A ~55 year-old female with a history of ESRD and diabetes who presented to the ED with progressively worsening foot odor. An x-ray was performed. The picture below shows the right foot.
What is the diagnosis?

Haloperidol has a higher D2 receptor antagonist effect than standard antiemetic treatment agents such as metoclopramide. In addition, newer antipsychotic agents such as Olanzapine have a high affinity at multiple antiemetic sites such as the dopamine and serotinergic receptors.
While formal RCT's are still in the works, multiple sources including palliative care, emergency medicine, and pain journals support their use in refractory emesis.
Consider Haloperidol 3-5 mg IV.
Check an EKG for long QTc prior to use. Consider dose reduction of haloperidol in those with hepatic impairment. Also consider dose reduction in patients taking carbamazepine, phenytoin, phenobarbital, rifampicin, or quinidine due to that pesky CYP3A4 inhibition.
Consider Olanzapine 2-5 mg IV.
Several case reports have shown a higher rate of success with olanzapine for refractory emesis. Olanzapine has similar precautions as those to haloperidol (EKG, hepatic impairment), although it's CYP drug interactions are less common. Additionally, use olanzapine cautiously in hyperglycemic patients as there are several case reports of olanzapine prompting episodes of DKA. Consider frequent blood sugar checks or small doses of insulin in hyperglycemic patients.
Take Home Points:
Consider the antipsychotic agents Haloperidol or Olanzapine for patients with refractory emesis, they may be more effective than traditional antiemetics.
Get an EKG prior to administration to check for QTc prolongation. As the classical and atypical antipsychotic agents are sedating, use caution in conjunction with other sedating medications (such as benzodiazepines).
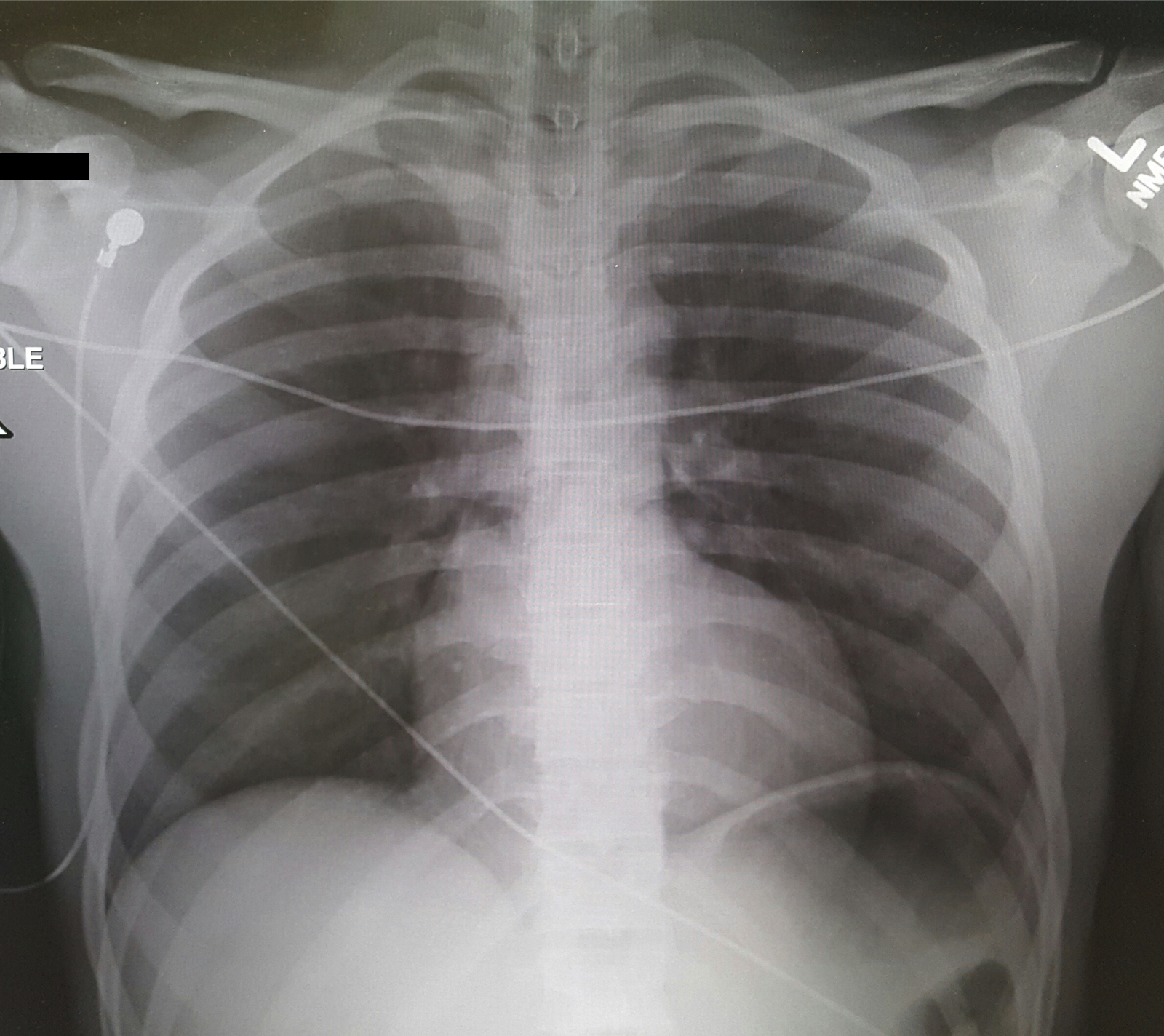
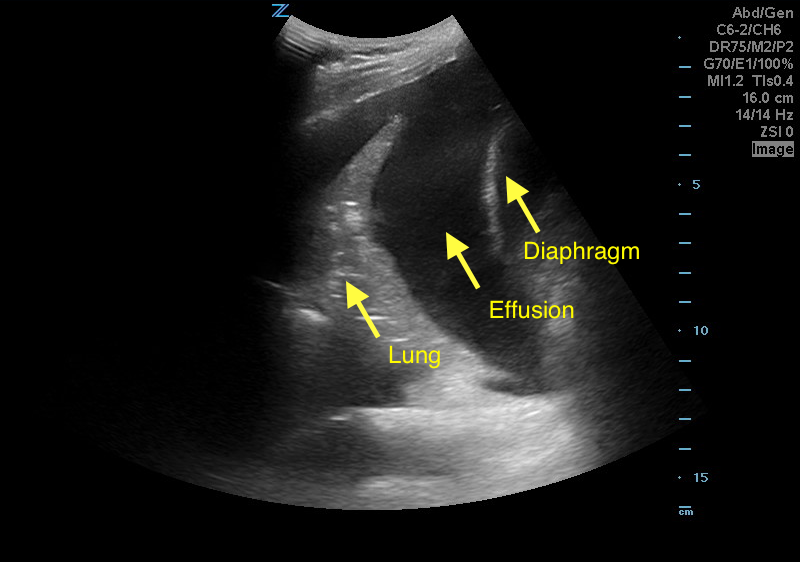
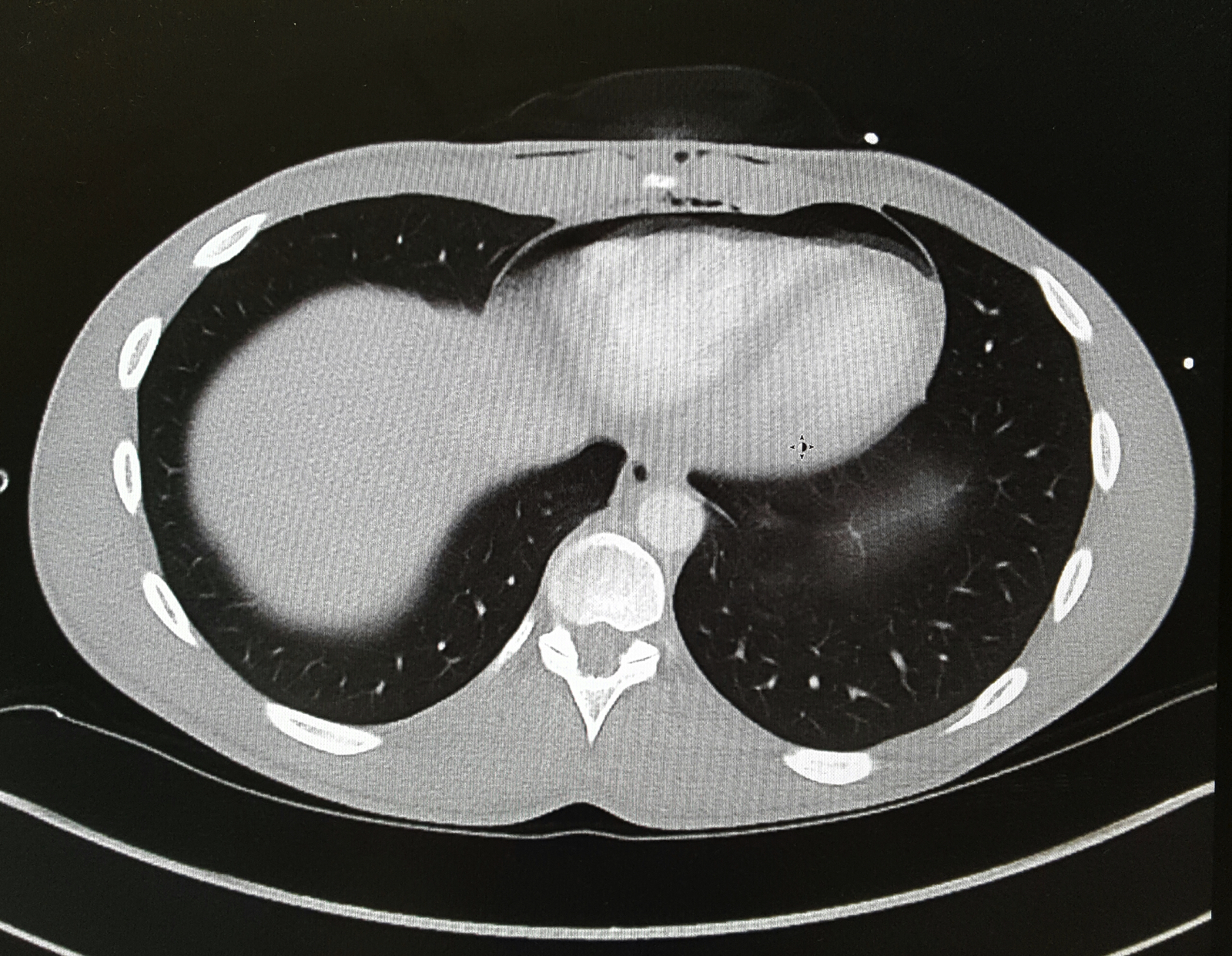
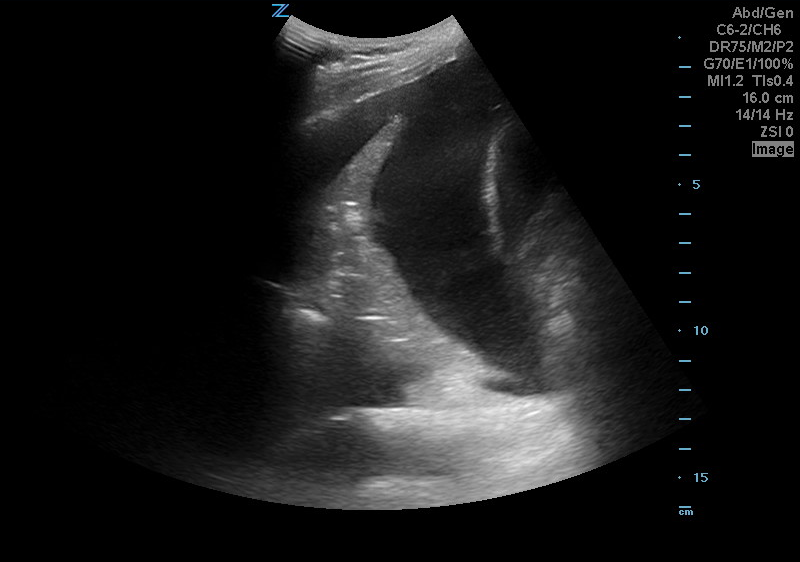
A 50 years old male with a history of CHF, presenting to the ED with progressively worsening shortness of breath. POCUS was performed. The picture shows the left lower part of the chest. What is the diagnosis?
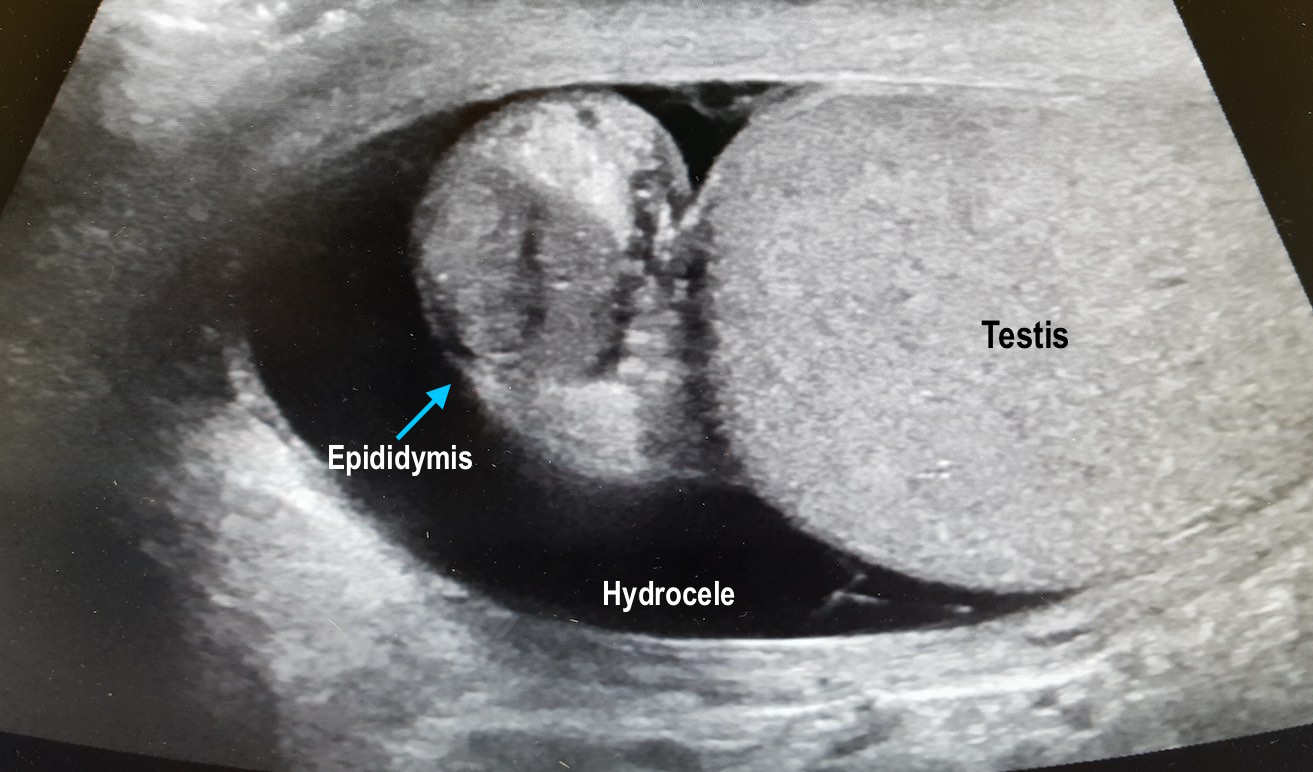
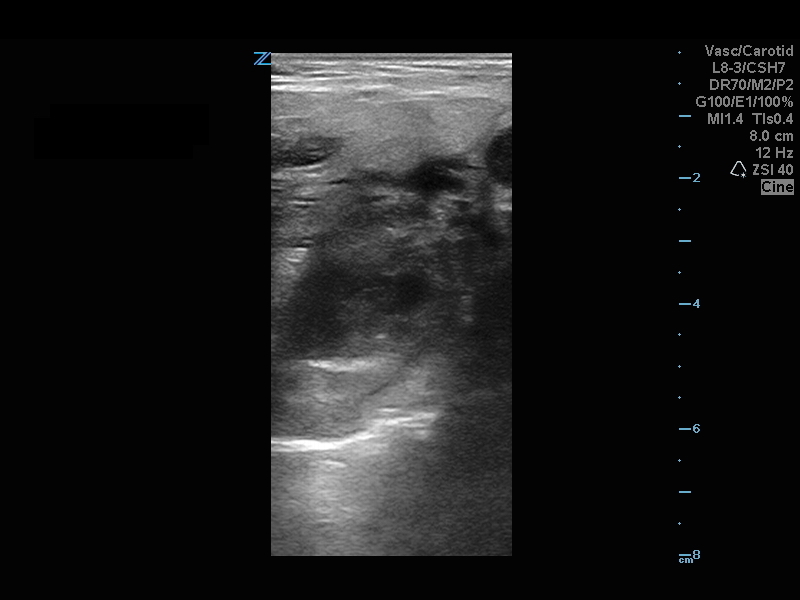
56 year-old male with history of hypertension presents with complaints of right scrotal swelling and pain. Denies any urinary symptoms, abdominal pain, nausea/vomiting or change in bowel habits or prior episodes. Temp was 99.0.
A scrotal ultrasound was done and an image of the right testis was seen (below). What's the diagnosis?
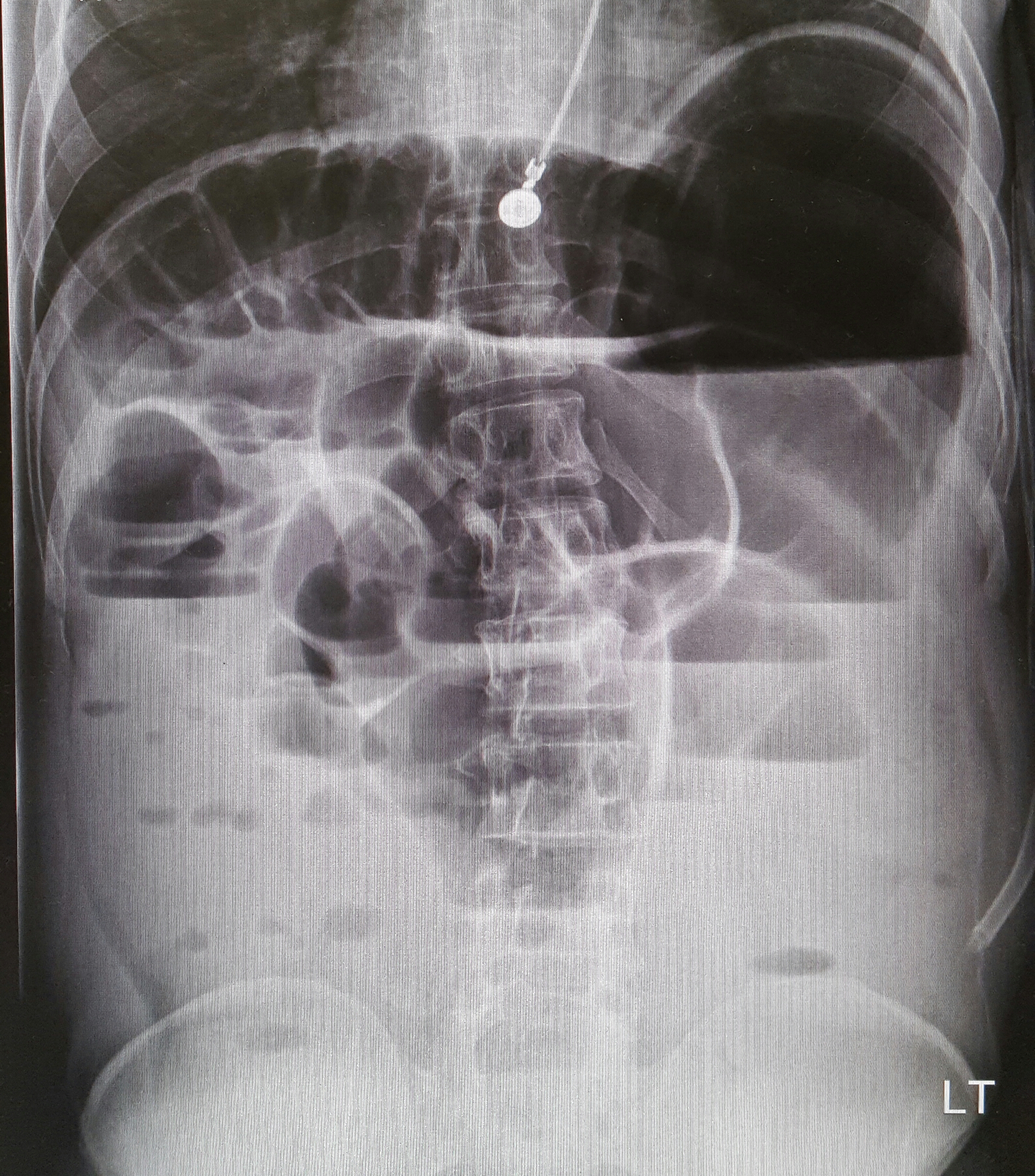
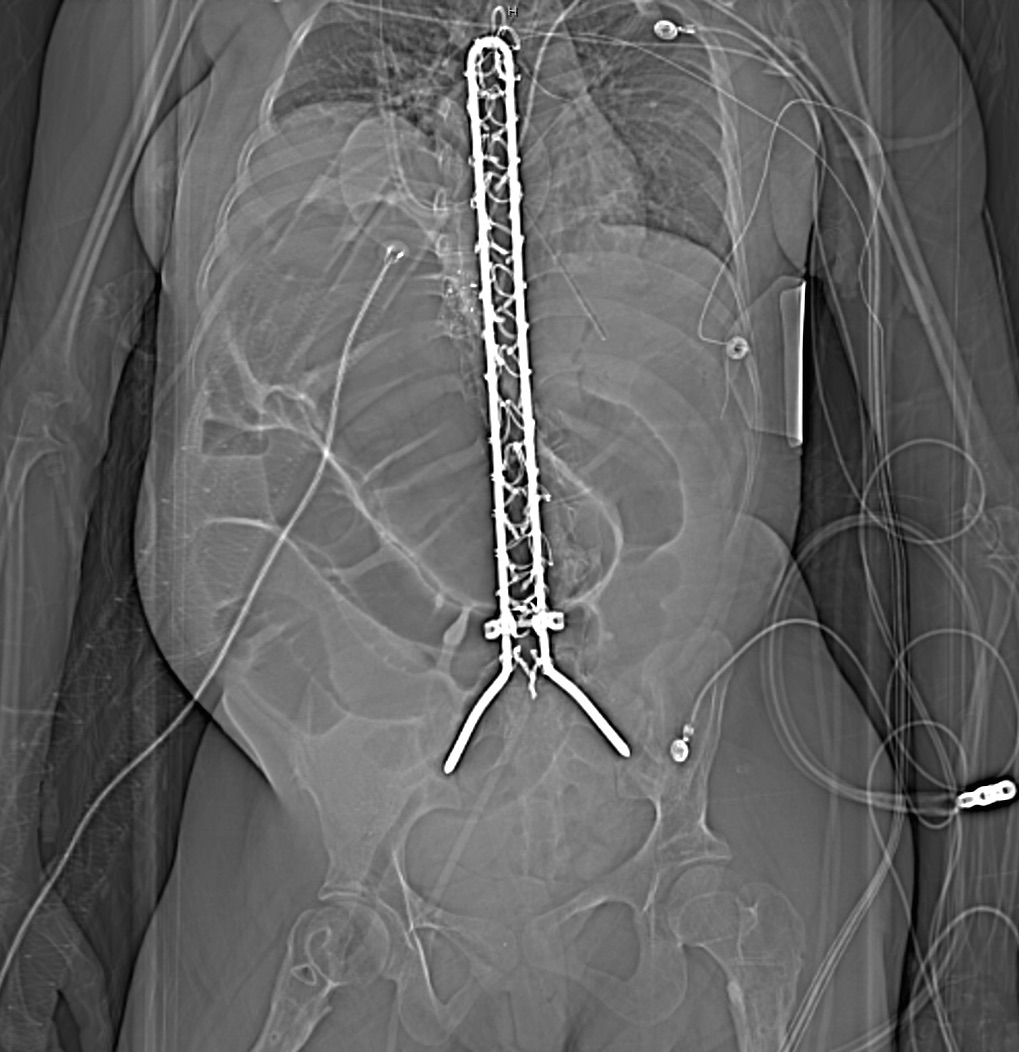
25 year-old female with hx of cerebral palsy with significant developmental delay, s/p G-tube who presented with acute hypoxic respiratory failure, hypotension and a distended, tense abdomen. A CT was done with the scout film below. What's the diagnosis?
A 60 year-old man with history of atrial fibrillation, CAD presents with left lower leg/foot pain for a few days. His foot is seen below. What's the diagnosis?


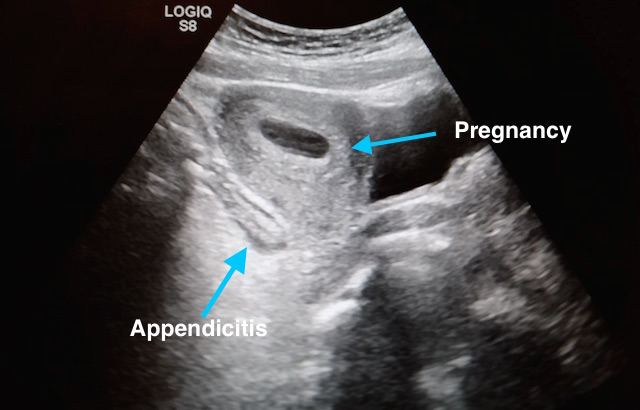
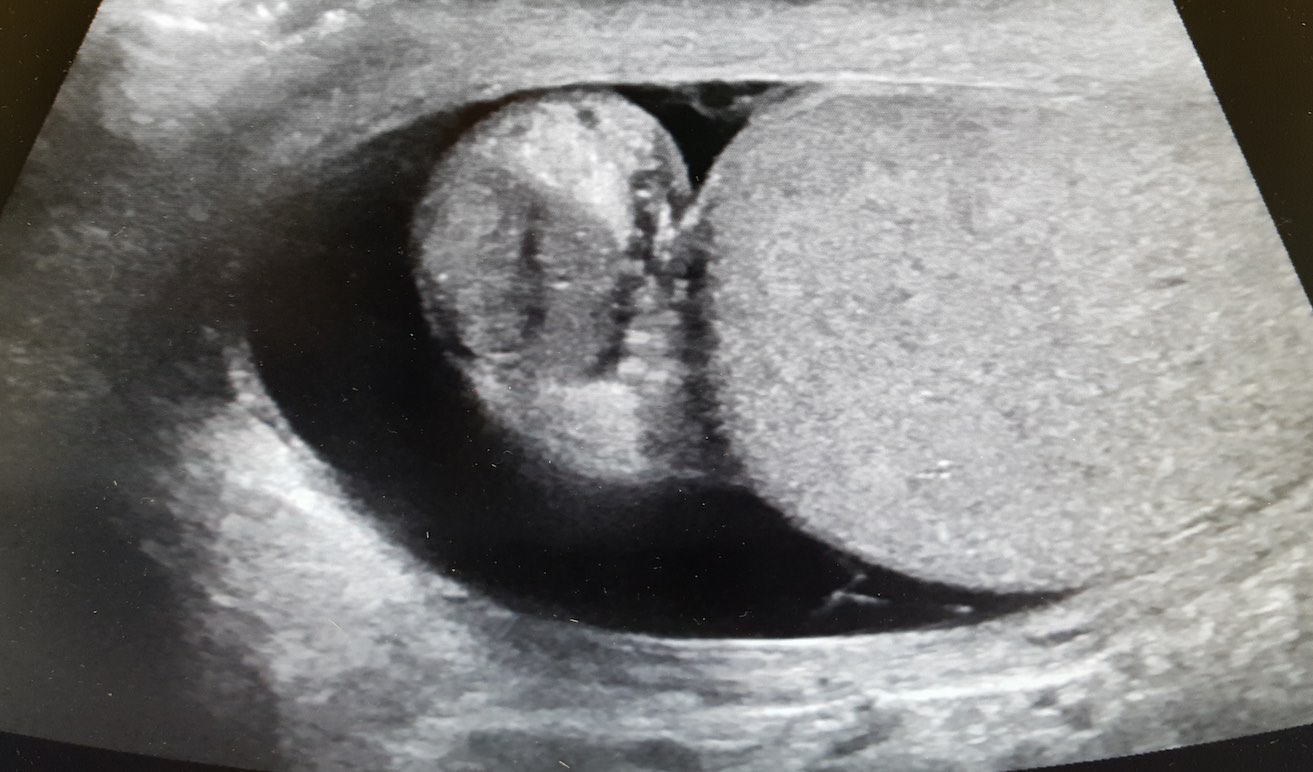
27 year-old G2P1 presents with 3 days of abdominal pain that is mostly suprapubic. Denies any urinary symptoms and vaginal bleeding. Physical examination reveals slight rebound in the right lower quadrant.
An ultrasound revealed the following. What's the diagnosis?

8 year-old female with no PMH who presents with concerns for "purple patches" popping up on her arm for 2-3 days. Stated that one appeared and then, the other one appeared 12 hours later. She denied any trauma whatsoever, history of easy bleeding/bruising and did feel safe at home. The rest of the review of systems was negative.
Patient said there was mild pain when the area was touched. The rest of the physical examination was normal.
What's the diagnosis? (Image below)

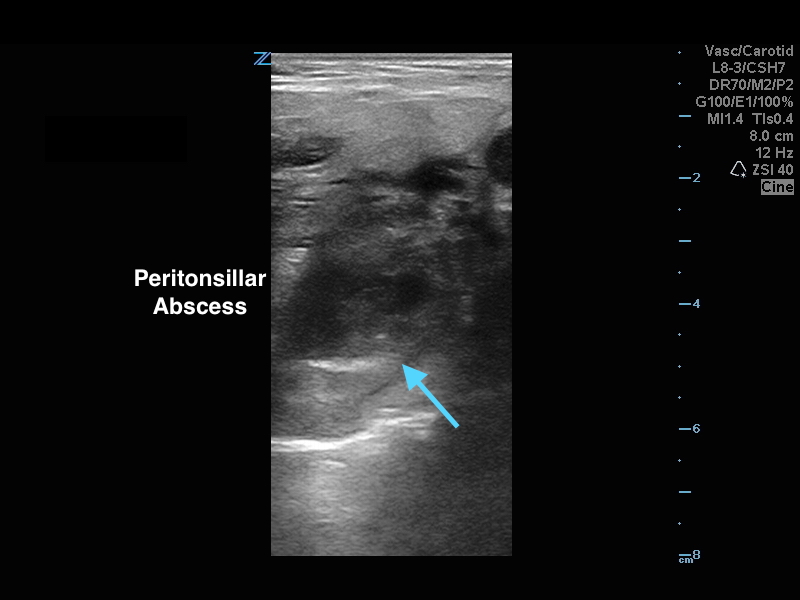
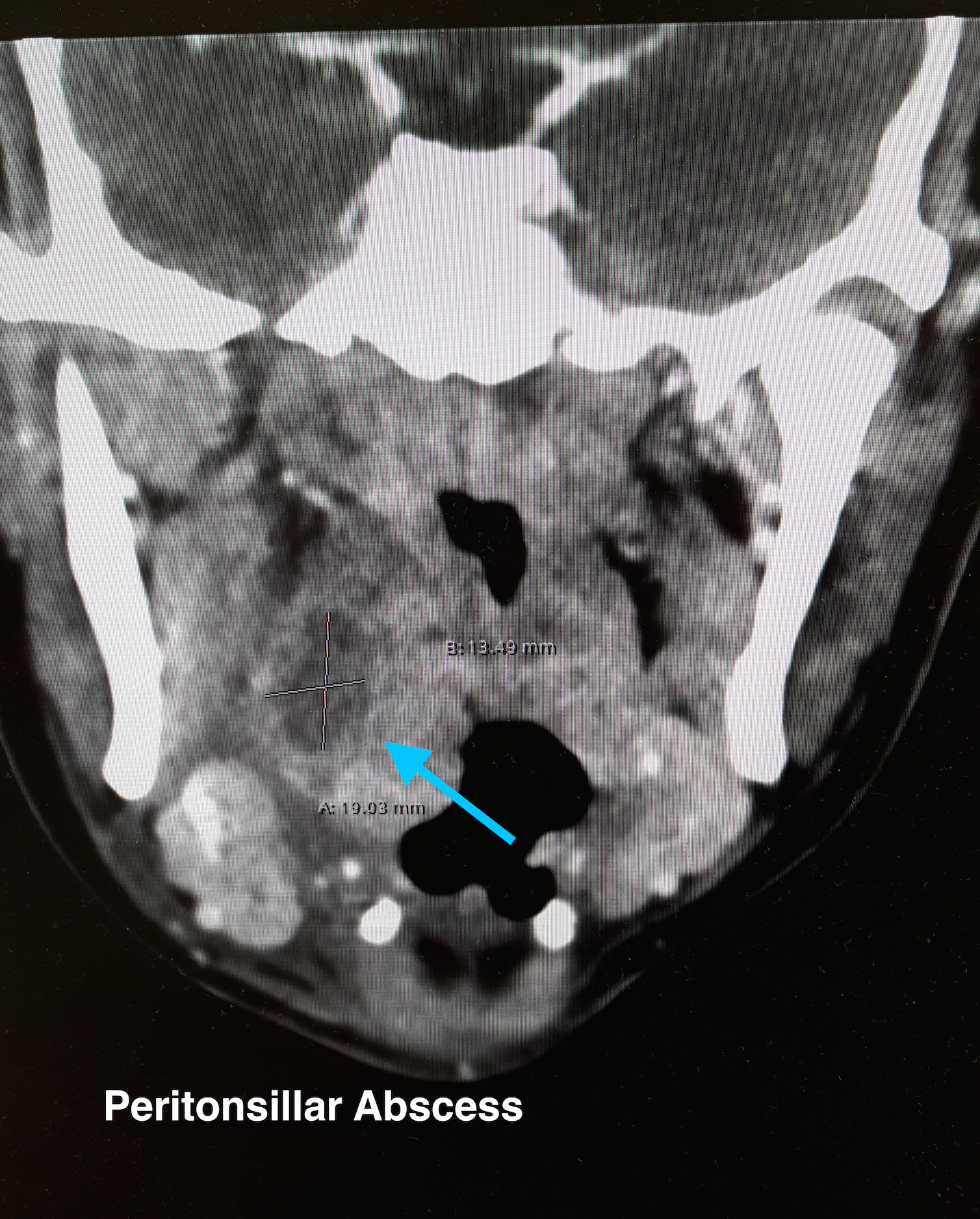
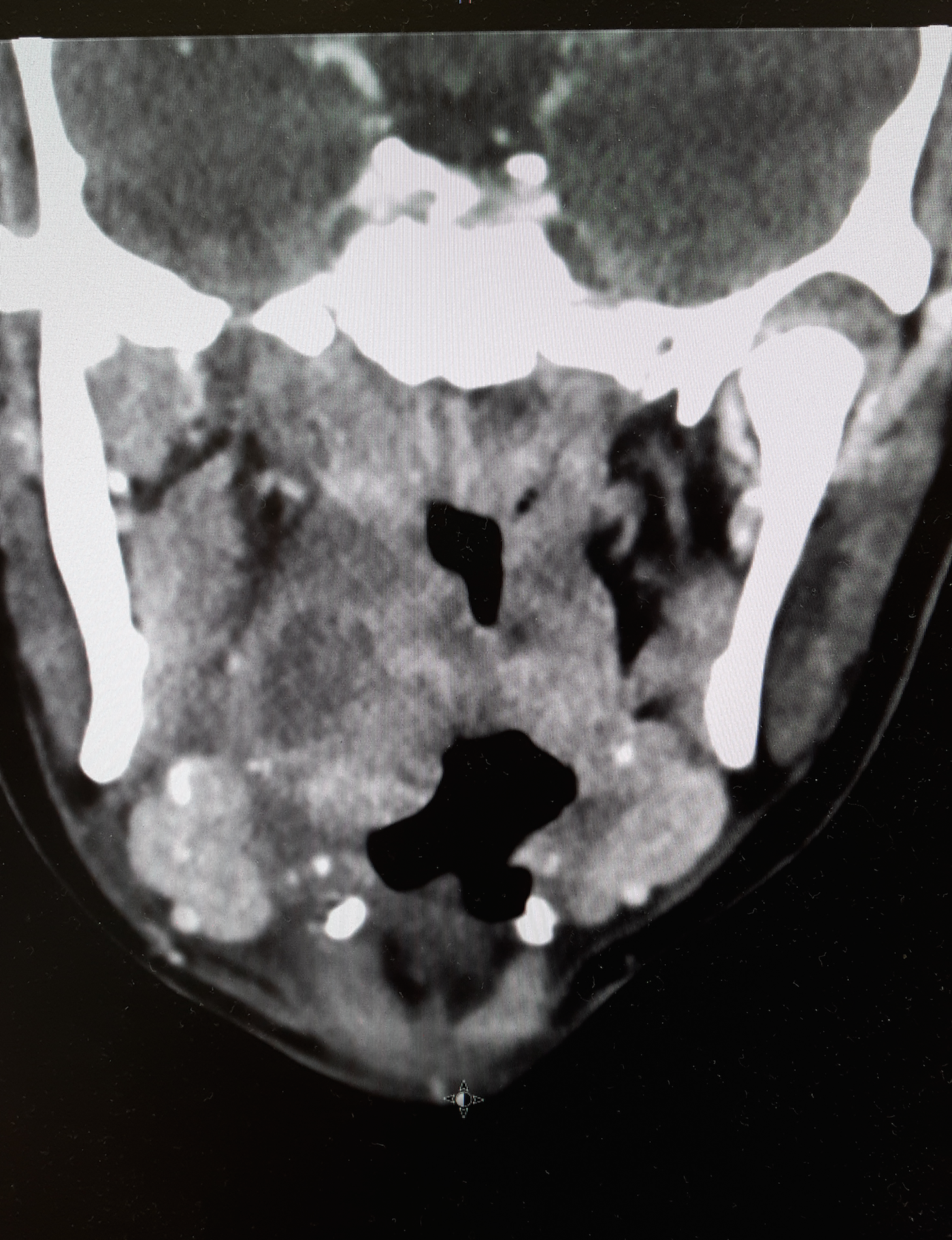
20 year-old female presents with sore throat, right throat fullness, difficulty speaking for 2-3 days. A bedside ultrasound and subsequent CT was obtained as seen below. What's the diagnosis?
57 year-old female with history of bilateral lung transplants presents with fever, and 2 days of a painful, red, bumpy rash over the left labia and left buttock, but also notes a small tender area on the plantar surface of the left foot.
Below is a figure depicting the location of the rash, as well as a photo of her foot.
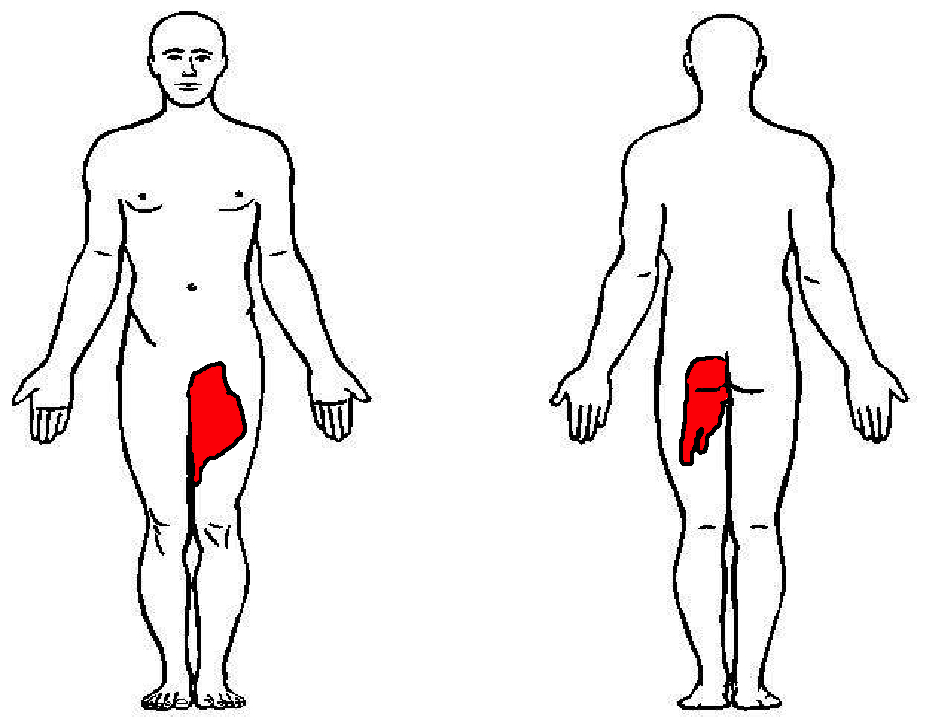
%20copy%201.JPG)
22-year-old male with history of autism, mental retardation who is non-verbal presents with abdominal pain and vomiting for one day. Patient was found clutching his abdomen and moaning. What's the diagnosis?
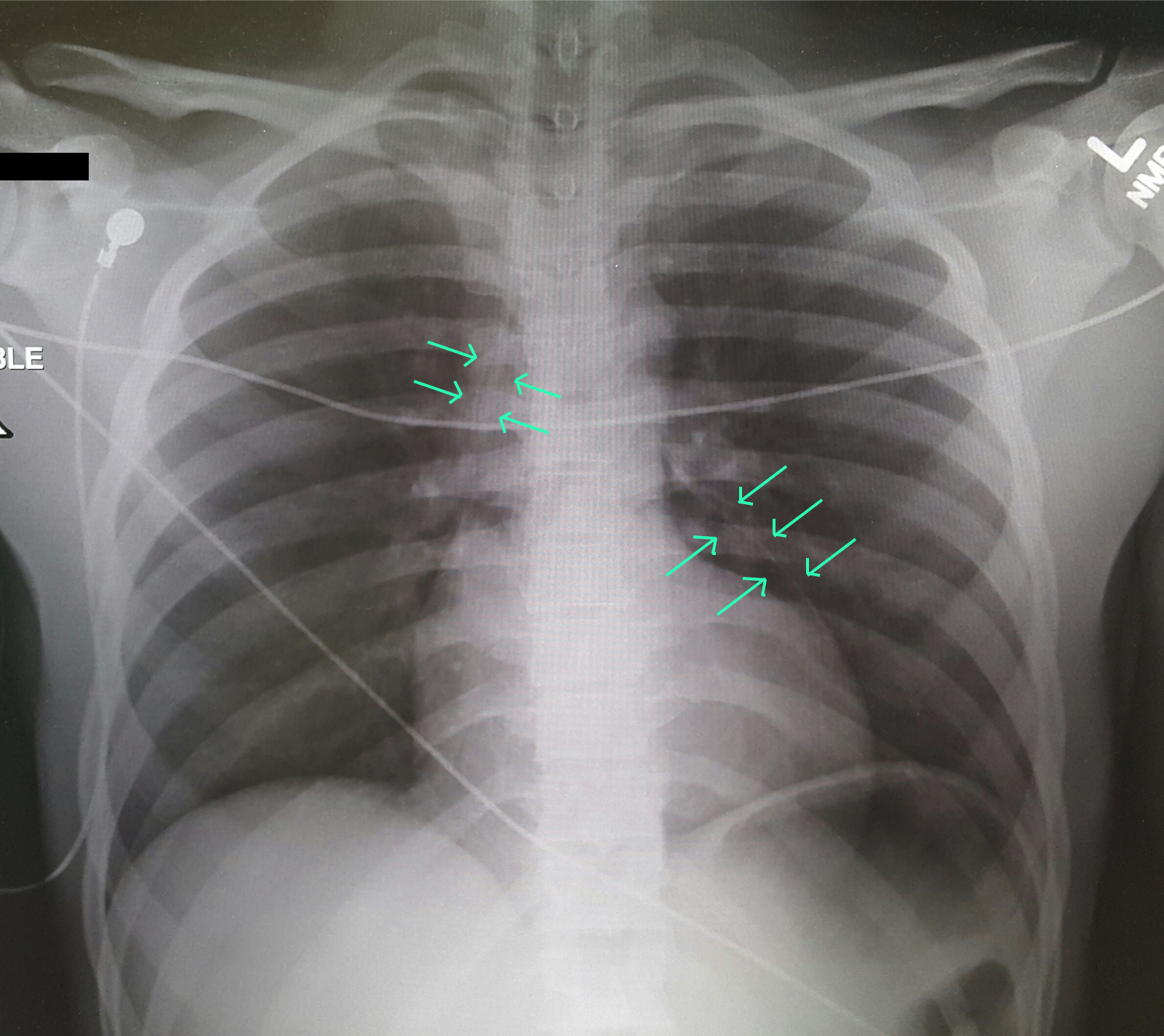
A 25-year-old male was brought in by EMS with a stab wound to the chest. What's the diagnosis?