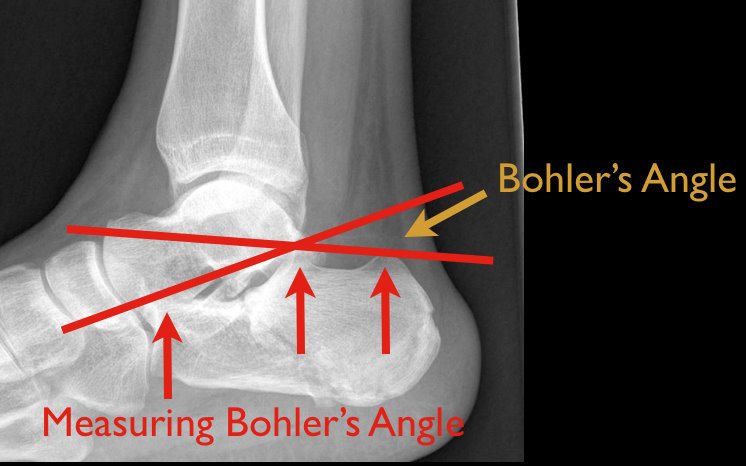
48 year old male following 15 foot fall onto both feet. What is the diagnosis?
…and why is it called the “Lover’s Fracture”?

There has been some controversy regarding the actual clinical benefit of non-invasive ventilation (NIV) for patients with cardiogenic pulmonary edema in recent years. However a recent Cochrane review has confirmed the benefit of NIV for these patients. Early (ED) use of NIV is associated with a decrease in both intubation rates and mortality. The NNT to prevent one intubation is 8, and the NNT to prevent one hospital mortality is 13. To put this in perspective, the NNT for NIV to prevent death in patients with cardiogenic pulmonary edema is lower than the NNT for thrombolytics to prevent death in acute MI.
One key point to remember is that it MUST be used early! If you wait until your patient is decompensating, it is often too late. Start the NIV as soon as possible in these patients.
Emergency physicians are often called upon to provide event coverage for marathons.
Prolonged endurance racing is safe for the majority of participants.
Hyponatremia (8.2% - 13.5%) - finishing times of greater than 4 hours is an independent risk factor
Hypokalemia – uncommon
Renal function – BUN > 30 or Cr > 1.4 mg/dL (23.6%). There is no data that this is of any clinical significance.
Cardiac Troponin - (11%) had significant increases (troponin T > or = 0.075 ng/mL or troponin I > or = 0.5 ng/mL). Elevations were more commonly seen with weight loss and increased Cr levels and may be associated with running inexperience (< 5 previous marathons) and young age (< 30 years) though interestingly not with race duration or traditional cardiac risk factors.
Findings are similar for men and women
Animal studies show high doses of caffeine produces catecholamine triggered activity
Small studies in high risk patients (recent MI, malignant arrhythmias) have shown no increase in frequency or severity of arrhythmia
No large scale human studies exist evaluating caffeine's effects on patients with malignant arrhythmias (VF/VT)
Overall, the data suggest that caffeine is well tolerated in moderate doses in most patients, even those with known or suspected arrhythmias
In patients who claim sensitivity to caffeine, or in those with known arrhythmias where catecholamines are felt to drive the arrhythmia, caffeine may be discouraged by physicians.
Amiodarone is a class III anti-arrhythmic for tachyarrhythmias
Although most patients remain euthyroid on amiodarone, 4-18% develop thyroid disease months to years after exposure.
Amiodarone-induced thyroid disease occurs because amiodarone is structurally similar to triiodothyronine and thyroxine and each 200mg tablet contains 75 mg of iodine.
Two types of amiodarone-induced thyroid disease:
Amiodarone-induced hypothyroidism (AIH)
Amiodarone-induced thyrotoxicosis (AIT)
DDx for JVD + hypotension + clear lungs:
RV infarction
massive PE
tension PTX (clear lung)
pericardial tamponade
Assuming your physical exam diagnoses tension PTX, you only need two simple tests to make the diagnosis amongst the other possibilities:
1. EKG: RV infarction will almost always show a concurrent inferior MI;
2. bedside U/S: tamponade patients have effusion, PE patients have RV distension
Patients requiring anticoagulation for HIT or with a history of HIT may be initiated on argatroban. We have recently been seeing increased utilization. Here are some important points to remember.
The mounting evidence on the use of 20% lipid emulsion or intrlipid has been growing for any patient that is hemodynamically unstable due to a drug exposure. There is now a recent case report of a verapamil overdose patient that received intralipid and did well. They were able to measure verapamil levels before and after administration. They were able to remove the lipid from the serum to appropriately measure the level and found effective removal. This adds to the theory of the "lipid sink" where the lipid actually is binding/surrounding a lipophilic molecule effectively removing it from interaction.
Hepato-Renal Syndrome
49 y.o. female on Trimethoprim/sulfamethoxazole presents with rash and oral mucus membrane lesions. Diagnosis?

Paroxysmal supraventricular tachycardia (PSVT) is a common tachydysrhythmia encountered in ED practice. PSVT in itself has not been found to be an isolated manifestation of myocardial infarction or unstable angina (i.e. "isolated" = in the absence of other concerning symptoms, such as anginal-type pain, etc.). Nevertheless, some physicians will routinely test cardiac troponin levels to evaluate for ACS in these patients. We should all remember, though, that tachydysrhythmias including PSVT are a potential cause of elevated troponin levels in the absence of coronary disease, and these elevations do NOT correlate with adverse outcomes unless other concerning symptoms/signs are present as well.
A recent study1 corroborated this point: 11 out of 38 patients with PSVT had a positive troponin level. Only 2 of the 11 ruled in for ACS, and all of the patients were well at 30 days. Both patients presented with hypotension (SBP in the 70s) and also had other concerning symptoms, such as chest pain (both), dizziness (both), and dyspnea (one).
The takeaway point is simple: if you routinely send troponin levels on your patients for PSVT in the absence of other concerning symptoms/signs, you'll find yourself chasing a lot of false-positive levels.
Pes Anserine Bursitis is an inflammatory condition of the medial knee
Occurs at the bursa of the pes anserinus which overlies the attachment of the 1) Sartorius 2) gracilis and 3) semitendinosis tendons
Note the location is 2-3 inches below the knee joint on the medial side
http://kneespecialistsurgeon.com/images/uploaded/Pes%20anserinus%20bursitis%20image.jpg
http://eso-cdn.bestpractice.bmj.com/best-practice/images/bp/en-gb/575-27_default.jpg
Patients complain of pain (especially with stair climbing)
PE: Tenderness to palpation of the bursa with mild swelling
DDx: MCL tear, medial meniscus injury, medial (knee) compartment arthritis
Treatment: Cessation/modification of offending activities, Icing and ice massage, NSAIDs, hamstring stretching and physical therapy. Failure of the above should prompt referral for bursal steroid injection.
Cancer patients admitted to ICUs with AKI or who develop AKI during their ICU stay have increased risk of morbidity and mortality. AKI in cancer patients is typically multi-factorial:
Causes indirectly related to malignancy
Septic, cardiogenic, or hypovolemic shock (most common)
Nephrotoxins:
Aminoglycosides
Contrast-induced nephropathy
Chemotherapy
Hemolytic-Uremic Syndrome
Causes directly related to malignancy
Tumor-lysis syndrome
Disseminated Intravascular Coagulation
Obstruction of urinary tract by malignancy
Multiple Myeloma of the kidney
Hypercalcemia
Because AKI increases the already elevated morbidity and mortality in these patients, prevention (e.g., using low-osmolar IV contrast, avoiding nephrotoxins), early identification (e.g., strict attention to urine output and renal function), and aggressive treatment (e.g., early initiation of renal replacement therapy) is essential.
There are several complications of acute aortic dissection that emergency physicians must be familiar with.
These include:
*Key Pearl: If a patient with suspected or confirmed acute aortic dissection suddenly arrests consider cardiac tamponade.