DOSE VF (DOuble SEquential External Defibrillation for Refractory VF) Trial
Background - High quality data regarding the use of double sequential external defibrillation (DSED) and vector-change (VC) defibrillation in refractory vfib is limited
Study
-Three-group, cluster-randomized, controlled trial in six Canadian paramedic services
-Study population:
-OHCA with refractory vfib (initial presenting rhythm of vfib or pulseless VT that was still present after three consecutive rhythm analyses and standard defibrillations separated by 2 minute intervals of CPR) of presumed cardiac etiology (405 patients)
-Some notable exclusion criteria:
-suspected drug overdose, hypothermia, traumatic cardiac arrest
-Protocol:
-First 3 defib attempts in the standard (anterior-lateral) position
-If remained in vfib after three consecutive shocks randomized to one of:
1. Standard defib for all subsequent attempts (136 pts)
2. VC defib (all subsequent attempts in anterior-posterior position) (144 pts)
3. DSED (applied second set of pads in AP position) with near simultaneously (<1 sec) defib shocks (125 pts)
Results
-Primary outcome: survival to hospital discharge
-38 patients (30.4%) in the DSED group vs. 18 (13.3%) in the standard group (RR 2.21; 95% CI, 1.33 to 3.67) (Fragility index of 9)
-31 patients (21.7%) in the VC group (RR [vs. standard], 1.71; 95% CI, 1.01 to 2.88) (Fragility index of 1)
-Notable secondary outcome: survival with a good neurologic outcome
-34 patients (27.4%) who received DSED vs. 15 patients (11.2%) with standard defibrillation (RR, 2.21; 95% CI, 1.26 to 3.88)
Takeaways/Caveats:
-68% of arrests witnessed, 58% received bystander CPR, median response time of 7.4-7.8 min
-Did not reach planned sample size 2/2 COVID pandemic
-No reporting of post-arrest care (e.g. TTM, PCI)
-Overall rates of survival and good neuro outcome on the higher side even with standard of care
-More/larger studies needed, but can consider DSED for refractory vfib, particularly if you are in a setting without more advanced circulatory support/resources
Airway Pressure Release Ventilation (APRV) is an "advanced" mode of mechanical ventilation that has long been considered a "rescue" mode of ventilation and has recently garnered much more attention during the COVID pandemic. Given the long boarding times of critical care patients in the ED with widespread improvement in sight, I wanted to send out some great resources that have come out recently delineating the difference in thought process between APRV as a "rescue" mode and as a "primary" mode.
Rory Spiegel of EMNerd and former UMMC CCM fellow has recently given a great talk on APRV and its use as a rescue mode of ventilation. See also Phil Rola's recent paper listed on that webpage.
https://emcrit.org/emcrit/aprv-for-lung-rescue/
APRV as a primary mode of ventilation has been used in the STC for years and is often referred to in the literature according to the basic ventilatory philsophy called Time Controlled Adaptive Ventilation. I realize this may be heresy to some and perhaps a curiousity to others. I recommend you take some time to peruse the following resources:
1. Dr. Habashi has done a great deal of work in the basic and translation literature on APRV and TCAV. His recent review dispels many myths and concerns surrounding APRV
Myths and Misconceptions of Airway Pressure Release Ventilation: Getting Past the Noise and on to the Signal - https://www.frontiersin.org/articles/10.3389/fphys.2022.928562/full
2. The TCAV Network has great resources for those who want to do a deeper dive into this topic.
https://www.tcavnetwork.org/
(Can also find their recommended protocols at the Multi Trauma Critical Care education website: https://stcmtcc.com/handouts/)
Arterial line waveform interpretation and troubleshooting are essential skills for any physician caring for critically ill patients. Overdamping and underdamping of the arterial line waveform leads to inaccurate systolic and diastolic blood pressure readings which can lead to unidentified hypertension or hypotension. In addition to scrutiny of the arterial waveform pattern, the square-wave test is a tool to identify overdamped or underdamped arterial lines.
Overdamped arterial waveforms will underestimate systolic blood pressure and overestimate diastolic blood pressure. Underdamping will have the opposite effect and overestimate systolic blood pressure and underestimate diastolic blood pressure. In both cases, the mean arterial pressure (MAP) often remains the same.
The square-wave test is a rapid flush that is applied to the arterial line for approximately 1 second. This rapid high-pressure surge results in vibration and oscillation of the arterial catheter. These oscillations are then read by the pressure transducer and the number and amplitude of these oscillations can be measured. 0 or 1 oscillations is suggestive of overdamping. 3 or more oscillations is suggestive of an underdamped system.
Major causes of an overdamped arterial line waveform include low infusion bag pressure, loose connectors, air bubbles in the tubing, blood clot in the circuit, or kinking of vascular catheter. An underdamped arterial line, however, is caused by overly stiff circuit tubing or a defective transducer.
Scrutiny of the arterial waveform and utilization of the square-wave test can be helpful to both identify erroneous arterial line blood pressure readings as well as suggest likely corrective measures.
Emergency physicians are familiar with posterior reversible [leuko]encephalopathy syndrome as an entity associated with untreated hypertension. It also happens to be a well-documented entity amongst solid organ transplant patients.
While the exact pathophysiology remains unclear, PRES is characterized by posterior subcortical vasogenic edema due to blood-brain barrier disruption, usually in the setting of elevated blood pressure with loss of cerebral autoregulation and/or endothelial dysfunction.
The immunosuppressants used in this population, namely calcineurin inhibitors (CNI) such as tacrolimus and cyclosporine, are thought to contribute most to this endothelial dysfunction and development of PRES in transplant patients, although high-dose corticosteroids, ischemia-reperfusion injury during surgery, and antibiotics have also been implicated.
Presentation of PRES post-transplant:
Clinical symptoms:
Time course:
Diagnostics:
Management:
Bottom Line:
Patients with a history of solid organ transplant are at risk for PRES. While ED stabilization of these patients remains the same, recognition of PRES as a potential etiology for a transplant patient's presentation is crucial to proceed with important testing and necessary changes to their immunosuppressive regimen.
Needless to say, therapeutics for COVID-19 pneumonia have been controversial. From hydroxychloroquine to ivermectin to remedesivir to steroids to bleach (sorry, but it had to be said...), it depends on who you ask whether medications make a difference in COVID, how much of a difference, when they should be given, and what the correct dose is.
Dexamethasone, however, ala the RECOVERY trial, is one of the relatively few therapies supported by the majority of the literature and guidelines, and generally is recommended when respiratory support is required for COVID-19 pneumonia. Further add to this that steroids for ARDS is a long-running point of critical care controversy (e.g. DEXA-ARDS, Meduri, etc), and all you need to say to an intensivist is "how much steroid should I give this patient?" and you can walk away and come back 10 minutes later to find them having not noticed you had ever left.
Wu et all did a fairly small (n=107) single-centered RCT looking at dexamethasone 6 mg daily vs dexamethasone 20 mg daily for COVID-19 requiring O2. There are several notable limitations to this study, but in short it did NOT add support to the notion that higher dose dexamethasone is a good thing for COVID-19 pneumonia. In fact, the 20 mg group trended towards worse outcomes. Small sample size, single-center, limited follow up, variable use of biologics between the groups, and failure to investigate intermediate doses between 6 and 20 are all significant limitations of this trial. Of note, DEXA-ARDS, which was conducted before COVID (2013-2018), looked at 20 mg x 5 days followed 10 mg x 5 days and DID find a significant benefit, as well as pretty darn good NNT and p values (and was a higher quality trial), so in my opinion it is also not unreasonable to use DEXA-ARDS dosing if the patient meets moderate-severe ARDS (P:F < 200) criteria, even though of course DEXA-ARDS was before COVID and Wu et al slightly contradicts it.
When faced with a very sick COVID-19 pneumonia patients many intensivists will do either RECOVERY or DEXA-ARDS dexamethasone (with relatively limited basis to choose one vs the other), and some will do Meduri protocol methylprednisolone (1-2 mg/kg/day). Relatively few nowadays will omit steroids unless there's a contraindication.
Bottom Line: It probably remains a good idea to give dexamethasone to your COVID-19 pneumonia patients with hypoxia, but you can probably stick to RECOVERY (see reference below; 6 mg daily x 10 days) dosing as opposed to higher doses. If they're REALLY sick (P:F < 200), consider DEXA-ARDS (20 mg x 5 days followed by 10 mg x 5 days) dosing.
Optimal Timing of Source Control in Sepsis
Enter the WATERFALL trial into the present flood of fluid strategy trials, a multi-country (primarily Spain) open-label RCT of “Aggressive” versus “Moderate” fluid resuscitation with lactated ringers for early mild acute pancreatitis.
Population: 249 adults (1/3 of the planned enrollment) presenting to the ED within 24hrs hours of abdominal pain onset diagnosed with mild acute pancreatitis. Numerous exclusions for local pancreatic complications, acute or chronic organ dysfunction (including CHF and CKD), among many others. Average age of 57, 51% female, 61% due to gallstones, median Charleson index of 2, median BISAP of 1, and 52% clinically judged hypovolemic on enrollment.
Interventions: 1:1 randomization to two complex protocols, both with time points every 48 hours and same criteria for initiating oral diet.
Outcomes/Results: Primary outcome was development of moderate of severe pancreatitis with no difference found between the two strategies. Median fluid at 72 hours was 8.3L (IQR 7.1- 10.8) in the aggressive arm and 6.6L (IQR 4.1 - 8.0) in the moderate arm. Several point estimates favor the moderate group, but none statistically significant and there was not a difference in symptom or SIRS improvement at 72 hours. The trial was stopped after 1/3 enrollment when the monitoring board noted a significantly increased rate of fluid overload in the aggressive arm (20.5%) versus the moderate arm (6.6%).
Discussion:
-Aggressive fluids for mild acute pancreatitis didn’t show benefit over a moderate strategy and showed some harms in contrast to previous smaller studies and some guideline recommendations in mild disease
-Only reached 1/3 of target enrollment significantly limiting analysis
-This was by design not a trial of severe or critical disease
-The open label nature may have affected some endpoints, including safetly endpoints
-Another trial to shift our thinking a bit about how to use and safely limit fluid resuscitation
Have you ever encountered an ESRD patient who missed dialysis because the patient "felt too sick to go to dialysis"? The patient then had hypotension from an infected catheter line? Do we give 30 ml/kg of balanced fluid now?
__________________________
Title: Outcomes of CMS-mandated ?uid administration among ?uid-overloaded patients with sepsis: A systematic review and meta-analysis.
Settings: This is a meta-analysis
Patients: Septic patients who have underlying fluid overload conditions (CHF or ESRD).
Intervention: intravenous fluid administration according to the mandate by the Center for Medicare/Medicaid as 30 ml per kilograms of bodyweight.
Comparison: fluid administration at less than 30 ml/kg of body weight.
Outcome: 30-day mortality, rates of vasopressor requirement, rates of invasive mechanical ventilation
Study Results:
Discussion:
Conclusion:
Point-of-care ultrasound compression of the carotid artery for pulse determination in cardiopulmonary resuscitation
Background:
Take Home:
This is essentially a secondary analysis of a previous prospective observational cohort study with high quality methods. The authors have an excellent discussion of the previous studies on this topic (which for those with an interest I highly recommend you read). They conclude that this study supports previous literature which I would think would be seemingly obvious, which is that those who are more ill to begin with have less tolerance of propofol (in a dose-independent relationship) in this and previous studies. Their use of IPTW extends the analysis on this large international population by addressing confounders in a novel way.
Their overall conclusion is that propofol is bad for the critically ill, and especially bad for those with pre-existing risk factors for intubation complications. I agree: This study suggests in even stronger terms that propofol should be used carefully and probably only in unhealthy patients when other options are unavailable.
Study Background and Characteristics
Findings
Traditionally, internal jugular and subclavian central line placement has required chest x-ray confirmation of correct placement (venous cavoatrial junction placement) as well as demonstrating lack of complication (no pneumothorax) prior to use of that central line. However, current evidence supports similar if not superior complication identification and placement confirmation with ultrasound,(1-7) allowing for a much quicker confirmation time than traditional chest x-ray, which can be vital in critically ill patients who need immediate medication administration.
Venous placement is confirmed with prompt visualization of microbubbles in the right atrium and ventricle with a rapid flush of 5-10 ml of agitated saline via the distal central line port. Additionally, if the opacification occurs <2 seconds after injection then the catheter tip is sufficiently distal in the central venous system to not require additional verification. Additional confirmation of lung sliding in both lung apices will rule out pneumothorax.
Some authors recommend checking the contralateral internal jugular vein to ensure that the central line catheter has not traveled up the internal jugular towards the head, however this may be redundant as long as the time from agitated saline injection to right atrial visualization of microbubbles is clearly less than 2 seconds.
Bottom Line: Utilization of ultrasound for central line placement confirmation is a relatively simple, rapid, safe, and accurate means of confirmation of venous catheter placement and catheter tip location, as well as ruling out pneumothorax complications.
Deep sedation in the ED has previously been associated with longer duration of mechanical ventilation, longer lengths of stay, and higher mortality.1 Current guidelines recommend light sedation, consistent with a goal RASS of -2 to 0, for most critically-ill patients in the ICU.2
The ED-SED3 multicenter, pragmatic, before-and-after feasibility study implemented an educational initiative (inservices, regular reminders, laminated sedation charts) to help target lighter sedation depths in newly-intubated adult patients without acute neurologic injury or need for prolonged neuromuscular blockade.
After educational intervention:
Even with the caveats of the confounding and bias that can exist in before-and-after studies, these results are consistent with prior sedation-related studies and offer more evidence to support for avoiding deep sedation in our ED patients. The study also demonstrates the importance of nurse-driven sedation in achieving sedation goals.
Bottom Line: Our initial care in the ED matters beyond initial stabilization and compliance with measures and bundles. Avoid oversedating intubated ED patients, aiming for a goal RASS of -2 to 0.
We previously posted on the COCA trial, which looked at empiric calcium administration in cardiac arrest. They studied 391 adult Danish cardiac arrest patients. The immediate and 30 day outcomes showed no benefit, and in fact strongly trended towards calcium being WORSE than placebo. This article provides the 6 month and 1 year follow up data. Surprise, surprise... calcium is still not looking good.
At 6 months survival non-significantly favored the placebo group, and at 1 year it significantly favored the placebo group. Neurologic outcome for those who survived was also no better, and perhaps slightly worse, in the calcium group.
Importantly, the trial excluded patients with "traumatic cardiac arrest, known or suspected pregnancy, prior enrollment in the trial, adrenaline prior to possible enrollment, and clinical indication for calcium at the time of randomization."
Bottom Line: The evidence continues to not support the routine empiric administration of calcium in cardiac arrest. Patients in whom there is an indication to give calcium (e.g. known ESRD, suspected hyperkalemia, etc) are excluded from these trials, and should likely still receive empiric calcium, but in undifferentiated cardiac arrest you can probably skip the calcium.
Diastolic Blood Pressure
Hemodynamic instability and cardiac arrest are major complications following endotracheal intubation. The mantra “resuscitate before you intubate” has prompted several studies of how to prevent this.
The PREPARE II trial is a multicenter ICU-based trial studying the effect of 500cc of crystalloid versus no crystalloid pre-emptively to prevent hypotension following endotracheal intubation. The study enrolled 1067 critically ill patients in United States ICUs. Some 60% of patient were intubated for respiratory failure and 20% were already on vasopressor. The primary induction drugs we etomidate and rocuronium. Importantly, urgent intubation was an exclusion. There were no differences in multiple endpoints including hypotension, new need for vasopressors, cardiac arrest, or 28-day mortality.
This was in some ways this in not unexpected and patients already in an ICU setting have typically received some form of fluid loading already. Being ICU based and primarily a more smoldering medical population this has limited application to more emergent and undifferentiated settings, but study underscores the need for a broad and nuanced view of what “resuscitate” means. Positive pressure may exacerbate hypovolemia, but the patient’s underlying disease, the effect of anesthetic drugs both by direct action via relief of pain, discomfort, or dyspnea may predominate if you think the patient is euvolemic.
Remember to dose anesthetics/sedatives/RSI drugs with an eye toward hemodynamics and consider starting vasopressors prior to intubation
Bottom Line:
-In a broad well-conducted ICU-based study a 500cc peri-intubation bolus doesn’t prevent hypotension
-Have a broad view of what resuscitation for intubation might entail
-Having fluid ready for intubation is helpful, hemodynamic dosing of drugs and having a plan for vasopressors might be even more helpful
-Applicability to ED environments is limited in this ICU-based trial
Have you ever wonder what patients feel after being intubated in the ED?
The study " Awareness With Paralysis Among Critically Ill Emergency Department Patients: A Prospective Cohort Study" aimed at answering just that.
Settings: Emergency Departments from 3 hospitals; This was a secondary analysis of a prospective trial.
Patients:
Patients who received neuromuscular blockade in ED
Intervention: None.
Comparison: None.
Outcome: Primary outcome was Awareness while paralyzed, secondary outcome was Perceived threat, which is considered the pathway for PTSD.
Study Results:
The study evaluated 388 patients. There were 230 (59%) patients who received rocuronium.
Patients who received rocuronium (5.5%, 12/230) were more likely to experience awareness than patients receiving other neuromuscular blockade (0.6%, 1/158).
Patients who experienced awareness during paralysis had a higher threat perception score that those who did not have awareness (15.6 [5.8] vs. 7.7 [6.0], P<0.01).
A multivariable logistic regression, after adjustment for small sample size, showed that Rocuronium in the ED was significantly associated with awareness (OR 7.2 [1.39-37.58], P = 0.02).
Discussion:
With the increasing use of rocuronium for rapid sequence intubation in the ED, clinicians should start to pay more attention to the prevalence of awareness during paralysis. According to the study, patients reported pain from procedures, being restrained, and worst of all feelings of impending death.
One of the risk factors for awareness during paralysis would be the long half-life of rocuronium, compared to that of succinylcholine. Therefore, clinicians should consider prompt and appropriate dosage of sedatives for post-intubation sedation. Previous studies showed that a mean time from intubation till sedatives was 27 minutes (2), and propofol was started at a low dose of 30 mcg/kg/min for ED intubation (3).
Conclusion:
Approximately 5.5% of all patients or 4% of survivors of patients who had invasive mechanical ventilation in the ED experienced awareness during paralysis. They also were at high risk for PTSD.
Tachyarrhythmias in the setting of high-dose vasopressors due to septic shock are not uncommon. Aside from amiodarone, some providers may not know of alternative therapeutic options in the setting of septic shock. In addition, some may view the use of a beta-blocker as counter-intuitive or counter-productive in the setting of norepinephrine usage.
However, there have been multiple smaller studies evaluating using esmolol (and other short-acting beta-blockers) in the setting of tachycardia, septic shock and pressors. Outcomes regarding the theoretical benefits of beta-blockade in sepsis (i.e. decreased mortality/morbidity 2/2 decreased sympathetic innervation, inflammation, myocardial demand etc.) have been varied. However, esmolol has been demonstrated multiple times to be effective at reducing heart rate without significant adverse outcomes (i.e. no sig diff in mortality, refractory shock, or time on vasopressors).
Caveats/pitfalls
-most of the studies discuss “adequate resuscitation” prior to initiation of esmolol
-not studied in patients that also had significant cardiac dysfunction
-be aware that esmolol gtts can be a lot of volume and pts can become volume overloaded if boarding in the ED for an extended period of time
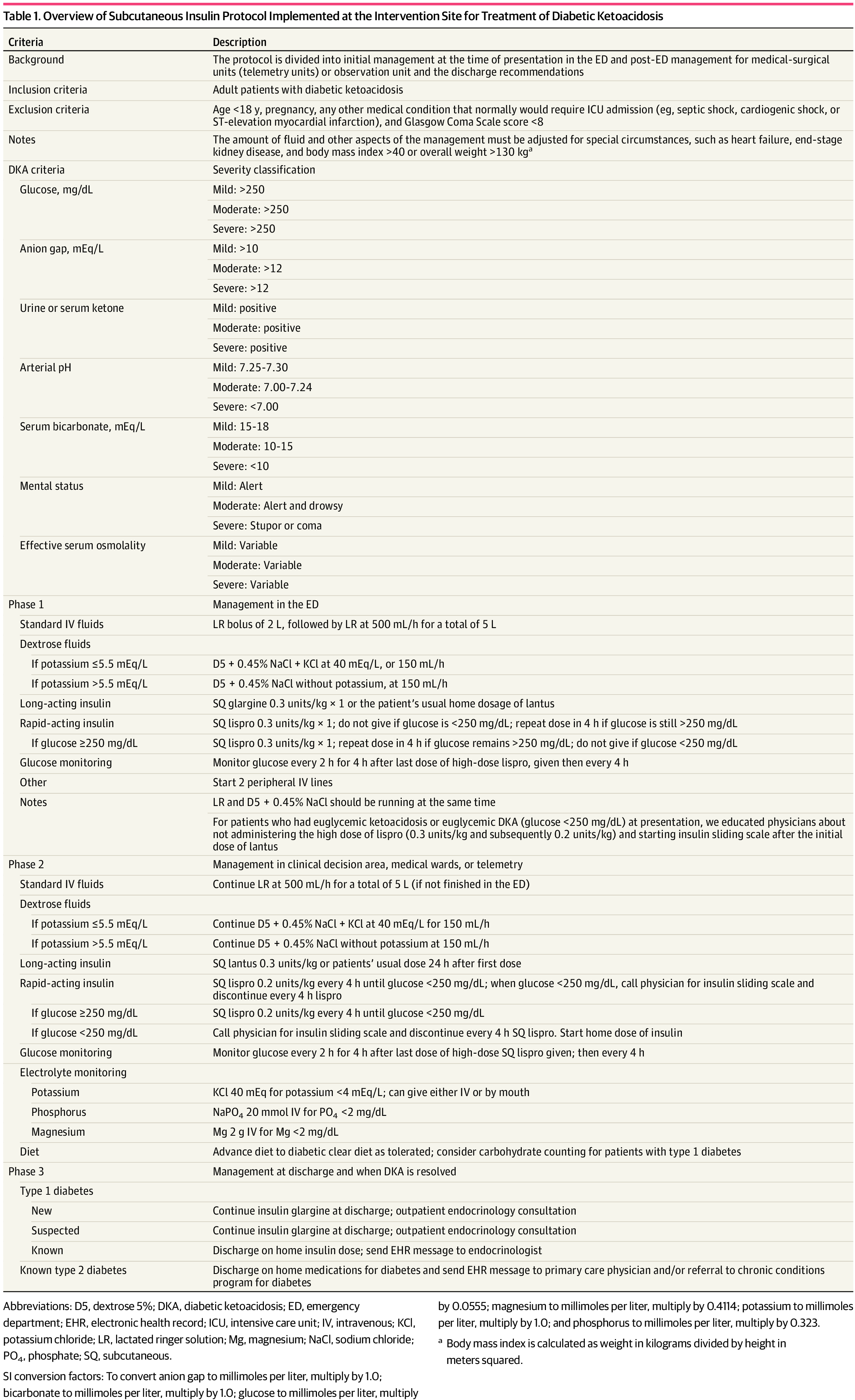
Background: It is classically taught that the tenets of DKA management are IV fluids, electrolyte repletion, and an insulin infusion that is titrated until approximately 2 hours after anion gap closure, when long-acting subcutaneous insulin is administered if the patient is tolerating oral intake. It has been previously found that earlier administration of subcutaneous long-acting insulin can shorten the time to anion gap closure, while other small studies have noted similar efficacy in subcutaneous insulin compared to IV in mild/moderate DKA.
A recent JAMA article presents a retrospective evaluation of a prospectively-implemented DKA protocol (see "Full In-Depth" section) utilizing weight-based subcutaneous glargine and lispro, rather than IV regular insulin, as part of initial and ongoing floor-level inpatient treatment.
When compared to the period before the DKA protocol:
The only exclusion criteria were age <18 years, pregnancy, and presence of other condition that required ICU admission.
Bottom Line: Not all DKA requires IV insulin infusion.
At the very least, we should probably be utilizing early appropriate-dose subcutaneous long-acting insulin. With ongoing ICU bed shortages and the importance of decreasing unnecessary resource use and hospital costs, perhaps we should also be incorporating subcutaneous insulin protocols in our hospitals as well.
Although it is well-documented that there is no true "maximum" dose of vasopressor medications, further blood pressure support as doses escalate to very high levels tends to be limited. As such, debate has raged in Critical Care as to when is the "right" time to start a second vasoactive medication. The VASST trial (Russell et al, NEJM, 2008) is considered to be the landmark trial in this area, and found a trend towards improvement with early addition of vasopressin to norepinephrine, but no statistically significant difference, and may have been underpowered.
Partly as a result of VASST, the pendulum has tended to swing towards maximizing a single vasoactive before adding a second over the past decade. The relatively high cost of vasopressin in the US has also driven this for many institutions. However, more recently a "multi-modal" approach, emphasizing an earlier move to second, or even third, vasoactive medication, is increasingly popular. Although cost is often prohibitive for angiotensin-2 given controversial benefits, many now advocate for targeting adrenergic receptors (e.g. with norepinephrine or epinephrine), vasopressin receptors (e.g. with vasopressin or terlipressin) and the RAAS system (e.g. with angiotensin 2) simultaneously in patients with refractory shock. A recent review by Wieruszewski and Khanna in Critical Care (see references) outlines this approach well.
Bottom Line: When to add a second vasoactive medication (e.g. vasopressin) for patients with refractory shock after a first vasoactive is controversial and not known. Current practice is trending towards earlier addition of a second (or third) agent, especially if targeting different receptors, but there is limited high-quality evidence to support this approach. Many practicioners (including this author) still follow VASST and consider vasopressin once doses of around 5-15 micrograms/min (non-weight based) of norepinephrine are reached.
Vasopressor Tips in the Critically Ill