As we eat our turkey today and the myth that we are tired because of the tryptophan content is propagated further - nothing to do with the 2000kcals that we just ate - I would like to share an interesting and controversial study.
Use of stimulants and and sedatives by EM residents. Incidence is as follows:
In a study of 485 residents with 47% response rate:
Prescription Stimulants: 3.1%
Sleep Aids (all): 89%
Use of Nonbenzodiazepines (zolpidem): 14%
Use of Melatonin: 10%
Benzodiazepines: 9%
Difficult job with difficult hours. What is the appropriate medication or is there a medication that truly assists with performance? Are they doing harm to themselves? to patients?
Disrupted circadian rhythm, addiction tendencies and the hardship of a stressful nightshifts are the price we pay for this specialty. Awareness and education are needed for the residents as well as the attendings.
In the setting of a patient suffering from an anticholinergic overdose with hallucinations/agitation, it may be beneficial to administer the antidote: Physostigmine. Many hesitate simply because they have never administered before or there may be doubt in the diagnosis. Here is the skinny:
1) Anticholinergic OD seen in following meds: diphenhydramine (Benadryl), dimenhydrinate (Dramamine), scopolamine, benztropine (Cogentin), some plants like datura stromonium (thorn apple)
2) Physostigmine 1mg IV slowly over a REAL 5 min. Administer to fast and patient may seize. Maximum dose of 2mg IV.
3) Contraindications: suspicion of TCA OD (anectdotal and from old case report) - screening EKG should be done prior to administration of physostigmine. Also glaucoma, closed angle, obstructive uropathy.
Remember your clinical endpoint needs to be measurable, thus hallucinations and agitation should be reversed. No indication if the patient is only experiencing dry mouth or other more mild anticholinergic symptoms.
French LK, et al. Hydrogen peroxide ingestion associated with portal venous gas and treatment with hyperbaric oxygen: a case series and review of the literature. Clinical Toxicology 2010;48:533–38.
Dabigatran
When a patient presents to the ED with a recent ingestion of a wild mushroom there are three very specific questions you must ask:
1) Exactly what time did you eat the mushroom?
2) Exactly what time did you begin vomiting/diarrhea/GI Sx in general?
3) Are there are more mushrooms that can be brought to ED for identification?
The reason the first two questions are critically important is it determines the total time of onset of toxicity. As a very general rule of thumb, delayed GI symptoms >6hrs is predictive of a possible lethal ingestion of a cyclopeptide containing mushroom like Amanita Phalloides. Immediate symptoms < 6hrs and even more so if within 2 hrs usually indicates ingestion of a nonlethal mushroom that causes GI distress (many mushrooms like Clitocybe nebularis)
Website with pics of the most poisonous mushrooms:
http://scienceray.com/biology/botany/13-deadliest-mushrooms-on-the-planet/
There is a saying:
"There are old mushroom pickers and wise mushroom pickers but no old and wise mushroom pickers"
Emerging evidence supports using intravenous fat emulsion (Intralipid) therapy for various drug overdoses, particularly those that are lipophilic. Within seconds to minutes of administration, toxic cardiovascular effects are reversed, including return of spontaneous circulation in cardiac arrest patients. Central nervous system effects also tend to improve.
Lipophilic agents for which there has been success include:
Bottom line: Consider intralipid therapy early in the course of a hemodynamically unstable patient with suspected overdose. Give a bolus of 1.5 mL/kg of 20% lipid emulsion over 1-2 minutes.
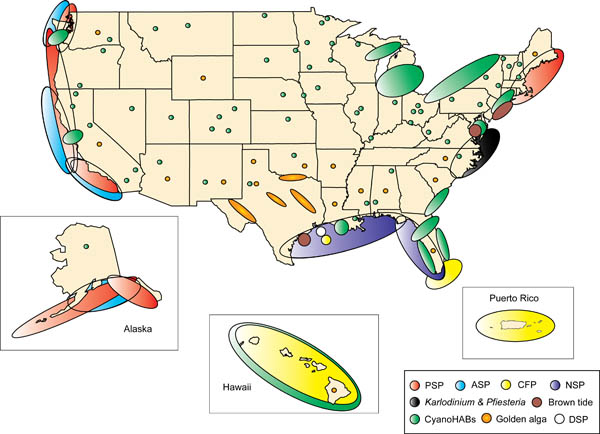
Although we may not be able to eat as much shellfish after the oil spill, there are still some left that can cause some interesting toxicity here in the USA. Shellfish act as vectors for the bacteria, virus etc that produces toxin thus not specific to one species of shellfish. There is a map attached that shows where shellfish poisoning occurs most. In the picture CFP=ciguatera, PSP=Paralytic and ASP=AmnesticC. Surprising the distribution and it will be interesting how the oil spill affects the distribution. Treatment for all of these is supportive with no known antidote and incidence increases during Red Tide months:
A fentanyl patch contains 100-fold more fentanyl in the reservoir than what is posted on the patch. For instance, 100mcg/hr patch will have over 10mg - thats milligrams - of fentanyl. This provides a rather large source for potential abuse. Overdose and deaths have occurred by patients in the following ways:
It is the many
In the setting of acute cyanide poisoning, it is virtually impossible to obtain a timely cyanide level to help assess toxicity. However, there are two diagnostic tests that can help confirm your diagnosis.
Remember cyanide halts cellular respiration meaning the cells cannot utilize oxygen. Therefore, the venous PO2 should be about the same as the arterial PO2. The cells then switch to anaerobic metabolism, thereby producing lactate.
A recent study examined the effects of accidental digital epinephrine injection from auto-injectors. 127 cases with complete follow-up had the following effects:
Pharmacologic vasodilators were used in 23%. Four patients had possible digital ischemia. All patients had complete resolution of symptoms, most within 2 hours. No patient was admitted, received hand surgery consultation, or had surgical care.
Although this speaks for the safety of digital anesthesia using epinephrine, it underscores the importance of providing education to patients who are prescribed epinephrine auto-injectors.
In a previous pearl we were discussing the need to perform EGD for any suicidal patient with a history of ingestion of a caustic to grade injury and assess chance of perforation and/or stricture formation. Suicidal patients are intentionally ingesting the caustic and can thus justify the risk/benefit ratio more easily than the pediatric unintentional ingestion. The concerned parent will bring the child in with a possible ingestion of a caustic. The container could be simply in the same room, spilled on the child and never be ingested. Even if ingested, the amount is less if the child tastes the caustic and will reflexively cause spitting. The literature is scant in regards to this type of patient but seems to point to this general algorithm:
Child displays 2 or more of the following symptoms there is enough evidence from case series that there will be a clinically signficant lesion found on EGD.
Vomiting, Drooling, Stridor, Presence of Oropharyngeal Burns
That being said, many clinicians would elect for EGD and assessment of airway with stridor alone. Do not be fooled into thinking if you see no oral lesions that there is no way the child ingested the caustic. Each case series showed a lack of correlation of physical exam findings to EGD findings.
We will all get the patient presenting with low blood glucose on a regular basis. In general, barring any underlying infection, those who are insulin dependent can be corrected with IV dextrose and/or food and be discharged. Those on a sulfonylurea may experience repeated hypoglycemic episodes and require admission - perhaps even treatment with the antidote: octreotide.
Below is the duration of action and half-life of the sulfonylureas which illustrates the need for admission:
Duration of action is the physiologic effect whereas the half-life is the pharmacokinetics of elimination of the drug. Often these two numbers are different for drugs. Do not let the half-life fool you into thinking it is safe to discharge a hypoglycemic patient on a sulfonylurea.
If benzodiazepines and supportive care fail to improve agitation and correct vital signs, several case reports indicate the successful use of cyproheptadine, an antihistamine with nonspecific antagonist effects at 5-HT1A and 5-HT2A receptors.
Cyproheptadine is available in 4 mg tablets or 2 mg/5 mL syrup. When administered as an antidote for serotonin syndrome, an initial dose of 8-12 mg is recommended, followed by 2 mg every two hours until clinical response is seen. Cyproheptadine is only available in an oral form, but it may be crushed and given through a nasogastric tube.
Cyproheptadine may lead to sedation, but this effect is consistent with the goals of management. It may also produce transient hypotension due to the reversal of serotonin-mediated increases in vascular tone. Such hypotension usually responds to IV fluids. Cyproheptadine is rated category B for safety in pregnancy by the FDA.
Ingestion of caustics can lead to immediate burns to mouth, esophagus, stomach as well as possible perforation. Months and years later, further complications are esophageal stenosis and increased incidence of esophageal carcinoma. The main benefit to EGD is to determine extent of injury within the esophagus. The lesions are graded much like a burn:
Grade I: Mild burn, no risk for esophageal stenosis
Grade II: Moderate, if circumferential, patient is at risk for esophageal stenosis
Grade II: Eschar present, high risk of perforation as well as esophagel stenosis
You can make a case that all intentional-suicidal ingestions of caustics should undergo EGD since there should be some injury if ingestion truly occurred or at the least a higher probability. The difficult case is the pediatric unintentional ingestion. Utilizing clinical exam and history will assist with that determination - there is a little research to guide this decision (next pearl)
The attached picture is the post-mortem of a caustic injury showing grade II linear lesions in esophagus with eschar distally and in stomach (Grade III).
A patient arrives via EMS agitated with VS: P 140, BP 155/100, R 18, T 101F. There is an admitted drug exposure and you examine his eyes which are dilated. You shine the light in the eyes - if the pupil reacts, would that be consistent with anticholinergic or sympathomimetic toxidrome?
Answer: Anticholinergic exposure paralyzes pupillary constrictor muscles and causes dilated pupils that do not react to light. Think about when you go to the eye doctor's office. They put homoatropine in your eyes so that when they look with the slit lamp they can see the retina without interference from pupillary constriction. Sympathomimetic exposure like cocaine activates pupillary dilator muscles, the constrictors are still intact and will give a reflexive constriction to light. This patient has reactive pupils and by the mere fact is in Baltimore probability dictates a sympathomimetic exposure like cocaine.
Valproic Acid (Depakote) is a drug that uniquely has the ability to raise serum ammonia concentrations. It is able to do this without raising liver er enzymes and it can occur in overdose or at therapeutic levels. Do not think of this in the context of hepatic encephalopathy. This a metabolic derangement caused by VPA.
In a patient with toxin-induced bradycardia and hypotension, here is a quick differential to help identify the responsible substance:
Less commonly seen causes include: magnesium, propafenone, and plant toxins (aconitine, andromedotoxin, veratrine).
In the state of Maryland, the most common venomous snake is the copperhead. Though not as dangerous as the rattlesnake, it can still cause loss of function of limb and mortality in the pediatric patient.
Treatment has involved the use of CroFab (Protherics, Atlanta). This ovine derived monovalent immunoglobolin is actually made against the following snakes:
Though efficacy has been shown with these snakes, we are hoping for cross-reactivity when we treat copperheads. There are case series and case reports (1) that have shown anectdotal improvement. We are still awaiting a real randomized controlled trial - may never happen.
Physostigmine has been used extensively in the fields of anesthesiology and emergency medicine. The only use of physostigmine with sound scientific support is for the management of patients with an anticholinergic syndrome, particularly those without cardiovascular compromise who have an agitated delirium. In this population, physostigmine has an excellent risk-to-benefit profile.