Transient brachial plexopathies aka Burners and Stingers
Brachial plexus injuries are the most common peripheral nerve injuries seen in athletes.
49-65% of all college football players have experienced at least one burner with a 87% recurrence rate.
Injuries most commonly occur at C5-C6 but may involve any root level.
3 Mechanisms: Commonly due to
1) Traction caused by lateral flexion of the neck away from the involved side
2) Compression of the upper plexus between shoulder pads and scapula
3) Nerve compression caused by neck hyperextension and ipsilateral rotation.
CC: Burning or numbness in the neck, shoulder and/or arm
Symptoms are UNILATERAL and tend to usually last seconds to minutes
Symptoms are reproduced by the Spurling maneuver.
Function gradually returns from the proximal muscle groups to the distal muscle groups.
Because most burners are self-limited, the most important goal is to rule out an unstable cervical injury.
TIP: Suspect when abdominal pain presents 10-14 after chemotherapy (when PMNs are lowest).

Iliopsoas tendonitis and Iliopsoas Syndrome
The following list of medications have been associated with the development of Lupus Anticoagulants. Though it sounds like they should anticoagulate, they interfere with the Protein C system which means that they could induce a pro-thrombotic state - good short list to know:
Chlorpromazine (Thorazine
Procainamide (sorry Amal, I know you love that drug)
Hydralazine
Quinidine
Phenytoin
(1) do not have increased risk for clinically significant ICH,
(2) have early clinical improvement similar to younger patients, and
(3) have poor outcomes related to increased mortality (odds ratio 30% versus 12%), rather than
to higher rates of functional dependence (i.e. Modified Rankin Score 3 to 5).
Acute Liver Failure (ALF)
Ever see that patient who shows up in the ED with blue painful toes? You look at the foot (or feet) and quickly determine that clot has embolized into the foot.
What is the differential diagnosis to consider in patients with evidence of embolic phenomenon in the feet (i.e. blue, painful toes)?
Things to consider:
Clearly we can't do the complete workup of embolic foot lesions, and many if not most of these patients will need to be admitted to complete their workup.

It is now well-accepted that induction of hypothermia should be initiated in victims of cardiac arrest who regain spontaneous circulation and remain unresponsive. Studies are now being performed and published that suggest that the earlier that hypothermia is induced, the better the neurological outcome. With this in mind, some experts are now recommending that cool IVF be the initial resuscitation fluid that these patients receive when resuscitation is initiated. It appears that aggressive use of cool IVF right from the initiation of attempted resuscitation results in improvements in survival to hospital admission and discharge.
The bottom line here is that when caring for victims of primary cardiac arrest, we should be certain to cool the patients fast and early!
Meralgia Paresthetica - caused by entrapment of the lateral femoral cutaneous nerve (LFCN)
The LFCN is responsible for sensation of the anteriorlateral thigh.
http://www.chiropractic-help.com/images/Meralgia-Paresthetica.jpg
NOTE* It has no motor component!
Associated with pregnancy, wearing tight pants, belts, girdles, and in diabetic and obese patients.
Symptoms include numbness, paresthesias and pain (not weakness). Worse w walking, standing. Better w sitting.
Diagnosis is clinical but may be confirmed with nerve conduction studies
Treatment includes, NSAIDs, injection and surgery for refractory cases.
"Ear to sternal notch" positioning has gained wide acceptance in the emergency medicine and anesthesia literature. Most often, this teaching is brought up with respect to obese adult patients whose large body habitus requires the raising of the neck and head to achieve airway alignment.
However, the correct anatomic positioning principle applies to all ages. Specifically, with regard to neonates, a shoulder roll is often placed indiscriminately to put the patient into the now out-dated "sniffing position," usually worsening the view of the airway.
Though this positioning is frequently misused, it can be easily adapted to apply ear to sternal notch positioning to neonates, whose misaligned airway is the result of a large occiput rather than a large torso. In all ages, if you follow these positioning principles, you will improve your view of the airway:
1. Align the ear to the sternal notch
2. Keep the face parallel to the ceiling (do NOT hyperextend the neck, as in the sniffing position)
3. In adults, the head usually needs to be raised (Image 1), while in infants, the torso usually needs to be raised (image 3).


Several patients have recently presented with a medication history including tapentadol (Nucynta), the newest opioid formulation. It is approved for treatment of acute moderate-severe pain. Here are some key points:
Causes of Pulsatile Tinniitus
Although oral metronidazole is indicated for mild to moderate Clostridium difficile associated diarrhea, oral vancomycin should be considered first-line therapy in critically-ill patients with moderate to severe disease. Vancomycin dosing should begin at 125mg PO q6 and increased to 250mg q6 if poor enteral absorption exists. Consider adding metronidazole IV if either reduced enteral absorption or severe disease exists.
Recently, fidaxomicin has been shown to be non-inferior to oral vancomycin in the treatment of mild to moderate C. difficile. While promising, the study population was not critically-ill and extrapolation should be avoided.
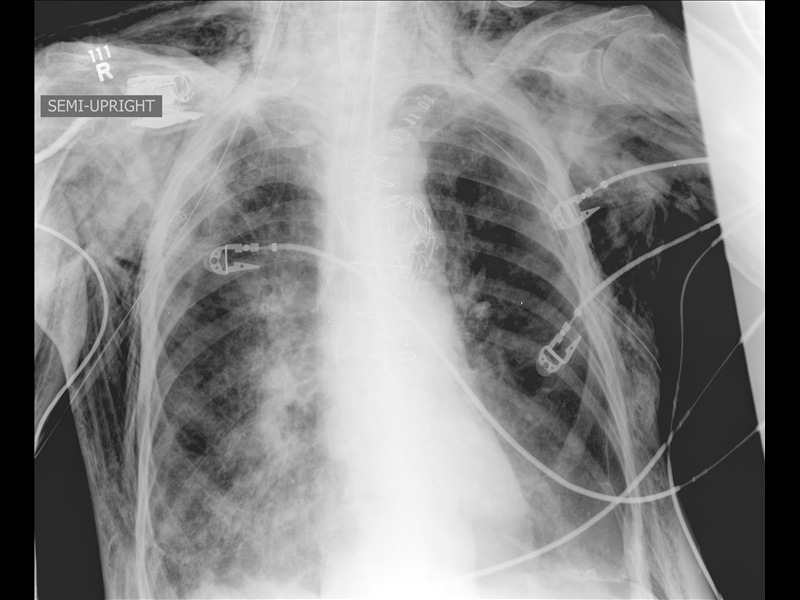
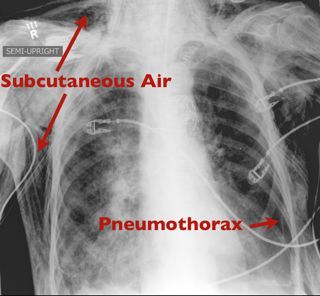
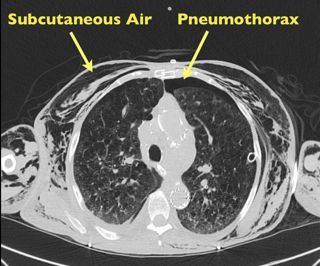
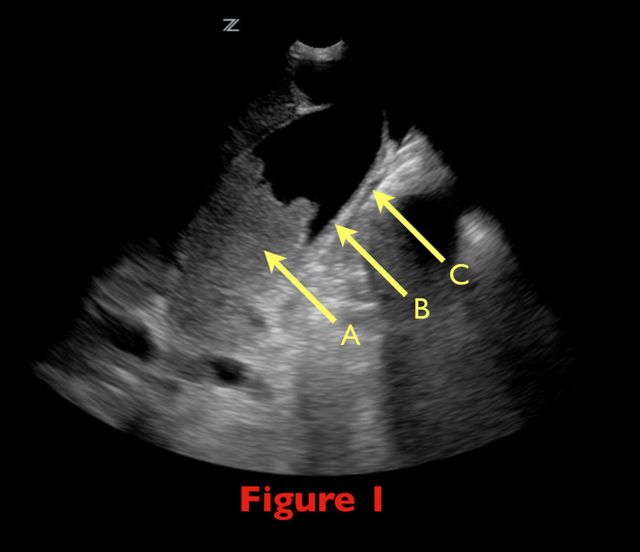
70 yo female from nursing home with fever. RUQ ultrasound is shown below. Diagnosis?

Beck's triad is well known to many physicians, but here's some simple things you may not have known.
Beck actually described two triads, one for acute and one for chronic tamponade.
The triad for chronic tamponade consists of increased CVP (JVD), ascites, and a small quiet heart (muffled heart sounds).
The triad for acute tamponade consists of JVD hypotension, and muffled heart sounds.
Almost 90% of patients have at least 1 of the signs, but only one-third have all 3. Furthermore, it appears that the simultaneous occurrence of all 3 signs is a very late manifestation of tamponade, usually preceding cardiac arrest.
Tendon Lacerations:
A reasonable approach to all tendon lacerations is to close the wound and splint in the hand in the position of function until the patient can be seen by a hand surgeon in the next 1-3 days. These injuries do not require immediate surgical repair.
Continuing the theme of endotracheal tube size pearls... You get a box call for a pre-term baby delivered precipitously by mom at home and baby is blue. EMS is bagging but unable to secure a definitive airway. What size ETT do you reach for? If you try to apply the formula "uncuffed ETT = (age/4) + 4", how much smaller than size 4 can you go?
IV acetaminophen has been approved for use since November 2010
It is indicated for the:
The results of studies demonstrating opoid sparing effects have been mixed; some studies have not demonstrated either a reduction in opioid dose or opioid side effects.
The dose is the same for acetaminophen administered by other routes.
It must be administered over 15 minutes, and onset of activity is 15 minutes. Peak effect occurs at one hour.
The MAJOR drawback is the cost, which is $13 dollars per vial. This is compared to oral acetaminophen and ibuprofen, which are pennies.