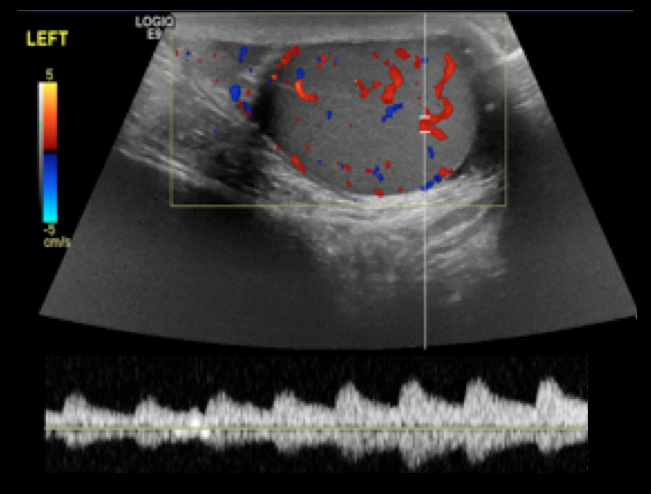
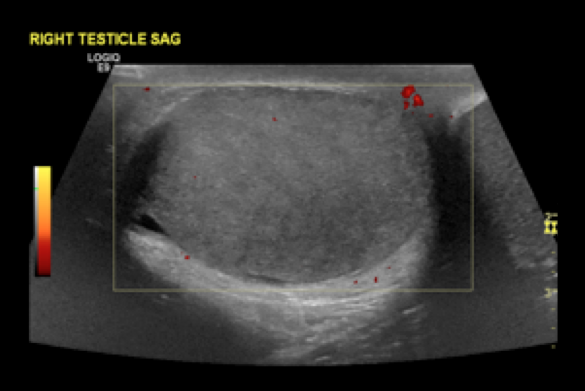
14 year-old male presents with right-sided testicular pain. What's the diagnosis?
A recent study in JAMA has provided further evidence regarding some key issues in ACS/MI presentations which seem to be commonly taught but often forgotten in actual practice. Here's just a few of the key findings from this study:
1. Generally speaking, women were more likely to present without chest pain than men, and the difference between the sexes was most apparent in the < 45yo groups. Overall, 42% of women presented with painless MIs. [remember from a recent prior cardiology pearl that painless MIs have a higher mortality as well]
2. Women had a higher mortality than men within the same age groups, and the difference between the sexes was most apparent in younger ages.
3. Almost 1/5 of women < 45 yo with MI did not report chest pain. [We've always assumed it's just the older women that present with painless MIs....not true!]
A final point that should be re-stated: young women DO have MIs, they DO often present without pain, and they DO often die. Be wary.
The plantar fascia arises from the medial tuberosity of the calcaneous and extends to the proximal phalanges of the toes.
Pkantar Fasciitis is the most common cause of heel pain in adults.
Etiology is thought to be from a degenerative tear at the fascial origin followed by a tendinosis type reaction and .
Affects women 2x> men
More common in overweight patients.
Onset is insidious and not related to trauma.
Hx: Pain and tenderness directly over the medial calcaneal tuberosity and 1-2cm distally along the plantar fascia.
Pain is worse with prolonged standing/walking. Pain is most intense however when rising from a resting position such as first thing in the morning.
PE: Pain is increased with passive dorsiflexion of the toes. Tenderness to palaption over the medial calcaneal tuberosity and 1-2cm distally along the plantar fascia.(At times, one may have to apply increased pressure to approximate weight bearing type stress)
XR: Usually not necessary with a good history and exam. Heel spurs are seen in up to 50% with the disease (and in up to 20% without it!)
DDx: Tarsal tunnel syndrome. Calcaneal stress fracture. Fat pad atrophy. traumatic rupture of planter fascia.
Pressure immobilization involves wrapping the entire extremity with a bandage and then immobilizing the extremity with a splint. It is a technique routinely employed in the pre-hospital management of neurotoxic snakes in Australia.
A position statement was recently published by several international toxicology societies regarding the utility of pressure immobilization after North American Crotalinae snake envenomation (e.g., Copperheads, Timber rattlesnakes, Cottonmouths).
"Available evidence fails to establish the efficacy of pressure immobilization in humans, but indicates the possibility of serious adverse events arising from its use. The use of pressure immobilization for the pre-hospital treatment of North American Crotalinae envenomation is NOT recommended."
Preventing VAP in the Intubated ED Patient
The seasonal influenza vaccine is produced in chicken eggs. Ovalbumin, an egg protein, is often listed as a component of the purified vaccine on most drug-package inserts. The concentration of ovalbumin indicates the potential egg-allergen content of a vaccine.
Earlier ACIP guidelines recommended against giving the influenza vaccine to people with egg allergy, including those with a history of mild symptoms. However, several studies showed that influenza vaccine containing inactivated, or killed, virus is safe to give to people with egg allergy, especially those with a history of mild allergic reactions.
Influenza vaccines are now made with much lower ovalbumin concentrations than in the past; therefore, the level of potential egg protein allergens in a single dose of vaccine is extremely low.
The following are ACIP recommendations for the 2011 to 2012 influenza season:
Ventricular assist devices (VAD) pump blood from the left, right or both ventricles for patients in severe ventricular failure.
VADs may be placed temporarily (as a bridge to transplant) or permanently in patients who are not transplant candidates (also known as Destination Therapy)
Certain types of VADs continuously pump blood in a non-pulsatile fashion. In these cases, a patient may be perfusing normally without a palpable pulse.
Familiarity with potential VAD complications is important as a patient with a VAD may be presenting to an ED near you. Complications include:
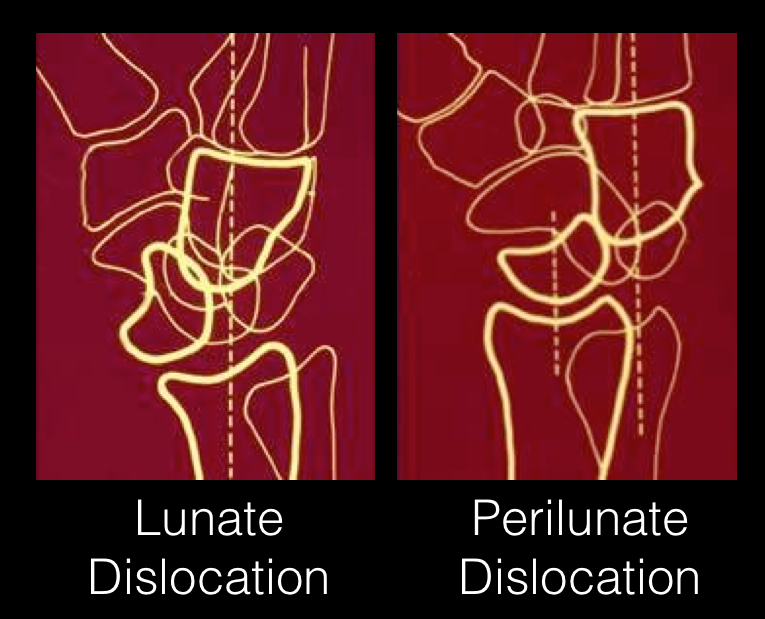
24 year-old male presents following fall from a scaffolding and complains of wrist pain. Diagnosis?

Quick pearls on cardiogenic shock
Post-MI cardiogenic shock is associated with a mortality of 50-70%. There are only a few interventions that have been demonstrated to improve outcomes: early use of intra-aortic balloon pump, stenting, and G2B3A inhibitors.
It is generally recommended to avoid clopidogrel since so many of these patients will require CABG.
Early use of mechanical ventilation decreases work of breathing and improves oxygenation.
Remember that age alone is not a contraindication to aggressive treatment.
Severs disease
- Perhaps the most common overuse injury
-Pain is due to inflammation of the calcaneal apophysis growth plate
- Caused by repetitive microtrauma from the pull of the Achilles tendon on the apophysis.
- Occurs in young athletes ages 7-14
Sx’s bilateral in >50%
Hx – Gradual onset of posterior heel pain, worse with activity, better with rest.
PE – Tenderness at the insertion of the Achilles tendon onto the calcaneous. Swelling is mild.
This is a self limited condition because as the adolescent ages, the physis closes
Tx – Rest (no running or jumping), ice, NSAIDs, heel lifts/arch supports. Outpatient physical therapy for stretching and strengthening exercises.
You have seen the study comparing diazepam to lorazepam IV for the cessation of seizures. Lorazepam one that one. Now, for prehospital status epilepticus midazolam IM went head to head with IV lorazepam to see which would stop seizure more quickly.
This study was more about the practicality of starting an IV than it was of the pharmacokinetics or onset of action of a particular benzodiazepine. It was a large enough study to warrant publication in New Engl J Med last month and is worth noting.
Subjects whose seizures ceased before ED arrival (median):
Time to active treatment: 1.2 min IM Midazolam group; 4.8 min IV Lorazepam group
Median times active treatment to cessation of SZ: 3.3 min IM Midazolam and 1.6 min IV Lorazepam
Safety was equal in both groups. This study validates EMS initiating therapy with IM midazolam for the cessation of seizures while intravenous access is being attempted.
Ice-Cold Crystalloid for Therapeutic Hypothermia
Getting tired of the same old Power Point presentations? Getting bored with Apple's Keynote? Looking for something new to excite learners?
Well, you might want to consider using a newer presentation tool, a tool designed to eliminate those boring bullet points...
Say hello to Prezi...
This really cool presentation tool allows you place all of your content (words, pictures, video, etc) on one canvas and then manipulate the sequence you want to show it in.
Check out the website and give it a try: www.prezi.com
Simply click on some of the sample Prezi presentations on the site. It's very cool and quite addictive.
Morton's Neuroma
Children & Appendicitis
A fluid bolus is often the first-line therapy for patients with pericardial tamponade. A fluid bolus, however, may not always improve hemodynamics.
The cardiac index of forty-nine patients with cardiac tamponade was assessed before and after a 500 cc normal saline bolus:
Bottom-line: A fluid bolus may a reasonable first choice in a hypotensive patient with tamponade, but remember that fluid boluses may not always work. Attempts at fluid resuscitation should never delay definitive treatment with pericardiocentesis.
35 year old male with sudden onset of abdominal pain. Diagnosis?