Bonus pearl: Types of Jaundice by Age
- < 24 hrs: hemolyis, TORCH, bruising from birth trauma (ie- cephalohematoma), acquired infection
- Day 2-3: Physiologic
- Day 3-7: infection, congenital diseases, TORCH
- >1 week: Breast Milk Jaundice, breast feeding jaundice, drug hemolysis, hypothyroidism, biliary atresia, hepatitis, red cell membrane disorders (SS, HS, G6PD deficiency)
CIWA-Ar (Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised)
The use of a scoring system for the disposition of an ethanol withdrawal patient can be helpful. The CIWA-Ar Score can guide both treatment in the ED as well as admission versus discharge. Most studies have verified that a score of <8 can be treated outpatient; 8-15 requires treatment and >15 wil require admission/IV benzodiazepines.
N/V: 0-7 (None to Constant N/V)
Tremor: 0-7 (None to Severe even with arms not extended)
Sweats: 0-7 (None to Drenching Sweats)
Anxiety: 0-7 (None to panic attack/delirium)
Agitation: 0-7 (None to pacing/thrashing during interview)
Tactile Disturbance: 0-7 (Mild itching to Continuous Hallucinations)
Auditory Disturbances: 0-7 (None to Continuous Hallucinations)
Visual Disturbances: 0-7 (None to Continuous Hallucinations)
Headache: 1-7 (Miild to Extremely Severe)
Orientation: 0-4
Go to this website to see the actual tool and how it should be administered:
http://www.regionstrauma.org/blogs/ciwa.pdf
Steroids and Septic Shock
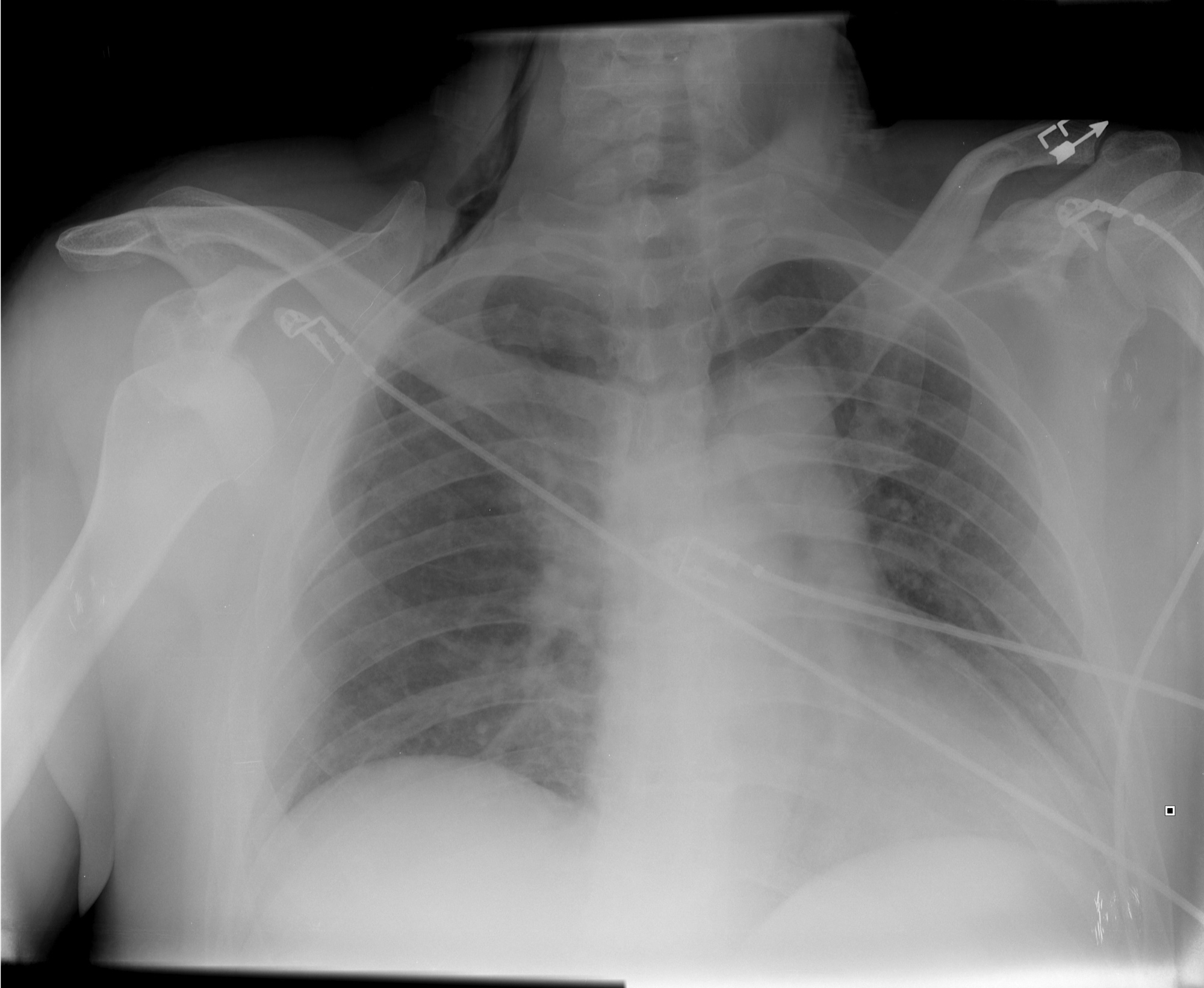
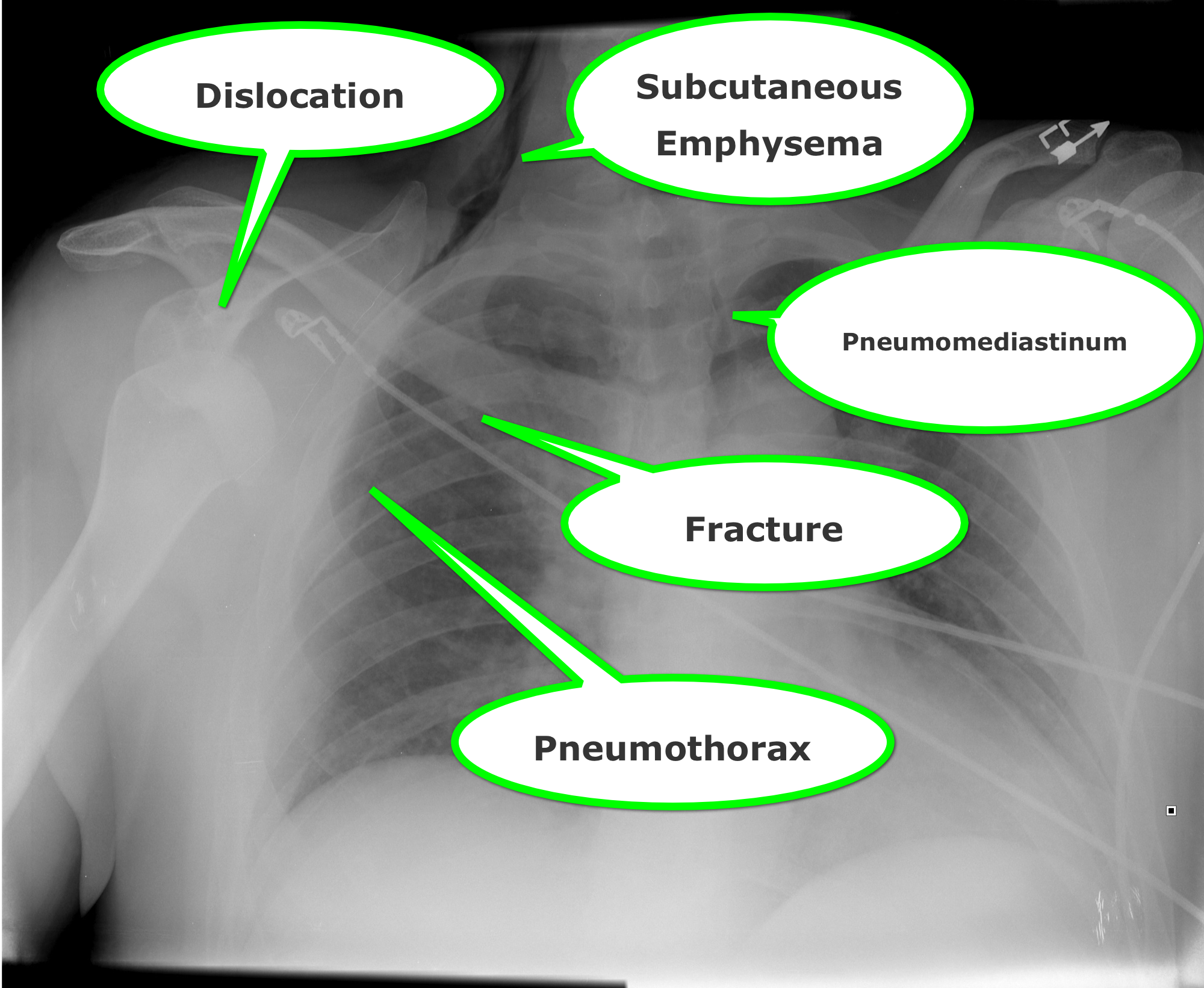
Humerus Fractures, Proximal
Wernicke encephalopathy (WE) is a neurologic disorder secondary to prolonged thiamine deficiency; it is characterized by confusion, ataxia, and ocular abnormalities.
Traditional medical teaching advises against the administration of glucose (or glucose containing fluid) in thiamine deficient patients, without first giving thiamine, as this may precipitate WE.
This teaching is problematic, however, in hypoglycemic patients who require the immediate administration of glucose while simultaneously being suspected of thiamine deficiency (e.g., malnourished alcoholics). Delays in treating hypoglycemia may be more harmful (e.g., seizures, permanent neurologic deficits, etc.) than the risk of WE.
Schabelman et. al performed a literature search to unearth the origins of this teaching. Nineteen papers related to this topic were found consisting of case reports, animal studies, and expert opinion; there were no randomized trials, cohort studies, or case-control studies.
Bottom-line: The available evidence does not support withholding glucose treatment until thiamine can be administered and educators should consider abolishing this dogmatic teaching until better evidence is available.
23 year-old female presents complaining of progressive right lower quadrant pain after doing "vigorous" pushups. CT abdomen/pelvis below. What’s the diagnosis? (Hint: it’s not appendicitis)

Atrial fibrillation is most commonly associated with cardiovascular disease
Non cardiac causes: pulmonary disease/PE, hyperthyroidism, sympathomimetics, drugs/ETOH
AFFIRM & RACE trials compared outcomes of a fib patients treated w/ rate vs. rhythm control
- No significant difference in survival between groups
Risk of thromboembolic CVA
- Rhythm control = Rate control + anticoagulation
New data challenges the need for strict heart rate control
- Resting heart rate should be <110 bpm
Use CHADS2 score to identify who requires anticoagulation based on %risk of emboli
- Chronic heart failure, HTN, Age>75, DM, Stroke/TIA
The median nerve is not the only compression neuropathy of the wrist
The ulnar nerve can become compressed at the level of the wrist as it 1) enters Guyon's canal or 2) or as the deep branch curves around the hook of the hamate
Compression can occur due to carpal bone fractures, local inflammation, ganglias, lipomas, anatomic abnormalities, etc
In sports medicine, the most common mechanism is injury is seen in cyclists (cyclist/handlebar palsy)
http://www.hughston.com/hha/b_15_3_2a.jpg
Also seen in those who participate in racquet sports, baseball, and golf
Symptoms can be isolated motor (claw hand = rare), sensory or both
http://en.academic.ru/pictures/enwiki/85/Ulnar_claw.jpg
Can be associated w/ median nerve compression
Tx: Activity modification such as wearing padded gloves, padding the object, or changing hand position on the handlebars
If above fails, surgical decompression is very effective.
Levamisole is a pharmaceutical with anthelminthic and immunomodulatory properties that was previously used in both animals and humans to treat inflammatory conditions and cancer.
It has been identified as a cocaine adulterant in the U.S. since 2003, with the DEA estimating that by 2009 up to 70% of cocaine seized contained levamisole.
Leukopenia, agranulocytosis, and vasculitis are well known complications of levamisole use.
One important complication to keep in mind is the possibility of multifocal inflammatory leukoencephalopathy (MIL). Although no formal case of leukoencephalopathy in the setting of cocaine use has yet been reported, various neurological side effects were described with levamisole therapy, the most concerning complication being MIL.
Anaphylaxis
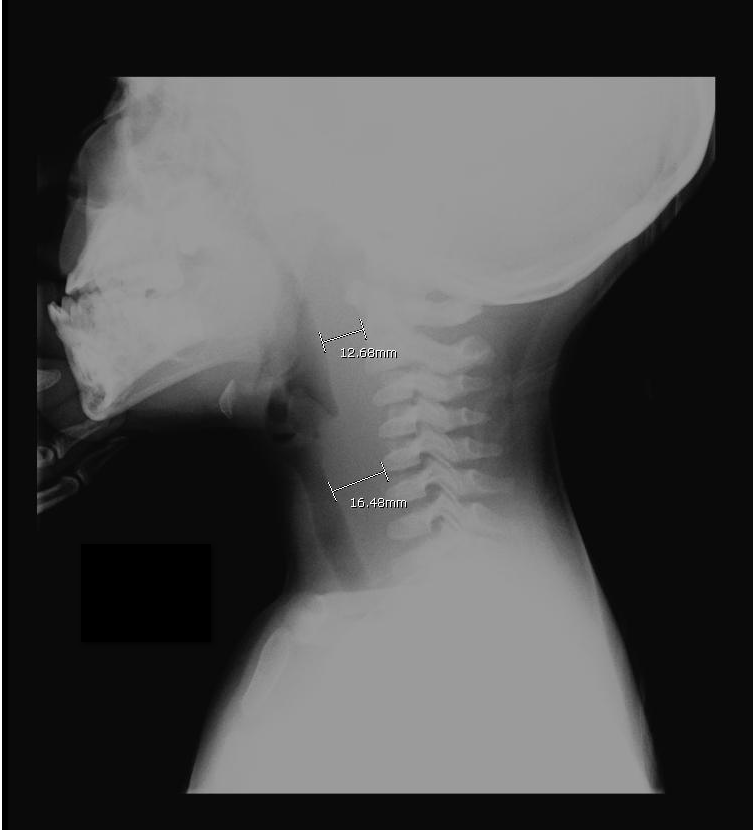
A previously healthy 3 year-old male presents with a one-day history of fever, drooling, and refusal to move his neck. The lateral neck x-ray is shown. What's the diagnosis?
Issue 1: Mean INR in study patients was only 1.22 (median 1.2). An INR of 1.2 represents very little actual anticoagulation.
Issue 2: In the small subgroup of patients with INR 1.5 to 1.7 (n = 269) there was a higher risk of ICH (7.8%), but did not reach statistical significance (it was significant in the unadjusted risk population).
Bottom line: Patients with INRs < 1.5 may be ok to receive tPA. Patients with INRs 1.5 or greater need further study.
No one treatment has demonstrated consistency of pain relief from jellyfish stings over all species; conversely, a treatment for one species may worsen an envenomation from another.
Deionized water, seawater, meat tenderizer, and urea treatment do not appear to produce any improvement in pain sensation.
Ammonia, acetic acid, and ethanol may cause an increased stinging sensation, and in most species vinegar may cause nematocyst discharge.
Application of topical lidocaine reduced the local sensation of pain (10% and 15% produced immediate pain relief), and hot water results in pain relief in the majority of patients tested.
Septic patients with hemodynamic instability often require intravenous fluids as part of their resuscitation. Major debate has occurred whether the optimal resuscitation fluids are crystalloids (e.g., normal saline) or colloids (e.g., albumin).
In theory, colloids are more potent intravascular expanders than crystalloids because their oncotic pressure is higher and should increase intravascular volume similarly to larger amounts crystalloid (i.e., colloids require less volume during resuscitation).
Despite these theoretical benefits, the colloid hydroxyethyl starch (HES), has come under scrutiny after prior studies have linked its use with adverse outcomes.
A recent prospective randomized-control trial compared the use of HES to lactated acetate for resuscitating septic patients and found that HES significantly increased both the incidence of renal-replacement therapy and mortality at 90 days (both primary end-points in the study).
Bottom line: There is no convincing data that HES performs superiorly to crystalloid for resuscitation in sepsis and there is increased harm with its use. Furthermore, the increased cost of HES compared to crystalloids does not justify its routine use.
Have you ever had to give a national presentation, but can't find that one ultrasound clip or image that you really need? You could "borrow" it from someone on the internet, but you are secretly afraid that the "owner" of the clip is lurking somewhere in the audience. Well, the guys at the Ultrasound Podcast (www.ultrasoundpodcast.com) have come to your rescue by creating SonoCloud, a free access ultrasound library. At Sonocloud, you will find several categories of ultrasound clips and images for you to view and share,...and again it's FREE. In fact, the only thing you are expected to do is upload some of your own ultrasounds to share.
[Pearls provided by Dr. Semhar Tewelde]
Cocaine...
1. causes systolic and diastolic dysfunction, arrhythmias, and atherosclerosis even in young users with relatively few cardiac risk factors, typically TIMI risk score <1
2. decreases myocardial contractility and ejection fraction by blocking sodium and potassium channels within the myocardium
3. prolongs the PR, QRS, and QT intervals on the ECG
4. users have a higher overall incidence of MI (odds ratio 3.8 to 6.9)
5. -induced chest pain is associated with acute MI in approx. 6% of cases
6. increases the risk of MI by 24-fold in the first hour after use
7. contributes to approx. 1 of every 4 MIs between 18 and 45 years of age
First Metacarpal Fractures:
There are two types of fractures that commonly occur at the base of the 1st metacarpal. They are:
Bennett Fracture: This is an intraarticular fracture at the base of the 1st metacarpal that always involves some degree of subluxation or dislocation of the 1st carpometacarpal joint.

Image from Wikipedia Commons
Rolando Fracture: This is a communited intraarticular fracture at the base of the first metacarpal that typically has a T or Y shaped configuration with 3 fragments.

Image courtesy of WikiPedia Commons