This single center prospective study asked residents to determine if their patient had barriers to post ED discharge health care such as having a PCP, transportation issues, affording medications, and need for assistance with activities of daily living. They then compared the physicians’ answers to patient’s answers and found: “Physicians had poor sensitivity for accurate identification of patient barriers.”
Some of our discharged patients are struggling more than we realize.
This was a retrospective study of the pediatric cardiac arrests over a 5 year period (including COVID years) in Vienna.
Infants (<1 year) had the highest incidence of OHCA among all pediatric age groups, consistent with German registry data showing an incidence of 23.4 per 100,000 in this age group.
Non-shockable rhythms (asystole/PEA) predominated, as expected given that most pediatric OHCA results from progressive respiratory failure or shock rather than primary cardiac causes.
Survival to hospital discharge remained low, consistent with international data showing pediatric OHCA survival ranging from 6.6% for infants to 17.3% for adolescents in the US CARES registry.
Bystander CPR rates and witnessed arrest status were important modifiable factors associated with improved outcomes, aligning with findings from the adult Vienna cohort where witnessed arrests with shockable rhythms had substantially higher survival (39% vs. 9.3% overall).
The study highlighted that even in a high-resource, physician-staffed EMS system, pediatric OHCA outcomes remain poor, underscoring the importance of primary prevention and early bystander intervention
There were a handful of big name critical care studies published the last few weeks (LOGICAL, ARISE FLUIDS, SODa-BIC to name a few) but many of you probably already saw those so we're gonna stick with something a little more off the beaten path.
A retrospective observation trial was published recently by Gastanadui et al in Journal of Intensive Care looking at the mortality impact of corticosteroids in cardiogenic shock. They looked at 167,721 patients from the Vizient database admitted with cardiogenic shock (excluded patients with other indications for steroids). The unadjusted mortality was a whopping 48.8% in the steroid group and 29.6% in the non-steroid group. They did Inverse Probability Treatment Weighting (IPTW), which attempts (imperfectly, but best as you can retrospectively) to control for treatment selection bias, and still found a roughly 3% mortality increase in the steroid group.
Bottom Line: Corticosteroids were already controversial (at best) in cardiogenic shock, but this further adds to the reasons to avoid them in this condition. Of note, this trial excluded patients with classic hard-indications (e.g. adrenal insufficiency, COPD exacerbation, etc) and steroids should still be given to those groups, but in my opinion if you feel cardiogenic is the primary driver of the patient's shock and they do not have another indication, I would consider avoiding steroids solely for the shock.
This multicenter study looked at trauma patients with a hemothorax who underwent early tube thoracostomy vs. being observed. They found volume of over 300 ml predicted observation failure. Those observed had shorter hospital stays and less ICU admissions. Twenty two percent of observation patients required tube thoracostomy. The failed observation group had similar outcomes except longer hospital stays.
Bottom Line: Lactate is a useful but imperfect marker of critical illness. Below are some key points to consider when interpreting lactate.
Bottom Line: In pediatric patients, identifying the underlying etiology of hypercalcemia is essential to guide appropriate long-term management.
Etiology: The causes of hypercalcemia in children are diverse and are broadly classified into parathyroid hormone (PTH)-mediated and non–PTH-mediated categories. Non–PTH-mediated causes include endocrine disorders, inborn errors of metabolism, medication-induced hypercalcemia, granulomatous diseases, immobilization, and malignancy.
Clinical Presentation: Symptoms vary depending on the severity of hypercalcemia. Mild hypercalcemia may be asymptomatic or present with findings such as shortened QT interval, polyuria, and constipation. Severe hypercalcemia can lead to significant complications, including seizures, altered mental status (e.g., hallucinations), dehydration, cardiac dysrhythmias, abdominal pain, and pancreatitis.
Management: In the emergency setting, the primary treatment is intravenous hydration, typically with 0.9% saline, to cause calcium dilution and increased urinary excretion of calcium. Loop diuretics should be used with caution in pediatric patients due to the risk of exacerbating dehydration. Additional pharmacologic therapies, including calcitonin, bisphosphonates, and glucocorticoids, may be indicated depending on the etiology and severity, and should be administered in consultation with a nephrologist and/or endocrinologist. In patients with contraindications to aggressive fluid management (e.g., renal or cardiac dysfunction), or in cases of severe, life-threatening hypercalcemia, dialysis may be required.
When managing suspected or proven Group A Streptococcus (GAS) Necrotizing Soft Tissue Infections (NSTIs), standard beta-lactams can lose efficacy due to the Eagle effect—where stationary-growth phase bacteria become less susceptible to cell-wall acting agents.
To counteract this and aggressively suppress life-threatening bacterial toxin production, always add a protein-synthesis inhibiting antibiotic to your empirical broad-spectrum base.
Expert consensus recommends not prescribing these eight classes of medications to older adults mostly due to sedative affect and fall risk. 1. Benzodiazepines 2. Barbiturates 3. Muscle relaxants 4. 1st generation antihistamines 5. Sulfanylureas 6. 1st generation antipsychotics 7. Zolpidem 8. Metocloprimide
A recent study shows marginal improvement in not prescribing these medications to older ED patients.
This single center study looked at diabetic patients who had a POC glucose over 300 and POC ketone over 1.1 and reviewed their diagnosis vs the laboratory accepted diagnosis of DKA.
“The most recent international consensus laboratory definition of (non-euglycemic) DKA includes a glucose of >?250; a pH <?7.3 or a bicarbonate ??18?mmol/L; and a beta-hydroxybutyrate (BOHB) ??3.0?mmol/L or urine ketone strip ??2+”
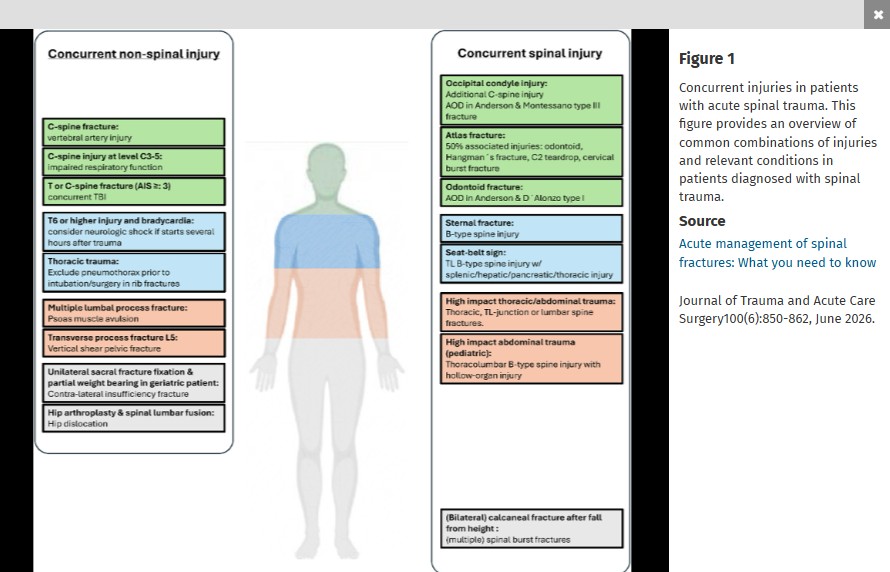
This nice review article reminds us “The AO-Spine classification is the most frequently utilized system for thoracic and lumbar fractures, and it categorizes fractures into three types. Type A fractures are compression injuries. In these fractures, the assessment of the involvement of the posterior elements of the vertebral body is essential. Type B fractures are distraction injuries implying tension band involvement, whereas type C fractures are translational or dislocated injuries. The AO-Spine Upper Cervical Injury Classification System… In this classification system, type A injuries have no ligamentous involvement and are considered stable. Type B injuries have tension band or ligamentous injury and may be unstable. Type C injuries are characterized by significant translation and loss of anatomic integrity and are considered unstable."
A 22 year old normally healthy male presents with tachycardia (HR 140), dilated pupils (7 mm), dry flushed hot skin, and confusion/agitation. His mother states he has a 1 day history of “talking out of his head not making sense”, “seeing things that aren’t there”, and “speaking to video game characters”. He has suprapubic tenderness with markedly distended bladder on exam revealing over 1 liter of urine on bladder scan. She found a small bottle containing a large amount of small 2-3 mm black seeds in his room and suspects he ingested them. What treatment options would you consider?

Do you have a patient with shortness of breath and pulmonary edema?
Don’t forget to place the color doppler over the mitral valve to look for acute mitral regurgitation.
These authors argue that bystander interventions in the early minutes (they call them the diamond minutes) can have an impact on trauma survival. Particular attention to External hemorrhage control; Airway opening and maintenance; Safe positioning of unconscious patients; Mitigation of early hypoxia and hypothermia could improve survival. We need to publicize this information and undo the years of teaching not to move these patients due to concern of secondary spinal cord injury. Many studies have dispelled that concern.

This article suggest that freeze-dried plasma (FDP) is an acceptable adjunct to whole blood for prehospital resuscitation of trauma patients. “FDP is pathogen-reduced, shelf-stable for up to two years at room temperature, lightweight, and rapidly reconstituted at the point of care.” This method offers an advantage when caring for patients in remote areas with long transport times and has been used by NATO and Canadian armed forces.
Of the 215 Norwegian patients on oral anticoagulation seen for a head injury and having a normal initial head CT, none developed delayed hemorrhage. Median age was 83 years.
A recently published commentary highlights the importance of looking beyond the numbers and remembering the core mission of emergency practice. It warns against “gaming” the system to create processes that give better metrics using the example of rates of patients who leave without being seen (LWBS). In the author’s words, efforts aimed at improving this metric create strategies that “raise concerns about distributive justice, beneficence, and professional integrity.” See link for key take home points.
Sodium bicarbonate significantly reduced the need of renal replacement therapy (risk ratio [RR] 0.69; 95% CI, 0.61–0.78) but not mortality (RR, 0.84; 95% CI, 0.55–1.30). However, there was not enough sample size to support the outcome of mortality.
There was still significant heterogeneity between studies as the sources of metabolic acidosis were different between different studies in this meta-analysis study of randomized control trial. One study recruited patients with septic shock only, while other studies enrolled patients with different disease states.
There was also heterogeneity in the threshold for pH to enter the study.
Bottom Line: In adults presenting to the ED with bacteremia, bandemia may be associated with increased short-term mortality, with higher band percentages correlating with greater risk. Although bacteremia is rarely diagnosed during the ED visit because blood cultures require time to result, the presence of bandemia should raise concern for possible occult critical illness.
{kind=link}