Category: Critical Care
Posted: 3/21/2023 by Mike Winters, MBA, MD
(Updated: 6/18/2026)
Click here to contact Mike Winters, MBA, MD
Things to Consider for Persistent or Worsening Septic Shock
Teja B, et al. How we escalate vasopressor and corticosteroid therapy in patients with septic shock. Chest. 2023; 163:567-74.
Category: Trauma
Keywords: trauma, whole blood, reduction, blood products, MHP, Shock index, RABT, hemorrhage (PubMed Search)
Posted: 3/19/2023 by Robert Flint, MD
(Updated: 6/18/2026)
Click here to contact Robert Flint, MD
Predicting the need for a mass hemorrhage protocol (MHP) activation is important both for individual patient outcome as well as for proper utilization of critical resources such as blood products and healthcare workers time and effort. These two studies look at using the RABT score to predict the need for mass transfusion. The RABT score is:
A 4-point score
blunt (0)/penetrating trauma (1),
shock index (hr/SBP)≥ 1 (1),
pelvic fracture (1)
FAST positive (1)
With a score >2 predictive of needing MHP.
These studies (one in Canadian trauma centers, the other in US trauma centers) validate the use of this score to predict the need for activation of a mass hemorrhage protocol.
1, Prediction of massive transfusion with the Revised Assessment of Bleeding and Transfusion (RABT) score at Canadian level I trauma centers Karan D'Souza , Mathew Norman , Adam Greene , Colby J.F. Finney Matthew T.S. Yan , Jacqueline D. Trudeau , Michelle P. Wong , Andrew Shih , Philip Dawe Injury Volume 54, Issue 1, January 2023, Pages 19-24
2.2. Multicenter Validation of the Revised Assessment of Bleeding and Transfusion (RABT) Score for Predicting Massive Transfusion Kamil Hanna 1, Charles Harris , Marc D Trust , Andrew Bernard , Carlos Brown , Mohammad Hamidi , Bellal Joseph World J Surg 2020 Jun;44(6):1807-1816. doi: 10.1007/s00268-020-05394-5.
Category: Pediatrics
Keywords: Croup, respiratory distress, stridor, URI (PubMed Search)
Posted: 3/17/2023 by Jenny Guyther, MD
(Updated: 6/18/2026)
Click here to contact Jenny Guyther, MD
Scribner C, Patel K, Tunik M. Pediatric Croup Due to Omicron Infection Is More Severe Than Non-COVID Croup. Pediatr Emer Care 2022;00.
Category: Trauma
Keywords: thoracic trauma, rib fractures, Sweden, trauma, 30 day mortality (PubMed Search)
Posted: 3/12/2023 by Robert Flint, MD
(Updated: 6/18/2026)
Click here to contact Robert Flint, MD
This study from Sweden looked at 2397 trauma patients and identified 768 with thoracic injury. Those with thoracic injury had a 30-day mortality of 11% whereas those without thoracic injury had a 4% 30-day mortality. Patients over age 60 had higher mortality and were more likely to have rib fractures. Those under 60 with thoracic injury were more likely to have thoracic organ injury than rib fracture.
Bottom line: Rib fractures were more common over age 60 and there was a higher mortality for those with thoracic vs non-thoracic trauma.
Lundin, A., Akram, S.K., Berg, L. et al. Thoracic injuries in trauma patients: epidemiology and its influence on mortality. Scand J Trauma Resusc Emerg Med 30, 69 (2022). https://doi.org/10.1186/s13049-022-01058-6
https://rdcu.be/c7q1w
Category: Critical Care
Keywords: ECG; status epilepticus (PubMed Search)
Posted: 3/7/2023 by Quincy Tran, MD, PhD
(Updated: 6/18/2026)
Click here to contact Quincy Tran, MD, PhD
Title: Electrocardiographic Changes at the Early Stage of Status Epilepticus: First Insights From the ICTAL Registry.
As the song goes: “the thigh bone is connected to the hip bone, the hip bone is connected to the back bone.” It turns out that the brain electrical activities are also connected to the heart conduction activities.
In a multi-center (23 French ICUs) retrospective analysis of 155 critically ill patients with status epilepticus, ECGs were done within 24 hours of onset of status epilepticus, and were independently reviewed by cardiologists showed abnormalities in 145 (93.5%) of patients.
Below is a list of events that occurred more than 10% of events.
Abnormal rate (<60 or > 100 beats/min 64 (44%)
Negative T-waves 61 (42%)
Flattened T-waves 18 (12%)
ST elevation 24 (16.6%)
ST depression 26 (17.9%)
Left axis deviation 22 (15.9%)
Discussion:
Major ECG abnormalities were not associated with 90-day functional outcome in multivariable logistic regression.
The brain-heart axis could be affected by antiseizure medication. For example, phenytoin, lacosamide are sodium channel blockers while benzodiazepines, propofol, barbiturates with their GABAnergic effects will also display cardiac side effects. This current study was not able to tease out whether the cardiac effects were from medication. Therefore, further studies are needed to figure out the cardiac effect for patients with status epilepticus.
Chinardet P, Gilles F, Cochet H, Chelly J, Quenot JP, Jacq G, Soulier P, Lesieur O, Beuret P, Holleville M, Bruel C, Bailly P, Sauneuf B, Sejourne C, Galbois A, Fontaine C, Perier F, Pichon N, Arrayago M, Mongardon N, Schnell D, Lascarrou JB, Convers R, Legriel S. Electrocardiographic Changes at the Early Stage of Status Epilepticus: First Insights From the ICTAL Registry. Crit Care Med. 2023 Mar 1;51(3):388-400. doi: 10.1097/CCM.0000000000005768. Epub 2022 Dec 19. PMID: 36533915.
Category: Trauma
Keywords: EMS, C-Spine, Canadian C-Spine Rule, spinal injury, trauma (PubMed Search)
Posted: 3/5/2023 by Robert Flint, MD
Click here to contact Robert Flint, MD
Applying a cervical collar to all patients involved in motor vehicle collisions and mechanical falls has been shown to add to patient discomfort, unwarranted imaging studies and prolonged on scene time for emergency medical services. This study adds further evidence that paramedics can use validated algorithms to clinically clear cervical spine injuries without any bad outcomes including spinal cord injuries. EMS medical directors and all of us who interact with EMS providers should be proactive in developing protocols to use cervical immobilization in appropriately selected patients only. This study used the Modified Canadian C-Spine Rule.
Implementation of Modified Canadian C-Spine Rule by Paramedics
Christian Vaillancourt, Manya Charette, Julie Sinclair, Richard Dionne, et al
Annals of Emergency Medicine Volume 81, No.2 February 2023. 187-196.
Category: Pharmacology & Therapeutics
Keywords: atrial fibrillation, atrial flutter, diltiazem, calcium (PubMed Search)
Posted: 3/3/2023 by Ashley Martinelli
(Updated: 6/18/2026)
Click here to contact Ashley Martinelli
Non-dihydropyridine calcium channel blockers, verapamil and diltiazem, can induce hypotension when administered intravenously (IV) in approximately 4% of patients. It has previously been taught that administering IV calcium before administering these medications may prevent the hypotension. Previously, this theory was tested for verapamil and found success with reducing hypotension. Only one study has been done exclusively with diltiazem and it found no benefit.
In a new multicenter retrospective cohort study of adults in the ED, patients were randomized into two groups: those who received diltiazem alone and those who received calcium with diltiazem for atrial fibrillation/atrial flutter (AF/AFL) with a HR ≥ 120 bpm. Patients were excluded if they required electrocardioversion, had other agents prior to diltiazem, incomplete information, were pregnant or incarcerated. The primary outcome was change in SBP 60 minutes (+/-30 minutes) after diltiazem administration.
Baseline characteristics: 73 year old, equal male:female, predominantly white patients. 40% had new onset AF/AFL and the initial HR was 140 in both groups. There were 198 patients in the diltiazem group and 56 patients in the combination group. Notably, patients in the combination group had a lower presenting SBP 109 (101-121) vs 123 (114-132) P<0.0001 which matches classical teaching for when to consider calcium use. Additionally, patients in the combination group received a lower diltiazem dose of 10mg vs 15mg in the monotherapy group p=0.004 with both group receiving doses lower than the standard 0.25 mg/kg dosing recommendation.
Outcomes:
Take Home Point:
Administration of IV calcium may not be as beneficial as previously thought to prevent hypotension induced by diltiazem administration. This particular study is confounded by the relatively low doses of diltiazem overall, but utilizing a lower dosing strategy in patients with low SBP is a reasonable safety strategy.
Rossi N, Allen B, Hailu K, et al. Impact of intravenous calcium with diltiazem for atrial fibrillation/flutter in the emergency department. Am J Emergency Medicine. 2023;64:57-61.
Category: Critical Care
Posted: 3/1/2023 by Caleb Chan, MD
Click here to contact Caleb Chan, MD
Background:
There have been a few studies that suggested that there may be some neuroprotective effect with a higher MAP goal in post-arrest patients. However, these studies were small and/or observational.
Intervention:
-The BOX trial was a double-blind, dual-center (Denmark), randomized trial
-Study population: >18 yo, OHCA of presumed cardiac cause
-Pts randomized to higher (77 mmHg) vs. lower (63 mmHg) MAP goal
-double-blinded by attaching a module that reported a BP that was 10% higher or lower than the pt’s actual BP
-Notable exclusion criteria:
-unwitnessed asystole or suspected intracranial bleeding/stroke
Results/Primary outcome:
-No sig difference in composite of death + Cerebral Performance Category of 3 or 4 (3= severe disability, 4= coma) within 90 days
-133 patients (34%) in the high-target group vs 127 patients (32%) in the low-target group (hazard ratio, 1.08;95%CI, 0.84 to 1.37; P=0.56)
Caveats/Takeaways:
-Mean difference in BP was 10.7 mmHg (95[CI], 10.0 to 11.4) which is still relatively clinically significant, but was lower than their goal difference of 14 mmHg
-They used IVF to target a CVP of 10 mmHg prior to initiation of norepi and used dopamine "if necessary"
-Consider generalizability given study population was patients with presumed cardiac cause of arrest
-Keeping a lower MAP goal of >65 mmHg is reasonable in post-arrest patients
Kjaergaard J, Møller JE, Schmidt H, et al. Blood-pressure targets in comatose survivors of cardiac arrest. N Engl J Med. 2022;387(16):1456-1466.
Category: Trauma
Keywords: substance abuse, trauma, fentanyl, injury (PubMed Search)
Posted: 2/26/2023 by Robert Flint, MD
(Updated: 6/18/2026)
Click here to contact Robert Flint, MD
In a small study at a single level one trauma center, ? of patients screened positive for illicit fentanyl use prior to violent or intentional injury. Those who screened positive were more likely to require ICU admission and had a higher rate of previous trauma center admission. The authors concluded:
“Exposure to illicit fentanyl was common among victims of violence in this single-center study. These patients are at increased risk of being admitted to intensive care units and repeated trauma center visits, suggesting fentanyl testing may help identify those who could benefit from violence prevention and substance abuse treatment.”
Illicit Fentanyl Exposure Among Victims of Violence Treated at a Trauma Center
ACUTE CARE SURGERY| VOLUME 283, P937-944,
Kyle R. Fischer, MD, MPH
Timothy Traynor, BS
Benoit Stryckman, MA
Joseph Richardson, PhD
Laura Buchanan, MD
Zachary D.W. Dezman, MD, MS
Category: Orthopedics
Keywords: wrist pain (PubMed Search)
Posted: 2/25/2023 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
21-year-old college softball player presents for evaluation of Left hand/wrist pain following batting practice.
She states her pinky is “tingly”
On exam, there is tenderness over her volar ulnar wrist.
You obtain an X-ray.
https://prod-images-static.radiopaedia.org/images/52314027/a662d8f338ec08ba56178463638d25_jumbo.jpeg
What’s the diagnosis?
Hook of the hamate fractures are often associated with sports that require a firm hand grip such as baseball, softball, tennis, golf. These sports cause repeated stress against the hamate bone from the gripped sporting equipment. A frequent mechanism is grounding a golf club or from the act of checking a baseball bat swing.
On physical exam, the most common finding is focal tenderness over the hook of the hamate.
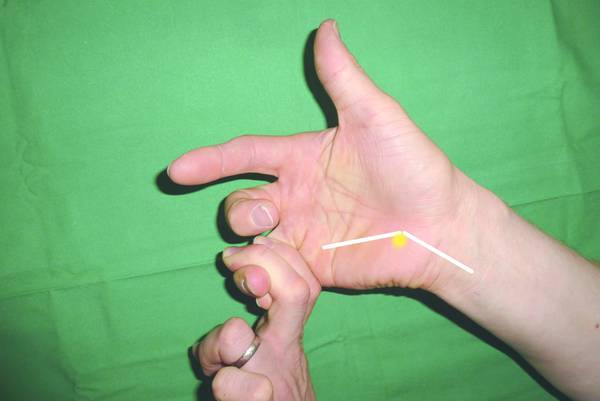
Another test with high sensitivity is a hook of the hamate pull test
Place the patient's hand in ulnar deviation and ask patient to flex the DIP joints of the 4th and 5th digits against resistance.
https://musculoskeletalkey.com/wp-content/uploads/2016/06/9783131746214_006_002.tif_epub1.jpg
Imaging: PA and lateral wrist views are frequently negative despite being the first line recommended imaging for wrist pain/trauma.
A carpal tunnel view has much better sensitivity to visualize the hook of the hamate.
Base fractures (less common than hook) may also be missed on carpal tunnel view and require advanced imaging using CT.
Place patient in ulnar gutter splint and arrange follow up with hand surgery.
Overall, this is an uncommon though frequently missed injury. Consider the above mentioned physical exam and imaging recommendations to improve diagnostic accuracy.
Category: Critical Care
Posted: 2/21/2023 by William Teeter, MD
(Updated: 2/22/2023)
Click here to contact William Teeter, MD
Given my previous post on APRV (11/6/2022) and while I take issue with many of the author's statements, I wanted to share a very well referenced article with an excellent discussion on the current gaps in the knowledge around APRV and its use.
One statement I do agree with is the need for a well-designed and adequately powered trial of this mode in an admittedly difficult-to-study population.
Fortunately, this article has an invited rebuttal pending from Dr. Habashi which I am sure will appear in the Educational Pearls in short order.
Good luck to the residents on the ITE!
Parhar, Ken Kuljit S. MD, MSc1,2,3; Doig, Christopher MD, MSc1,2,4. Caution—Do Not Attempt This at Home. Airway Pressure Release Ventilation Should Not Routinely Be Used in Patients With or at Risk of Acute Respiratory Distress Syndrome Outside of a Clinical Trial. Critical Care Medicine ():10.1097/CCM.0000000000005776, January 20, 2023. | DOI: 10.1097/CCM.0000000000005776
Article at https://pubmed.ncbi.nlm.nih.gov/36661571/
Category: Trauma
Keywords: head injury, anticoagulation, delayed, intracranial, warfarin, DOAC, risk (PubMed Search)
Posted: 2/18/2023 by Robert Flint, MD
(Updated: 6/18/2026)
Click here to contact Robert Flint, MD
This study looked at 69,321 head injured patients over age 65 in a health care database for delayed intracranial hemorrhage (within 90 days of visit). 58,233 patients were not on oral anticoagulants, 3081 (4.4%) were on warfarin and 8007 (11.6%) were on direct oral anticoagulants. One percent of patients not on anticoagulation and those on oral direct anticoagulation had a delayed hemorrhage while those on warfarin had a 1.8% delayed hemorrhage rate.
Bottom Line: Direct oral anticoagulants do not increase the risk of delayed intracranial hemorrhage in patients over age 65 from baseline but warfarin does.
Sharon Liu et al Delayed intracranial hemorrhage after head injury among elderly patients on anticoagulation seen in the emergency department CJEM 2022 Dec:24(8):853-861 doi:10.1007/s43678-022-00392-z.
Category: Pediatrics
Keywords: conjunctivitis, pink eye, eye drops (PubMed Search)
Posted: 2/17/2023 by Jenny Guyther, MD
(Updated: 6/18/2026)
Click here to contact Jenny Guyther, MD
Honkila et al. Effect of Topical Antibiotics on Duration of Acute Infective Conjunctivitis in Children. JAMA Network Open. 2022;5(10):e2234459.
Category: Critical Care
Keywords: high dose, nitroglycerine, SCAPE, Sympathetic Crashing Acute Pulmonary Edema, flash pulmonary edema (PubMed Search)
Posted: 2/14/2023 by Zach Rogers, MD
Click here to contact Zach Rogers, MD
Sympathetic Crashing Acute Pulmonary Edema (SCAPE) (also known as flash pulmonary edema) is an extreme form of hypertensive acute heart failure where a surge of high blood pressure from catecholamine surge and sudden vascular redistribution causes sudden onset decompensated heart failure hallmarked by rapid pulmonary edema and symptoms of hypoxia and dyspnea.
This is treated by systolic blood pressure control and venous vasodilation with IV nitroglycerine, bilevel positive airway pressure (BPAP), and diuretics if needed. A common error in treatment is administration of the traditional IV nitroglycerine infusion dosing protocol in which the nitroglycerine infusion is started at 5 mcg/min and slowly increased by 5 mcg/min increments until the clinical response is seen. However, in this syndrome, rapid blood pressure control and correction of vascular redistribution is critically important to reverse the central factor for patient decompensation. Lack of blood pressure control places the patient at risk of further cardiac decompensation or respiratory failure ultimately requiring intubation.
Increasing literature has been published on the concept of high dose or push dose IV nitroglycerine for the treatment of this syndrome. Many of these studies show decreased rates of intubation, decreased ICU admissions, and shorter hospital length of stays with high dose or push dose nitroglycerine, while also demonstrating low risk of hypotension.
The actual dose of the high-dose nitroglycerine administered in these trials is variable, with some trials administering nitroglycerine 1-2 mg IV pushes every 3-5 minutes, and other trials using a nitroglycerine infusion at a much higher starting rate (between 200-400 mcg/min) with rapid down-titration as blood pressure is controlled.
Collins, S., Martindale, J. Optimizing Hypertensive Acute Heart Failure Management with Afterload Reduction. Curr Hypertens Rep 20, 9 (2018). https://doi.org/10.1007/s11906-018-0809-7
Wilson SS, Kwiatkowski GM, Millis SR, Purakal JD, Mahajan AP, Levy PD. Use of nitroglycerin by bolus prevents intensive care unit admission in patients with acute hypertensive heart failure. Am J Emerg Med. 2017 Jan;35(1):126-131. doi: 10.1016/j.ajem.2016.10.038. Epub 2016 Oct 18. PMID: 27825693.
Mathew R, Kumar A, Sahu A, Wali S, Aggarwal P. High-Dose Nitroglycerin Bolus for Sympathetic Crashing Acute Pulmonary Edema: A Prospective Observational Pilot Study. J Emerg Med. 2021 Sep;61(3):271-277. doi: 10.1016/j.jemermed.2021.05.011. Epub 2021 Jun 30. PMID: 34215472.
Wilson SS, Kwiatkowski GM, Millis SR, Purakal JD, Mahajan AP, Levy PD. Use of nitroglycerin by bolus prevents intensive care unit admission in patients with acute hypertensive heart failure. Am J Emerg Med. 2017 Jan;35(1):126-131. doi: 10.1016/j.ajem.2016.10.038. Epub 2016 Oct 18. PMID: 27825693.
Paone S, Clarkson L, Sin B, Punnapuzha S. Recognition of Sympathetic Crashing Acute Pulmonary Edema (SCAPE) and use of high-dose nitroglycerin infusion. Am J Emerg Med. 2018 Aug;36(8):1526.e5-1526.e7. doi: 10.1016/j.ajem.2018.05.013. Epub 2018 May 10. PMID: 29776826.
Category: Trauma
Keywords: substance abuse, alcohol abuse, SBIRT, intervention, FACS (PubMed Search)
Posted: 2/10/2023 by Robert Flint, MD
Click here to contact Robert Flint, MD
In December 2022, The American College of Surgeons released a practice guidine discussing screening trauma patients for mental health disorders and substance use disorders. There is a very high likelihood that your acute trauma patient has a pre-existing disorder.
"Over 50% of hospitalized trauma patients report an alcohol and/or drug use diagnosis during their lifetime. At the time of admission, one in four trauma victims meet diagnostic criteria for an active alcohol use problem and 18% meet diagnostic criteria for a drug use problem".
Screening, Brief Intervention and Referal to Treatment (SBIRT) programs have a major impact on injury recidivism and future mortality. Trauma patients should be screened for mental health disorders and substance use disorders.
BEST PRACTICES GUIDELINES SCREENING AND INTERVENTION FOR MENTAL HEALTH DISORDERS AND SUBSTANCE USE AND MISUSE IN THE ACUTE TRAUMA PATIENT American College of Surgeons December 2022
https://www.facs.org/media/nrcj31ku/mental-health-guidelines.pdf
Category: Orthopedics
Keywords: concussion recovery, head injury, post concussive syndrome (PubMed Search)
Posted: 2/11/2023 by Brian Corwell, MD
(Updated: 6/18/2026)
Click here to contact Brian Corwell, MD
Prolonged post-concussion symptoms are loosely defined as those lasting more than three or four weeks versus typical recovery, typically between 10-14 days.
Athletes who take longer than "typical” to recover have a challenging road of uncertainty. Medical providers are asked to make informed decisions about “normal” and expected return based on limited information.
Evaluating both athlete and parental expectations is challenging, especially when navigating difficult conversations about medical disqualification and permanently discontinuing their sport.
A 2016 study of approximately 50 patients with sports-associated concussion who had persistent symptoms lasting greater than one-month found that a collaborative multidisciplinary treatment approach was associated with significant reduction in post concussive symptoms at six months versus usual treatment.
A recent 2023 study in Neurology provides additional good news for athletes who are slow to recover from sports associated concussion. Approximately 1750 concussed collegiate athletes (diagnosed by team physician) were enrolled. In this study, slow recovery was defined as taking more than 14 days for symptoms to resolve OR taking more than 24 days to return to sport.
Approximately 400 athletes met the criteria for slow recovery (23%).
Male athletes participated primarily in football, soccer, and basketball.
Female athletes participated primarily in soccer, basketball, and volleyball.
Of the athletes who took longer than 24 days to return to play:
77.6% were able to return to play within 60 days of injury,
83.4% returned to play within 90 days, and
10.6% did not return to play at 6 months.
Slow to recover athletes averaged 35 days after injury for return to play.
This study provides valuable information for medical providers: There is an overall favorable prognosis for slow to recover concussed athletes for return to school and sport.
McAllister TW,et al; Concussion Assessment, Research and Education (CARE) Consortium. Characteristics and Outcomes of Athletes With Slow Recovery From Sport-Related Concussion: A CARE Consortium Study. Neurology. 2023 Jan 18:10.1212
Category: Critical Care
Keywords: sodium bicarbonate, bicarb, OHCA, cardiac arrest, CPR, resuscitation (PubMed Search)
Posted: 2/8/2023 by Kami Windsor, MD
Click here to contact Kami Windsor, MD
Background: The use of sodium bicarbonate in the treatment of out-of-hospital cardiac arrest (OHCA) has been longstanding despite conflicting data regarding its benefit, outside of clear indications such as toxic ingestion or hyperkalemic arrest.
Study: A recent retrospective cross-sectional study by Niederberger et al.1 examined prehospital EHR data for ALS units responding to nonpregnant adults with nontraumatic OHCA, noting use of prehospital bicarb and the outcomes of 1) ROSC in the prehospital encounter and 2) survival to hospital discharge. They created propensity-matched pairs of bicarb and control patients, with a priori confounders: age, sex, race, witnessed status, bystander CPR, prearrival instructions, any defibrillation attempt, use of CPR feedback devices, any attempted ventilation, length of resuscitation, number of epi doses.
There were 23,567 arrests (67.4% asystole, 16.6% PEA, 15.1% VT/VF), 28.3% overall received sodium bicarb.
Results:
In the propensity-matched sample, survival was higher in bicarb group (5.3% vs. 4.3%; p=0.019).
There were no differences in rate of ROSC overall, but looking at the different rhythms, ROSC was higher in the bicarb group with asystole as the presenting rhythm (bicarb 10.6 vs 8.8%; p=0.013) but not PEA or VT/VF.
*There is no indication by the authors as to the dosing of bicarb most associated with survival to hospital discharge (or ROSC in asystole) in the study, however a previous study has indicated that a single amp of bicarb is unlikely to significantly improve severe metabolic acidosis (pH <7.1),2 so the general recommendation of at least 1-2mEq/kg should be employed.
Bottom Line: The use of sodium bicarb may increase survival in OHCA with initial PEA/asystole. The recommended initial dose is 1-2mEq/kg; giving at least 2 amps of bicarb (rather than the standard 1) should achieve this in many patients.
Between 1/2019 and 12/2020, there were 23,567 arrests that met inclusion criteria.
Overall EMS ROSC: 18.4%
Overall survival to hospital discharge: 7.6%
In the propensity-matched sample – survival was higher in bicarb group (5.3% vs. 4.3%; p=0.019).
There were no differences in rate of ROSC overall, but looking at the different rhythms, ROSC was higher in the bicarb group with asystole as the presenting rhythm (bicarb 10.6 vs 8.8%; p=0.013) but not PEA or VT/VF.
Overall, bicarb use was associated with improved survival (OR 1.25 (1.04-1.51) / aOR 1.3 (1.06-1.59) but not increased ROSC.
Category: Trauma
Keywords: penetrating neck trauma, zones, hard signs, operative management (PubMed Search)
Posted: 2/5/2023 by Robert Flint, MD
Click here to contact Robert Flint, MD
The classic teaching regarding penetrating neck trauma is violation of the platysma muscle in zones 1 and 3 requires angiography, endoscopy and bronchoscopy. Injury to zone 2 is an automatic operative evaluation. Now, more anatomic and physiologic signs dictate operative management and those not meeting these hard signs get evaluated with Ct angiography.
Neck zones and hard vs soft signs available by clicking link
| Zone | Boundaries | Structures |
|---|---|---|
| I (lower) | Clavicles and sternum to the cricoid cartilage | Vascular: subclavian arteries and veins, jugular veins, carotid arteries, vertebral arteryAerodigestive: lungs, trachea, esophagusNeurologic: spinal cord, vagus nerveOther: thoracic duct, thyroid gland |
| II (middle) | Cricoid cartilage to the angle of the mandible | Vascular: common/internal/external carotid arteries, vertebral arteries, jugular veinsAerodigestive: trachea, larynx, pharynx, esophagusNeurologic: spinal cord, vagus nerve, recurrent laryngeal nerve |
| III (upper) | Angle of the mandible to the base of the skull | Vascular: internal carotid arteries, vertebral arteries, jugular veinsAerodigestive: pharynxNeurologic: spinal cord, CN IX, X, XI, XI, sympathetic chainOther: salivary glands |
Hard SignsVascular injury
Severe uncontrolled hemorrhage
Refractory shock/hypotension
Large, expanding, or pulsatile hematoma
Unilateral extremity pulse deficit
Bruit or thrill
Neurologic deficit consistent with strokeMinor bleeding
Soft Signs Vascular
Small, nonexpanding hematoma
Proximity wound
Hard SignsAerodigestive tract injuryAirway compromise
Bubbling through wound
Extensive subcutaneous emphysema
Stridor
Hoarse voice
Soft Signs
Mild hemoptysis
Mild hematemesis
Dysphonia
Dysphagia
Mild subcutaneous emphysema
Protect That Neck! Management of Blunt and Penetrating Neck Trauma
Matt Piaseczny, MD, MSc Julie La, MD, MESc Tim Chaplin, MD Chris Evans, MD :https://doi.org/10.1016/j.emc.2022.09.005
Category: Pharmacology & Therapeutics
Keywords: Angioedema, ACE-inhibitor, C1-Esterase Inhibitor, ACEi, C1INH, Berinert (PubMed Search)
Posted: 2/3/2023 by Wesley Oliver
(Updated: 2/4/2023)
Click here to contact Wesley Oliver
ACE-inhibitor (ACEi) induced angioedema is mediated by bradykinin and there are no proven medications for the treatment of this disease. Theoretically, a C1-esterase inhibitor (C1INH) could be beneficial; however, data has not demonstrated any efficacy for these agents.
Strassen et al. recently published a double-blind, randomized, controlled, multicenter trial of 30 patients comparing C1NH (Brand Name: Berinert) to placebo. In addition to standard treatment, a dose of C1INH (Berinert) 20 IU/kg or placebo (0.95% NaCl) was administered intravenously.
The primary endpoint was the time to complete resolution of signs and symptoms of edema (TCER). When compared to placebo, the original primary analysis demonstrated that the placebo arm (15 hours) resolved faster than the C1INH arm (24 hours, p=0.046).
This study is further evidence against the use of C1INH for ACE-inhibitor induced angioedema. The primary focus in the treatment of ACEi induced angioedema should continue to be airway management.
For reference, at our institution we have both C1INH (Berinert) and icatibant on formulary and they are restricted to only being used for acute hereditary angioedema attacks and cannot be used for ACEi induced angioedema.
Strassen U, et al. Efficacy of human C1 esterase inhibitor concentrate for treatment of ACE-inhibitor induced angioedema. Am J Emerg Med. 2023;64:121-128.
Wilkerson RG, Martinelli AN, Oliver WD. Treatment of angioedema induced by angiotensin-converting enzyme inhibitor [letter]. J Emerg Med. 2018;55:132-133.
Category: Pediatrics
Keywords: otitis media, antibiotic (PubMed Search)
Posted: 2/3/2023 by Rachel Wiltjer, DO
Click here to contact Rachel Wiltjer, DO
Otitis media is a common pediatric complaint seen in the primary care, urgent care, and ED settings. Recommendations for timing of treatment and deferral of treatment have emerged over the last several years, as have recommendations for regimens for recurrent infections in the age of resistant organisms.
When to consider observation over antibiotics:
Initial treatment
High dose amoxicillin (90 mg/kg/day divided BID)
Recurrent Otitis Media
If less than 30 days from initial treatment, presumed to be persistent
If greater than 30 days from initial treatment can treat as new episode (so amoxicillin unless previous documented resistant infections)
Duration of Antibiotics
Other Considerations
Gaddey HL, Wright MT, Nelson TN. Otitis Media: Rapid Evidence Review. Am Fam Physician. 2019;100(6):350-356.
Rosenfeld RM, Tunkel DE, Schwartz SR, et al. Clinical Practice Guideline: Tympanostomy Tubes in Children (Update). Otolaryngol Head Neck Surg. 2022;166(1_suppl):S1-S55. doi:10.1177/01945998211065662
{kind=link}
{kind=link}
{kind=link}