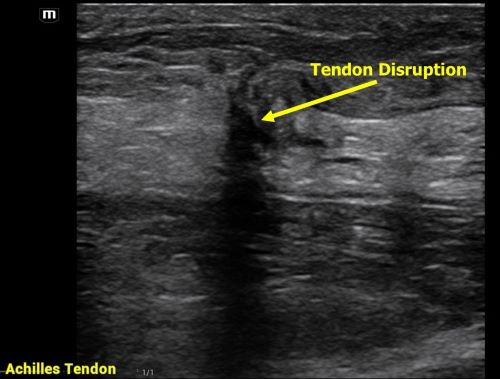
Achilles tendon injuries are commonly encountered in the emergency department. While MRIs are often unavailable, POCUS offers a quick and effective alternative for evaluating such injuries. In one review, the sensitivity of ultrasound for detecting complete Achilles tendon ruptures was 94.8%.
For the POCUS evaluation of the Achilles tendon:
- Place the patient in a prone position with their foot relaxed.
-Begin distally at the tendon’s insertion on the calcaneus and scan proximally, keeping the probe marker oriented toward the patient’s head.
-Next, obtain a transverse view by rotating the probe marker toward the patient’s right side.
-You can even do a sonographic Thompson’s Test!
Findings:
Complete Rupture: Displays as a full disruption of the tendon fibers.
Partial Tear: Shows intact tendon tissue with surrounding edema.
Tendinitis: Appears as a thickened tendon with increased vascularity on color Doppler imaging.
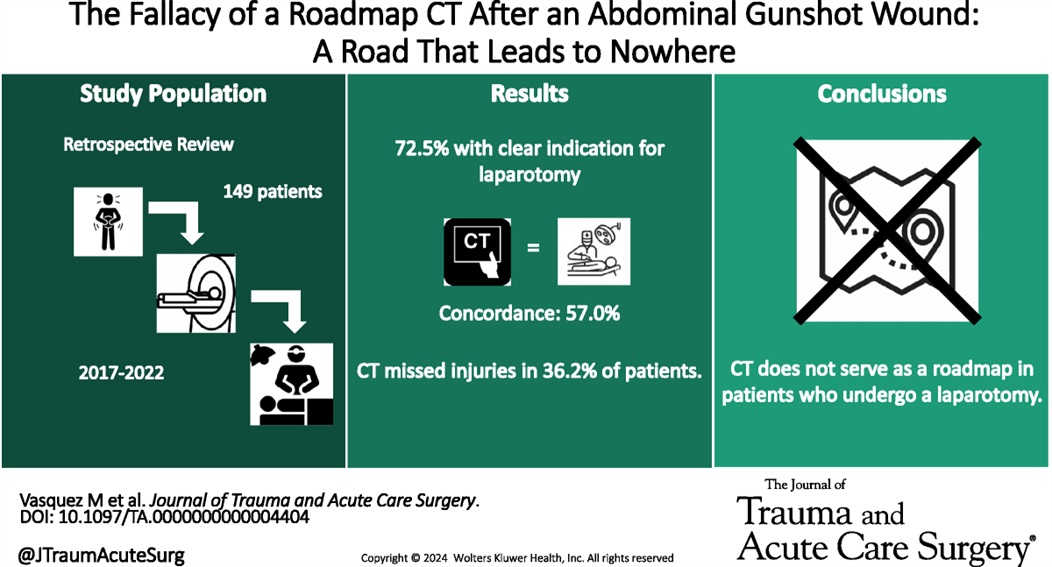
This retrospective study illustrates that the use of CT scanning to identify injury in gun shot wounds to the abdomen is not sensitive or specific enough to obviate the need for laparotomy. “Admission hypotension, abdominal pain and/or peritonitis, evisceration, and a transabdominal trajectory were considered clear indications for laparotomy.” If there is clear indication to go to the OR, stopping in CT does not add any benefit.
This article was a review of randomized control trials using intranasal (IN) fentanyl. There were 8 studies included that showed IN fentanyl was superior to controlling pain compared to other pain medications at the 15-20 minute mark, but not at the 30 and 60 minute marks. There were less reports of nausea and vomiting with IN fentanyl, but no difference in dizziness or hallucinations compared to the other medications included in the various trials (ie morphine, ketamine, po narcotics, ect)
The bioavailability of IN fentanyl ranges from 71-89% with effects noted in 2 minutes with maximal concentrations noted at 7 minutes. The half life is approximately 60 minutes.
Bottom line: Consider IN fentanyl for quick acute pain management in the pediatric patient.
An out-of-hospital, randomized, placebo-controlled, blinded, parallel group study was conducted in adult patients under the care of the city fire-based emergency medical services and the local level one trauma center. Adult male patients experiencing moderate to severe pain due to traumatic injuries received either 50mg of intranasal ketamine or placebo in addition to fentanyl after randomization in the field by the paramedic (a novel approach). The primary outcome was reduction of pain by 2 points 30 minutes after study drug administration.
199 patients were randomized with 107 receiving ketamine and 92 with placebo. Patients were young (30-40), and had a median weight of 83 kg. Pretreatment pain scores were 10/10 and patients presented to the ED 14 minutes after receiving study medication. The most common injuries were falls, MVC, and GSW. Half of the patients received IV fentanyl but others had IM or IN routes.
Ketamine receipt did not lead to a 2 point reduction in pain scores (36% vs 44.7% p = 0.22). There was no difference in pain at 3 hours, additional medications received, or total amount of analgesia received. Notably, there were no differences in adverse events.
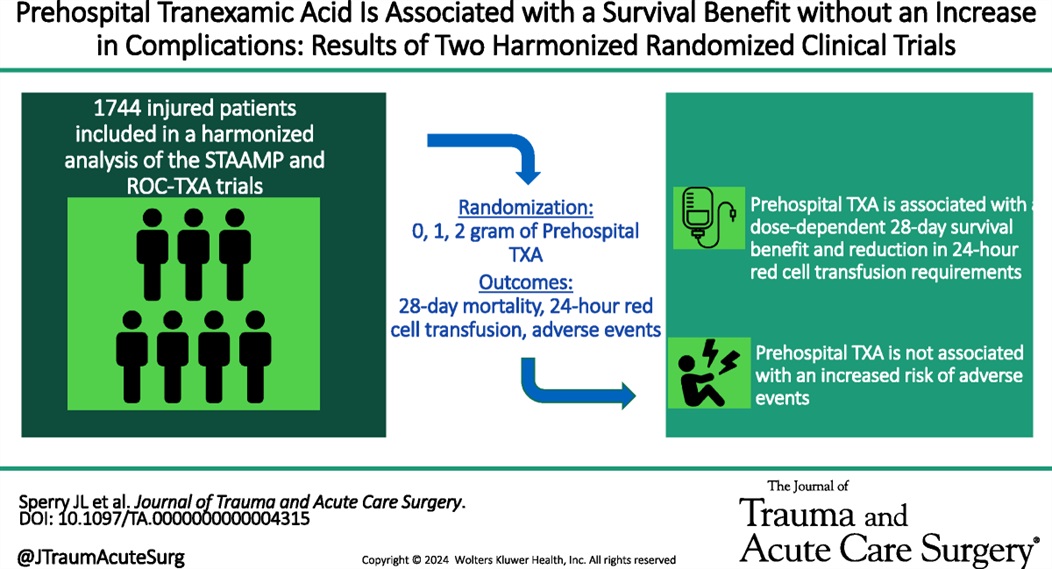
Administration of prehospital TXA was found to improve 28 day mortality and decrease the amount of blood required to be transfused without any increased risk of thromboembolism or seizure. Two grams of TXA was superior to one gram and no TXA.
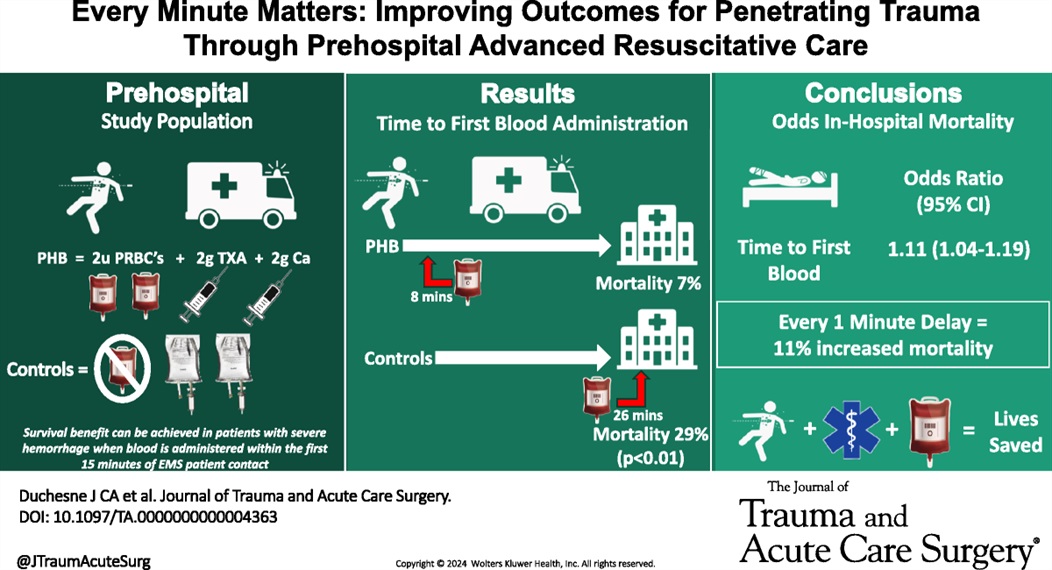
In this small retrospective study comparing outcomes before and after a prehospital blood administration protocol for penetrating trauma was initiated, the authors found improved survival in those receiving prehospital blood despite a five minute longer on scene time in those receiving blood. Also note TXA was part of the blood protocol but not the control group.
Trigger finger/thumb
Occurs from mechanical impingement
-Stenosing tenosynovitis
Much more common in patients with diabetes
Causes clicking, catching, locking and pain
Occurs at the A1 pulley
Flexor tendon “catches” as it attempts to glide through a stenotic flexor tendon sheath
Initially, patient's report painless catching or locking of the affected digit during flexion
During finger flexion and extension, pain is caused by inflamed tendon passing through a relatively constricted tendon sheath
Occurs most often in the ring and middle digits
May improve over the course of the day
Diagnoses with active triggering (with digit flexion and extension) and tenderness to palpation at the first annular pulley (A1) which overlies the first MCP joint
-Ask patient to place hand on table face up and gradually fully flex and extend the fingers
May note a palpable nodule of the flexor tendon
Treatment: Activity modification, NSAIDs and splinting (3-6 weeks)
Corticosteroid injection is very effective
https://www.ahta.com.au/client_images/2553101.png
Neonates are more prone to seizures than children of other ages. Ultimately, a cause of seizures is more likely to be identified in the newborn. Neonatal seizures are subtle and careful attention to repetitive motions of the face, arms or legs should be considered worrisome for seizure. Generalized tonic clonic seizures are rare in this patient population.
Common Causes:
Hypoxic ischemic encephalopathy (most common), infection, stroke, non-accidental trauma, intracranial hemorrhage (including from vitamin K deficiency), metabolic disorders, and structural abnormalities.
Guidelines for Treatment:
Phenobarbital should be used as first line, unless there is concern for channelopathy based on family history. Some literature does suggest possible benefits of a benzodiazepine in conjunction with phenobarbital for seizure cessation, but care should be given due to high risk for respiratory suppression in neonates.
For seizures that are unresponsive to first line treatment, consider phenytoin, levetiracetam, midazolam, or lidocaine.
A trial of pyridoxine can be attempted in patients who are unresponsive to initial measures
Evaluation:
Neonatal seizures require a full evaluation, including labs, head imaging (MRI preferred), low threshold for LP post imaging, concern for trauma
Disposition:
Neonates presenting with seizures require admission to the hospital for ongoing evaluation and monitoring.
In out of hospital cardiac arrest (OHCA), does it matter if you choose an intraosseous (IO) vs intravenous (IV) approach to getting access and giving meds?
No, according to a recent study by Couper et al, just published in NEJM. No significant difference in any clinically meaningful outcome including survival, neurologically intact discharge, etc. Technically the IV group had slightly higher rates of ROSC, which just met statistical significance, and to be fair that group did trend very slightly towards better outcomes in some categories, but really well within the range expected by statistical noise.
Interestingly, the median time from EMS arrival to access being established was the same in both groups (12 minutes), which I think raises some face validity questions. Furthermore, of course, previous trials have raised questions as to whether ACLS meds even work or impact outcomes anyways, so naturally if they don't, the method by which they are given isn't likely to matter either.
Bottom Line: This large, well conducted trial continues to support the notion that either an IV-focused, or IO-focused approach to access and medication delivery in OHCA is reasonable. You and your prehospital colleagues can likely continue to make this decision based on personal comfort, local protocols, and patient/case circumstances. At the very least, this continues to support the notion that if an IV is proving challenging, pursuing an IO instead is a very appropriate thing to do.
If significant orbital edema prevents visual assessment of the pupillary light reflex, ocular ultrasound can be a useful alternative.
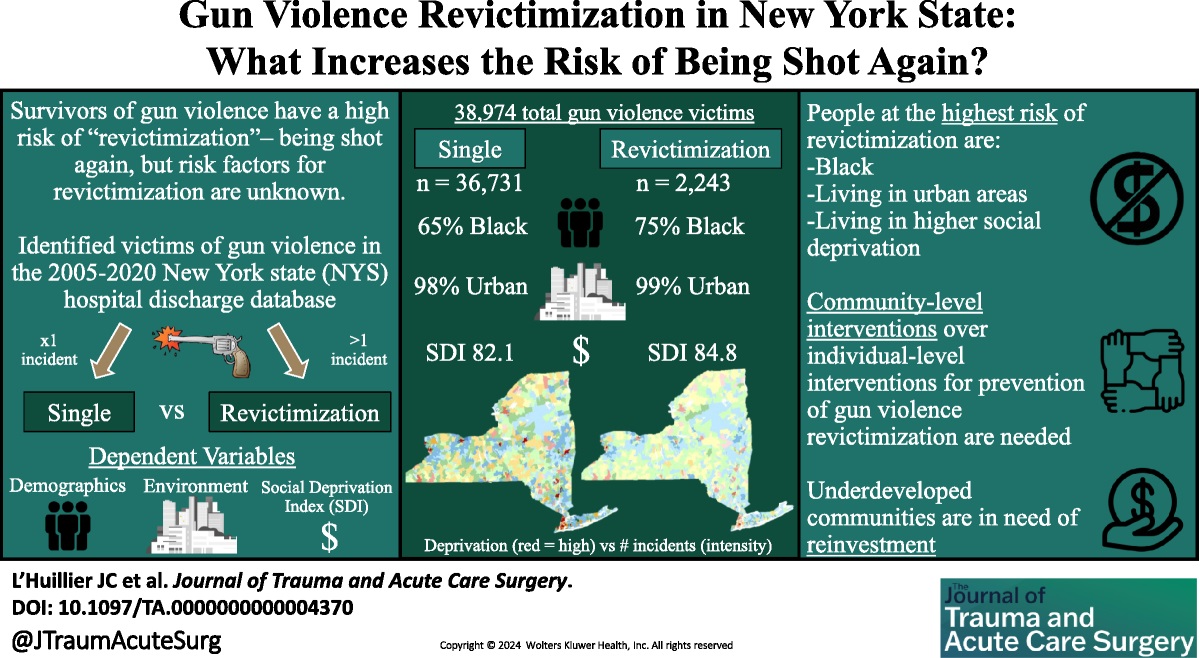
This study used the New York State hospital discharge database to look for factors associated with being the victim of repeat gun violence.
Unanswered questions include: is it similar in other areas, what interventions at the patient level could prevent this, what other patient level factors (substance use, etc) are involved, however, this is a good start in looking at this preventable disease.
Recent studies continue to highlight that Black, Native American, female, uninsured and Medicaid patients receive disproportionately more substance use screening when they are trauma patients. The authors of this paper point out that this inappropriate application of screening leads to missed opportunities.
“Screening patients for drug and alcohol use following injury is an evidence-based practice that can trigger wraparound care, such as brief substance use interventions, to prevent reinjury. Adolescents who consume alcohol but are not screened for alcohol use have 2- to 3- fold greater likelihood of reinjury compared with those who were screened and received a brief intervention.”
By Bobbi-Jo Lowie, MD
Assistant Professor
Emergency Medicine
University of Maryland School of Medicine
Since April of 2024 there have been 36 confirmed cases of avian influenza A across the United States. Avian influenza, primarily caused by influenza viruses that infect birds, can pose significant health risks to both animals and humans. The most notable strains include H5N1 and H7N9, with H5N1 being particularly alarming due to its high mortality rate among infected humans. The virus primarily spreads from birds to humans through direct contact with infected birds, their droppings, or contaminated environments. Although there have been recorded cases of human-to-human transmission, this usually occurs only in close-contact situations.
In humans, avian influenza can present with symptoms ranging from mild respiratory illness to severe pneumonia. Patients may experience fever, cough, sore throat, muscle aches, and in severe cases, gastrointestinal symptoms. Those that have more moderate or severe illness may develop shortness of breath, altered mental status, or seizures. Complications include acute respiratory failure, pulmonary hemorrhage among others, with respiratory failure being the most common cause of death in this patient population.
Diagnosing avian influenza involves a combination of clinical presentation, travel history, and exposure to birds and confirmation through PCR testing of upper respiratory tract samples like a nasopharyngeal swab.
Treatment for avian influenza focuses on antiviral medications such as oseltamivir which is most effective when administered early in the course of the illness but still administered after 48 hours of illness. Supportive care is essential for managing severe cases, especially those that progress to acute respiratory distress syndrome.
Hypertension in the ED comes in two varieties: emergency and asymptomatic (not urgency!). From this position statement: “Hypertensive emergency involves acute target-organ damage and should be treated swiftly, usually with intravenous antihypertensive medications, in a closely monitored setting.”
Conversely, asymptomatic does not require urgent, aggressive management. “Recent observational studies have suggested potential harms associated with treating asymptomatic elevated inpatient BP, which brings current practice into question.”
Without target organ involvement, we do not need to be initiating IV medications or trying to treat the numbers
Cardiovascular disease (CVD) and cancer are leading global causes of illness and death, and evidence increasingly shows they are interconnected. There is strong epidemiological data that the two disease entities share modifiable risk factors such as hypertension, hyperlipidemia, diabetes, obesity, smoking, diet, physical activity, and social determinants of health.
Shared mechanisms underlying both CVD and cancer include:
Take home points:
Keep all this in mind especially when seeing cancer and CVD patients in your ED!
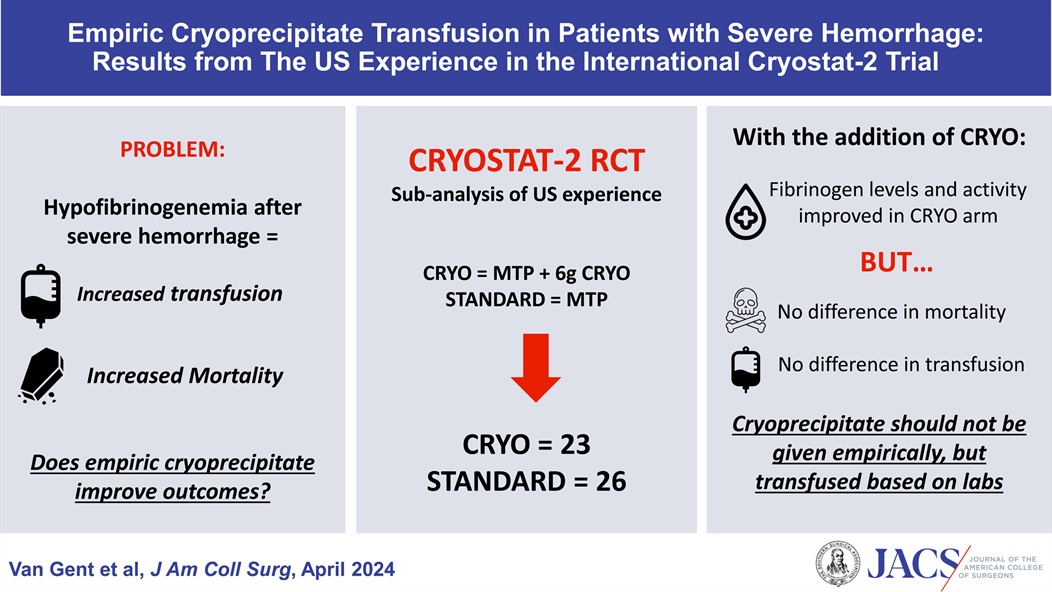
There is uncertainty if adding cryopercipitate empirically to all mass hemorrhage protocols has any benefit to mortality, need for transfusion, or any other meaningful outcome. This small study suggests it does not and that we should save the addition of cryopercipitate to those with lab proven low fibrinogen levels.
Olecranon bursitis
Superficial synovial membrane located overlying the proximal ulna/olecranon allows for easy irritation and inflammation
Swelling does not involve the joint
Most common bursitis (approx. 4x more common than prepatellar)
Male>>Female
Prone to trauma, inflammation or infection
-RA, gout, overlying break in skin
Chronic inflammation results from excessive leaning on the elbow such as with certain occupations (plumber, military recruit)
Inflammation may be septic or aseptic
Usual cause is traumatic
Approximately 20% of acute cases may have a septic origin
Classically appears as a “goose egg” area on posterior elbow
Well-demarcated and fluctuant
Small amount of swelling and/or those with minimal symptoms should be left alone and treated with activity modification, NSAIDS, ice. Suggest an elbow pad for protection.
If this does not resolve symptoms after approximately 4 weeks, consider referral for aspiration and steroid injection
If aspiration is ED performed for evaluation of possible septic bursitis, recommend a compressive elbow sleeve to help prevent reaccumulating
If a recurrent issue for patient and aspirated, consider a posterior elbow splint for approx. 10 days and refer to orthopedics.
For penetrating neck trauma:
Does it violate the platysma if no, close wound and discharge
If yes, are there any hard signs of injury like enlarging hematoma, air from the wound, difficulty swallowing, blood in the airway, respiratory distress then to the OR
If no, Ct angio of the neck. If negative and no other findings admit for observation or discharge. If positive, to the OR. If equivocal, endoscopy and broncoscopy.
No longer think about the zones of the neck. Treat them all the same.

Does physician altruism influence quality metrics? This study suggests yes.
45 physicians were defined as “altruistic” based on their willingness to share a $250 cash prize with a stranger in an on-line version of the dictator game, something you might have played in an economics class.
Of 250 physicians drawn from primary care and cardiology, 45 met the definition of altruistic and 205 did not.
Overall, patients of altruistic physicians:
The authors suggest that this difference may be on account of altruistic physicians being more willing to consider the appropriateness of tests or treatment or “devote more time and energy to their patients.”
They also note that while most physicians were categorized as not altruistic, at 18% this group of physicians exceeds the 5% of the general US population that would meet this definition.
Perhaps there is something quantitatively demonstrable to being a “good” doctor.
See https://jamanetwork.com/journals/jama-health-forum/fullarticle/2824419
Intravascular Volume and the IVC
{kind=link}
{kind=link}