In adult patients, ultrasound-guided long catheter IVs for difficult venous access have been shown to provide increased duration of use, reduced complication rates, and greater cost-effectiveness.
However, there are relatively few studies examining the use of ultrasound for IV access in pediatric patients.
A recent study, the DIAPEDUS study, investigated the success rate of peripheral IV access with and without ultrasound assistance in pediatric patients with difficult venous access.
The study included 110 pediatric patients. IVs were placed by 25 nurses and 6 pediatricians, each of whom had completed departmental training involving at least 20 ultrasound-guided IV placements prior to the study.
The results showed a significantly higher success rate on the first attempt with ultrasound-guided techniques (90% vs. 18%), along with reduced procedural time and fewer attempts overall.
Bottom Line: For patients with known difficult venous access, ultrasound-guided IV placement should be the first-line approach.
In this randomized trial of restrictive oxygen (arterial oxygen sat of 94% ) vs. liberal oxygen (12-15 L of O2 per minute) for 8 hours after traumatic injury there was no difference in mortality or major respiratory complications at 30 days between the two groups.
Further evidence that managing hypoxia is important but over oxygenation at best offers no benefit and may add harm.
Cardiovascular disease (CVD) is the leading cause of death both in the United States and globally for both men and women.
Major adverse cardiovascular events (MACE) is a commonly used composite outcome.
MACE is defined as non-fatal stroke/acute myocardial infarction/heart failure or cardiovascular death.
Physical inactivity is a leading risk factor for noncommunicable diseases and death worldwide
Up to 5 million deaths/yr could be averted with increased physical activity
Regular physical activity reduces the risk of many types of cancer by 8-28%, diabetes by 17%, heart disease and CVA by 19%, and dementia by 20%.
Many adults and children find meeting the recommended physical activity goals very challenging.
A recent observational study found that just 1.5-to-4-minute small bursts of high intensity exercise throughout the day may help lower an individual’s risk of MACE.
To clarify, this does not mean going to the gym to do a 45-minute HIIT class
Vigorous intermittent lifestyle physical activity (VILPA) involves such simple things as carrying the groceries a short distance or taking the work stairs instead of the elevator.
Such activities are more feasible for all of us vs structured exercise for obvious reasons.
Study group was >100,000 middle-aged men and women. Average age 61.
All participants wore an activity tracker continuously for a full week.
This data was used to calculate VILPA bouts throughout the day.
Female participants with no formal exercise regimen who recorded just 3.4 minutes of VILPA a day were 50% less likely to have a MI, had a 67% decreased risk for heart failure and 45% less likely to develop any type of MACE vs those who did not clock any VILPA during their day.
Female participants who recorded just 1.2-1.6 minutes of VILPA a day had a 33% lower risk of MI, 40% decreased risk of heart failure and 30% lower risk of MACE.
In male participants, those with 5.6 minutes of VILPA each day had a 16% reduced risk of having MACE than those who did not have any VILPA.
Differences may be due to women’s VILPA intensity was roughly 20% greater than men
Conclusion: Take the stairs
Infantile Spasms (now known as Infantile Epileptic Spasms Syndrome- IESS) is a subtle, can't miss diagnosis occurring in children under the age of 2, with 90% presenting before 1 year of age.
History:
Presentation for these patients can be sporadic, recurrent, flexion or extension of the limbs or head. The patient typically remains alert during an episode, but they can be startled or appear uncomfortable from the sudden movement.
With smart phone use, parents often have videos of the events that a provider can see as they are often no events in the ED.
Prognosis is very poor with up to 50% having long-term neuro-cognitive complications or regression.
Examination:
A complete physical exam should be performed with particular attention to focal neurologic deficits which would require emergent imaging, signs of electrolyte abnormalities (eg. Chvostek's sign in hypocalcemia), and evidence of neurocutenous syndromes (eg. Neurofibromatosis, tuberous sclerosis).
Testing:
Diagnosis is made with EEG showing hypsarrhythmia. This should be done as soon as possible, most often requiring an inpatient admission.
Lab work can be done to exclude other possible causes of abnormal movements including assessing for electrolyte abnormalities.
Imaging in the ED is not typically indicated unless there is concern based on exam. MRI is the imaging modality of choice, and is often completed after EEG confirmed diagnosis.
Treatment:
Management is initiated in conjunction with a pediatric neurologist with most common therapies being corticotropin (ACTH) and vigabatrin.
A recent review article highlighted the adverse effects that emergency physicians should know of with the novel antineoplastic agents. The adverse effects and the associated agents are briefly summarized from the article in the table below. A link to the full article is below.
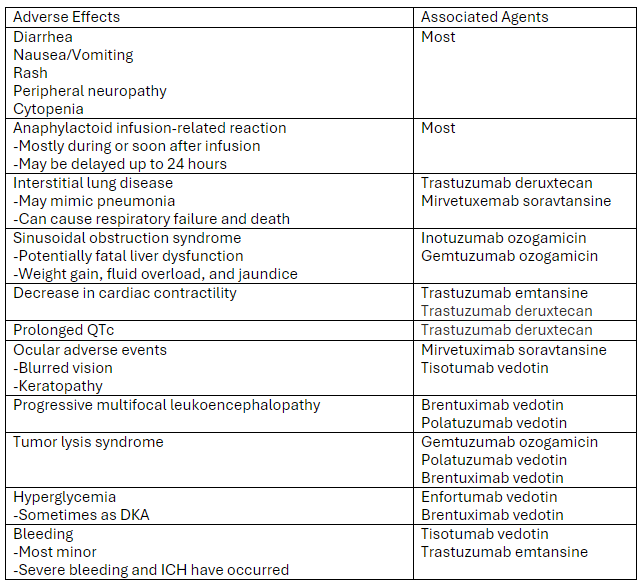
Link to article: Antibody-Drug Conjugates: The Toxicities and Adverse Effects That Emergency Physicians Must Know - Annals of Emergency Medicine
The Venous Excess Ultrasound (VExUS) exam integrates IVC, portal, hepatic, and renal vein findings to assess venous congestion and guide management, such as diuresis, in critically ill patients.
Technique:
Tips:
Interpretation:
Sometimes when other clinical information is contradictory, having the extra data point of the VExUS exam can be extremely useful to determine the best plan for a patient. Practice looking for the portal/hepatic veins and getting the waveforms on patients with a CLEAR clinical picture of venous congestion, then practice on more difficult cases.
This prospective observational study looked at patients with liver lacerations and active contrast extravasation who either had immediate embolization vs. observation. After matching for age, injury score etc. the observation first approach did as well as those who had immediate embolization.
This study tried to expand upon what they describe as the classic triad of signs to diagnose ruptured AAA “(1) abdominal pain, (2) hypotension and (3) a pulsatile abdominal mass”. They tested these against the _modified abdominal aortic aneurysm rupture signs. “_The MARS-signs encompassed (1) the registered pain-associated symptoms or signs, (2) all hypovolemic associated signs, and (3) pulsatile abdominal mass and/or ultrasound finding”. The MARS did slightly better in identifying ruptured AAA retrospectively. For me, this doesn’t add a great deal of help in making this can’t miss diagnosis and further work is necessary.
Background:
Ultrasound-guided subclavian central venous catheter (CVC) placement has become a preferred site due to low risk of infection and a low risk of complication. Complications include arterial puncture, pneumothorax, chylothorax, and malposition of the catheter. Ultrasound guidance can significantly reduce the risk of these complications aside from catheter malposition. The most common sites of malposition are in the ipsilateral internal jugular vein or the contralateral brachiocephalic vein. This study sought to evaluate the rate of catheter malposition between left-and right-sided subclavian vein catheter placement using ultrasound guidance with an infraclavicular approach.
Study:
Results:
Take Home:
For infraclavicular ultrasound-guided subclavian CVC placement, consider using the left-side over the right if no contraindications for left-sided access exist.
Early treatment of congestive heart failure (CHF) exacerbations is associated with improved mortality rates and shorter hospital length of stay. Lung ultrasound is a valuable tool in diagnosing CHF exacerbations. Recently, several studies have explored the use of lung ultrasound in the prehospital settings to expedite diagnosis and treatment.
A recent systematic review and meta-analysis evaluated the diagnostic accuracy and clinical impact of prehospital lung ultrasound. The authors found similar test characteristics to point-of-care ultrasound (POCUS) performed in the emergency department.
The eight studies included in the analysis utilized varying lung ultrasound protocols, analyzing between 2 and 8 lung zones. Notably, only two studies involved paramedics performing the ultrasounds, yet no significant difference in diagnostic accuracy was observed.
Further research is needed to evaluate the training requirements for prehospital providers and the broader impact of prehospital lung ultrasound on treatment strategies and patient outcomes.
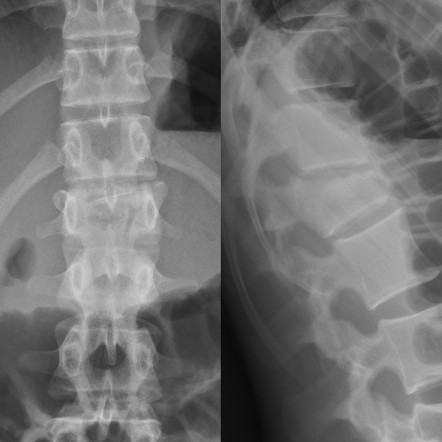
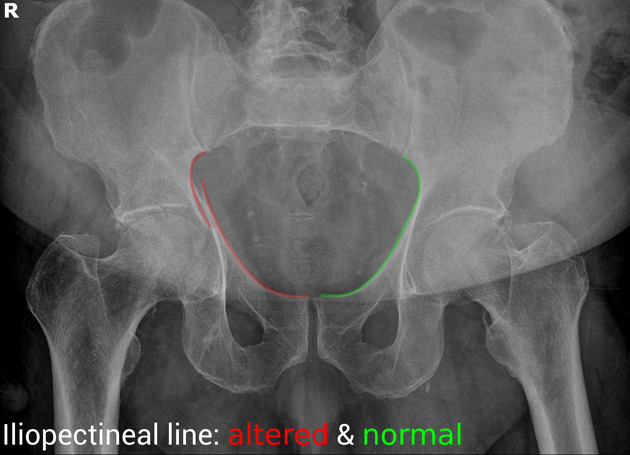
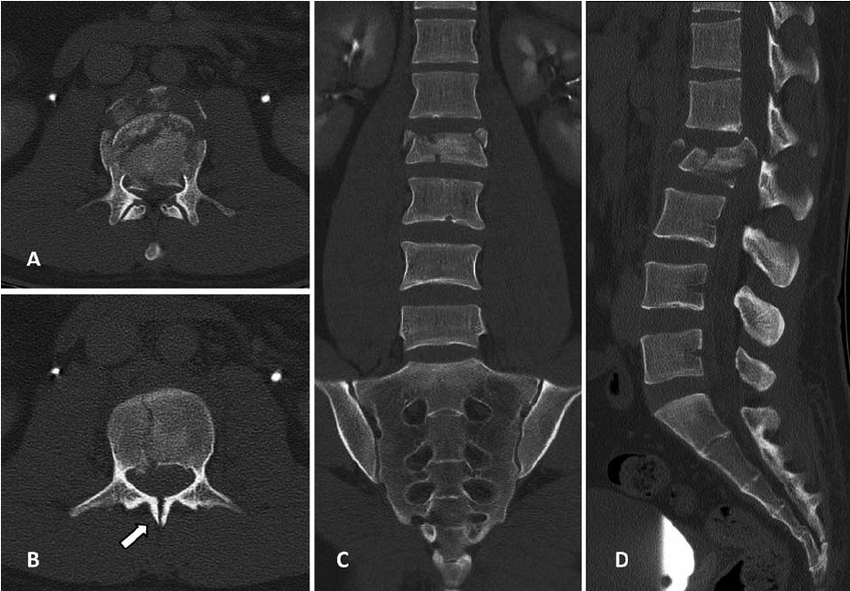
Fall from a height of 6 feet with back pain. Plain film shown. What is the diagnosis? Any further imaging indicated? Treatment? Disposition?
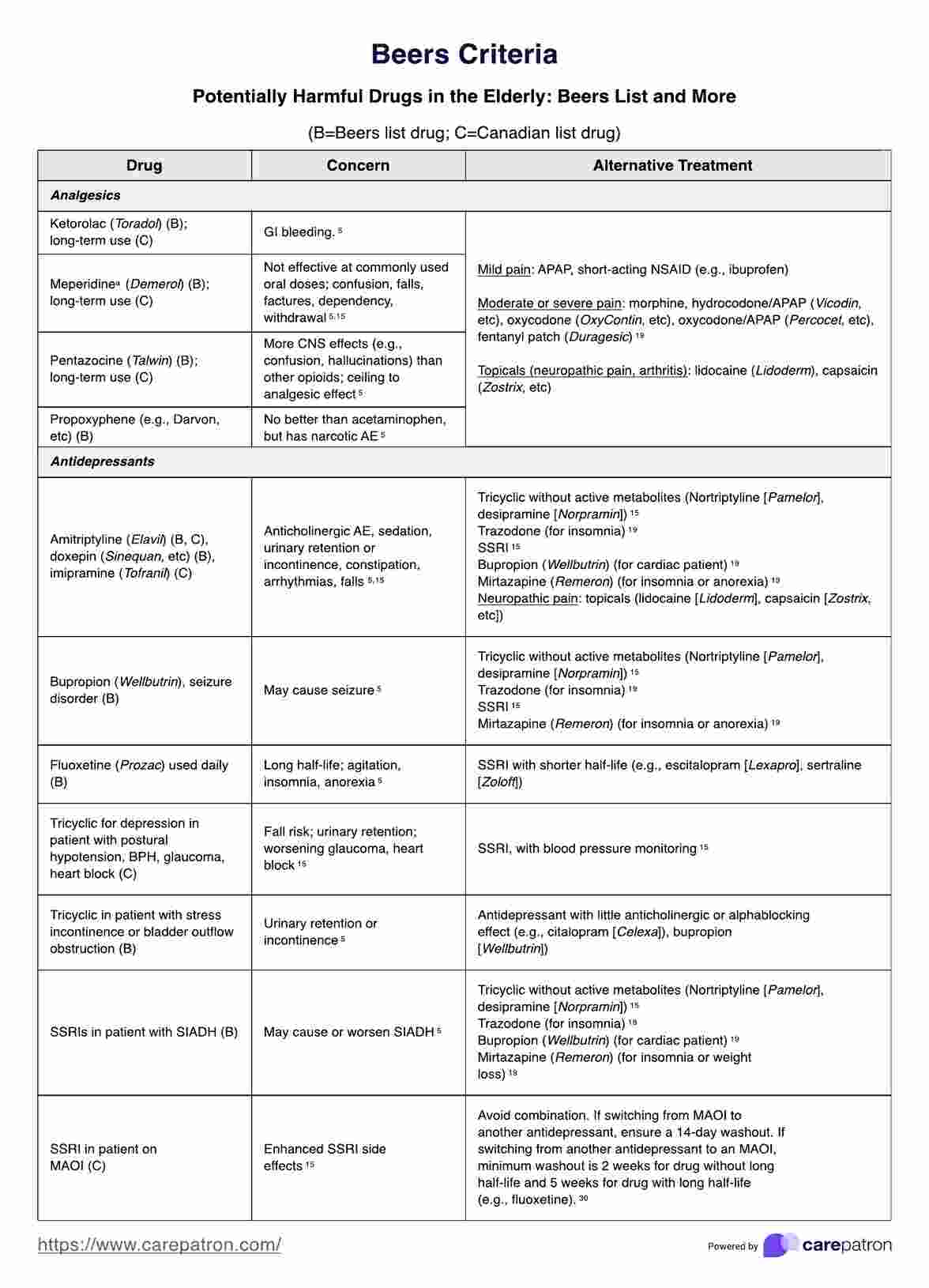
As a reminder, prescribing medications to older patients should be done with caution because of changed physiology, co-morbid conditions and other currently used medications. The Beers Criteria is a helpful list of medications that may cause trouble for your older patients. https://www.guidelinecentral.com/guideline/340784/#section-2776198 is a list of medications to either avoid or prescribe carefully in this patient population.
Pay particular attention to medications that have anticholinergic properties as they cause change in mental status and increase the risk for falls.
From all of us at UMEM, Happy Thanksgiving!!
We are incredibly Thankful for each of you and all that you do to care for patients and their families.
We are Thankful for those legends who have blazed the path in EM like Greg Henry who the EM community lost yesterday. Our thoughts are with his family. Thank you Dr. Henry for inspiring so many of us. Our pearls today are two of his famous quotes:
“Medicine is show business for ugly people.”
“You don’t go to Disney and see Mickey taking a smoke break. You have to be on when you are on shift”
Gooble, gooble,… gulp, some food for thought on the eve of Thanksgiving.
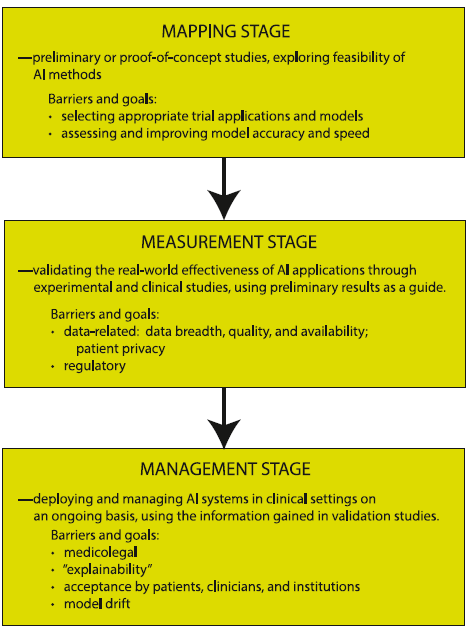
The development of artificial intelligence (AI) in emergency medicine is well under way. The schematic below and accompanying reference presents the anticipated stages in the process of AI development, including important features, considerations, and challenges as we move towards increased integration of AI in our practice of EM.
It’s the age-old question. We’ve read studies comparing propofol vs. etomidate, ketofol vs. etomidate, and now a meta-analysis about ketamine vs. etomidate. Etomidate is the staple induction agent for RSI, mostly used by Emergency Medicine, and to a degree in the Intensive Care Unit. However, the question about adrenal suppression was initiated in the early 2000s and researchers have been looking for other alternatives. This meta analysis attempted to look for another answer.
Settings: A meta-analysis of randomized controlled trials
Participants: 2384 patients who needed emergent intubation were included.
Outcome measurement: Peri-intubation instability
Study Results:
Compared with etomidate, ketamine was associated with higher risk of hemodynamic instability and moderate certainty (RR 1.29, 95% CI 1.07-1.57).
Ketamine was associated with lower risk of adrenal suppression, again, with moderate uncertainty (RR 0.54, 95% CI 0.45-0.66).
Ketamine was not associated with differences and risk of first successful intubation nor mortality.
Discussion:
Most studies were single center and involved small-moderate sample size, ranging from 20 patients to 700 patients.
For adrenal suppression, there were only 3 studies and a total of 1280 patients, thus, the results are still not definitive.
For an academic exercise, the Number Needed to Harm for both hemodynamic instability and adrenal suppression are calculated here.
Number Needed to Harm for hemodynamic instability: 25.
Number needed to harm for adrendal suppression: 11.
One of the many siginificant complications of cancers we encounter in the ED is cord compression. Here are pearls from a recently published systematic review focused on metastasis-associated spinal cord compression:
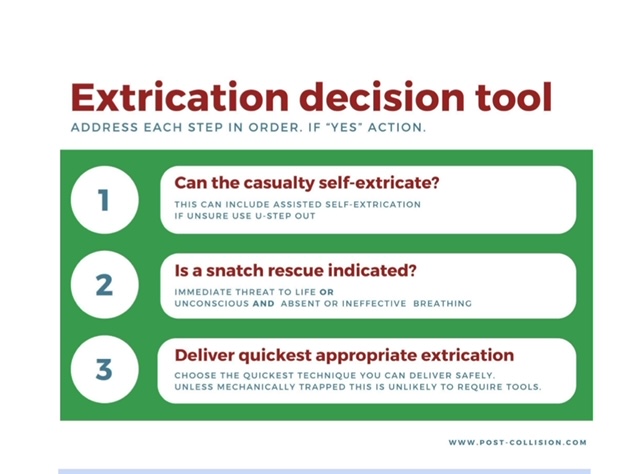
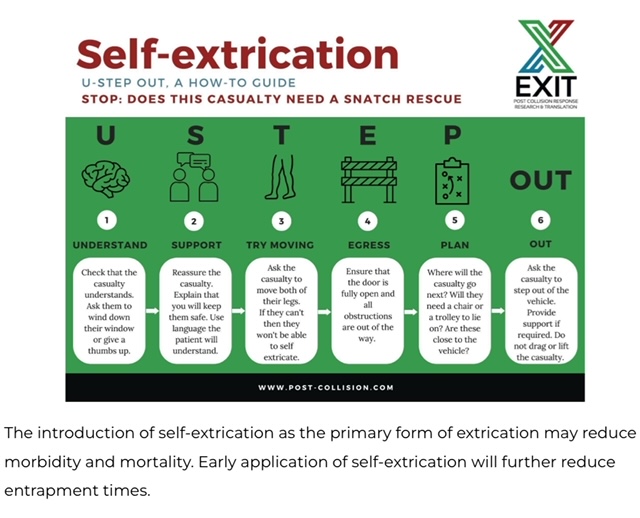
It is important for trauma and emergency care providers to understand what our patients experience prior to arrival in our clean, safe, and structured emergency department. It is also vitally important that we are involved in training and education in the pre-hospital environment. A group in the United Kingdom is challenging the age old “wisdom” that post-motor vehicle crash extrication should be slow, methodical, and work to have absolutely no movement in the spinal canal. Spinal immobilization and slow extrication instead of rapid resuscitation appears to be bad for patients. Based on several of their ground breaking papers they have published a 14 point recommendation of patient extrication post motor vehicle collision. Here are two important tenets they propose. For an in-depth discussion check out November 14, 2024 / CPD, Podcasts, Roadside to Resus.
Ankle sprains are frequently lateral.
They occur less frequently to the medial or “high” ankle.
High ankle sprains without fracture occur in 5-6% of ankle injuries presenting to the ED
Rates of injury are much higher in college and professional hockey and football players
The tibiofibular syndesmosis is primarily injured in high ankle sprains
Mechanism: Typically, external rotation or eversion on a dorsiflexed ankle
Example: When a player’s leg is forcefully rotated while foot is planted
Hx: anterior lateral ankle pain. Frequently significant pain with weight bearing.
PE: local tenderness over the syndesmosis ligaments
Two specialized tests may aid in the diagnosis
https://wikism.org/Squeeze_Test#/media/File:Squeeze_test_example.jpg
2. Dorsiflexion-external rotation test – This test attempts to reproduce the forces commonly involved in the original injury. Positive test is reproduction of pain. Position patient similar to above test. Grasp the upper calf with one hand while the other hand grasps the midfoot and places the foot in dorsiflexion and external rotation.
https://www.dralexjimenez.com/wp-content/uploads/2017/07/external-rotation-test-1.png
The authors looked at 51 patients intubated with both anterior and posterior cervical collar in place and measured the degree of movement within the spine during intubation. They repeated this process in 51 additional patients with just the posterior portion of the collar in place. They found there was one degree of difference in movement between the two groups. This adds evidence that removing the anterior portion of the collar is safe when intubating trauma patients.

{kind=link}
{kind=link}