [3 to 32] | 94 [83 to 99] | 73 [50 to 89] |
| Specificity % [95% CI] | 91 [78 to 97] | 71 [54 to 85] | 95 [85 to 99] | 94 [79 to 99] |
| Positive Predictive Value % [95% CI] | 85 [66 to 96] | 15 [2 to 45] | 95 [86 to 99] | 89 [67 to 99] |
| Negative Predictive Value % [95% CI] | 61 [48 to 72] | 56 [41 to 71] | 93 [82 to 99] | 83 [66 to 93] |
The take home point is that dedicated Spine CT scans are probably not needed unless they are going to be used to guide surgical or non-surgical management, and plain films should probably be abandoned in patients that are undergoing CT scans of the chest/abdomen/pelvis.
Impingement Syndrome and the Diagnostic Accuracy of 5 Common Tests
It is also reported that subacromial impingement syndrome (SAIS) is the more frequent cause of shoulder pain.
The authors of this study attempted to determine the diagnostic accuracy of the following 5 tests for SAIS:
The study demonstrated that any 3 positive tests out of the 5 has a sensitivity of 0.75 (0.54-0.96) , specificity of 0.74 (0.61-0.88), positive likelihood ratio of 2.93 (1.60-5.36) and negative likelihood ratio of 0.34 (0.14-0.80). See the table below for the individual test characteristics. No single test was deemed accurate enough to make the diagnosis by itself.
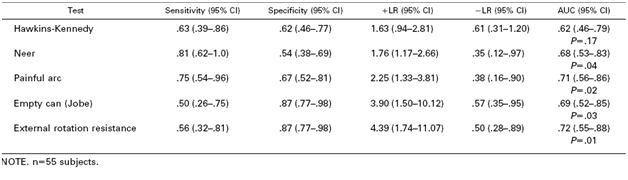
So in the end you should be familiar with most of these tests in order to use a combination of them to make the diagnosis of impingement syndrome. Future pearls will review how to perform these tests.
Scaphoid Fractures:
For suspected scaphoid fractures with negative radiographs it is common practice to put a person in a short arm thumb spica splint until followup up radiographs can be obtained in 10-14 days.
However, there is evidence that a short arm thumb spica splint is not enough for people that have a true scaphoid fracture. Gellman et al demonstrated that long arm thumb-spica cast immobilization for six weeks followed by short arm thumb-spica cast immobilization decreased time to union by 25% when compared to short arm thumb-spica casting alone.
The theory is that the short arm splint still allows for forearm rotation that can cause shearing motion of the volar radiocarpal ligaments. A long arm splint prevents this shearing action. The disadvantage of a long arm splint though is potential elbow joint stiffness and muscle atrophy that can occur during the prolonged period of immobilization.
So for your next patient with a scaphoid fracture seen on radiographs place them in a long arm thumb spica splint.
Acute paronychia
Scaphoid Fractures in Children:
Because of the high (30%) fracture rate seen on followup films it is recommended that all children be placed into a thumb spica splint until followed up.