Reversal of the new anticoagulants rivaroxaban (Xarelto) and dabigatran (Pradaxa) has been challenging particularly in the ED setting with no definitive reversal agent. Intracerebral hemorrhage or critical GI bleed management becomes challenging and worsens mortality.
There is growing literature that states activated prothrombin complex concentrate or non-activated PCC may reverse these new anticoagulants. A volunteer study (1) showed its efficacy and concensus workgroups are now recommending aPCC as first line therapy(2). The search goes on for a reliable reversal agent for these new anticoagulants which were suppose to solve more problems instead of create new ones.
General Information:
Nisseria meningitidis is the common culprit in epidemic meningitis. Serogroup B is currently causing an outbreak on the Princeton campus. So what are the serogroups and why are they important?
Six main serogroups cause disease: A, B, C, Y, X, W-135.
Two quadrivalent vaccines are currently licensed in the US that cover Serogroups A, C, Y, and W-135.
Relevance to the EM Physician: The currently available vaccines in the US cover the majority of serogroups of meningococcus, however, Serogroup B (currently causing an outbreak at Princeton) is not covered, nor is Serogroup X (for travelers to Sub-Saharan Africa).
Bottom Line: Serogroups B and X are not covered by the currently available vaccines in the US and at risk populations (and physicians treating those patients) should be made aware of the gap in coverage. Investigations for a vaccine for Serogroup B (licensed in Europe and Australia, but not in the US) are currently underway.
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH, FACEP
Ottawa Rules for Subarachnoid Hemmorhage (SAH)
Background
Design
Results
132 (6.2%) had SAH
Decision rule including any:
Had 98.5% sensitivity (95% CI, 94.6%-99.6%) and 27.5% specificity (95% CI, 25.6%-29.5%)
Adding “thunder-clap” headache and “limited neck flexion on examination” (inability to touch chin to chest or raise the head 8cm off the bed if supine) resulted in 100% (95% CI, 97.2%-100%) sensitivity.
The rule was then evaluated using a bootstrap analysis on old cohort data to validate the rule.
Conclusion/Limitations
For alert patients older than 15 y with new severe nontraumatic headache reaching maximum intensity within 1 h
Not for patients with new neurologic deficits, previous aneurysms, SAH, brain tumors, or history of recurrent headaches (≥3 episodes over the course of ≥6 mo)
Investigate if ≥1 high-risk variables present:
Age ≥40 y
Neck pain or stiffness
Witnessed loss of consciousness
Onset during exertion
Thunderclap headache (instantly peaking pain)
Limited neck flexion on examination
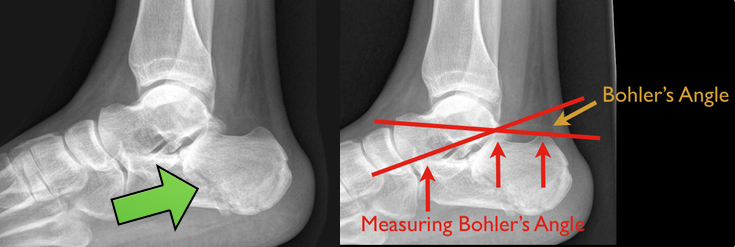
48 year-old presents after falling 15 feet following a “misunderstanding” with police. What's the diagnosis? ...and for a bonus question, why is this called a “Lover’s Fracture”?

Utility of Intra-Aortic Balloon Pump (IABP)
Compartment Syndrome
Compartment syndrome is classically described as having the 6 Ps:
The diagnosis of compartment syndrome can be difficult but ultimately it comes down to measuring the pressures in the area of concern. Various recommendations of the allowed pressure can be found, but in general a fasciotomy is not needed if the compartment pressure is 30 mmHg less then the diastolic pressure (The Delta 30). So if the patients diastolic pressure is 70, a fasciotomy is not need if the compartment pressure is less then 40.
Finally, if you are suspecting compartment pressure do NOT elevate the limb. Leave it in a dependent position to help improve blood flow into the limb.
Case: A 3 year 9 month female presents with fever to 39.4 C and intermittent abdominal pain worsening over 2 days. The patient had been tolerating food and had no change in her bowel habits. Based on the imaging below, what is your diagnosis and treatment?
All benzodiazepines are metabolized by the liver. Some are just metabolized by pathways that are less dependent on global liver function.
The ‘LOT’ drugs are metabolized by conjugation, have no active metabolites, and have minimially affected half-lives even in the setting of liver disease.
L – Lorazepam
O – Oxazepam
T – Temazepam
The rest of the benzodiazepines are primarily metabolized via hepatic CYP-mediated oxidation and may have prolonged duration of effect in patients with marked liver impairment.
For a bit more detail and commentary by Dr. David Juurlink, please read my recent post on the Academic Life in Emergency Medicine blog: http://academiclifeinem.com/all-benzodiazepines-are-metabolized-by-the-liver/
Helicopter EMS (HEMS) has rapidly grown over the past 30 years. HEMS is frequently used to transport trauma patients from the scene of a crash. The question is: for which trauma patients is HEMS most useful?
A recent article published in the Journal of the American Medical Association, based upon data from the National Trauma Data Bank (NTDB), looked at injured patients transported to a trauma center by helicopter versus ground ambulance. It showed that, after controlling for multiple known confounders, more severely injured patients had better outcomes when transported by helicopter than when transported by ground ambulances. Another recent article in the Journal of Trauma and Acute Care Surgery, again based upon the NTDB further showed that HEMS survival benefit seems to limited to individuals with physiologic instability.
Bottom Line:
Transport of severely injured trauma patients by helicopter versus ground from the scene of injury to a trauma center improved patient outcomes and decreased mortality. Transportation of stable, less injured patients by helicopter may actually worsen outcomes.
University of Maryland Section of Global Emergency Health
Author: Jon Mark Hirshon
Acalculous Cholecystitis in the Critically Ill
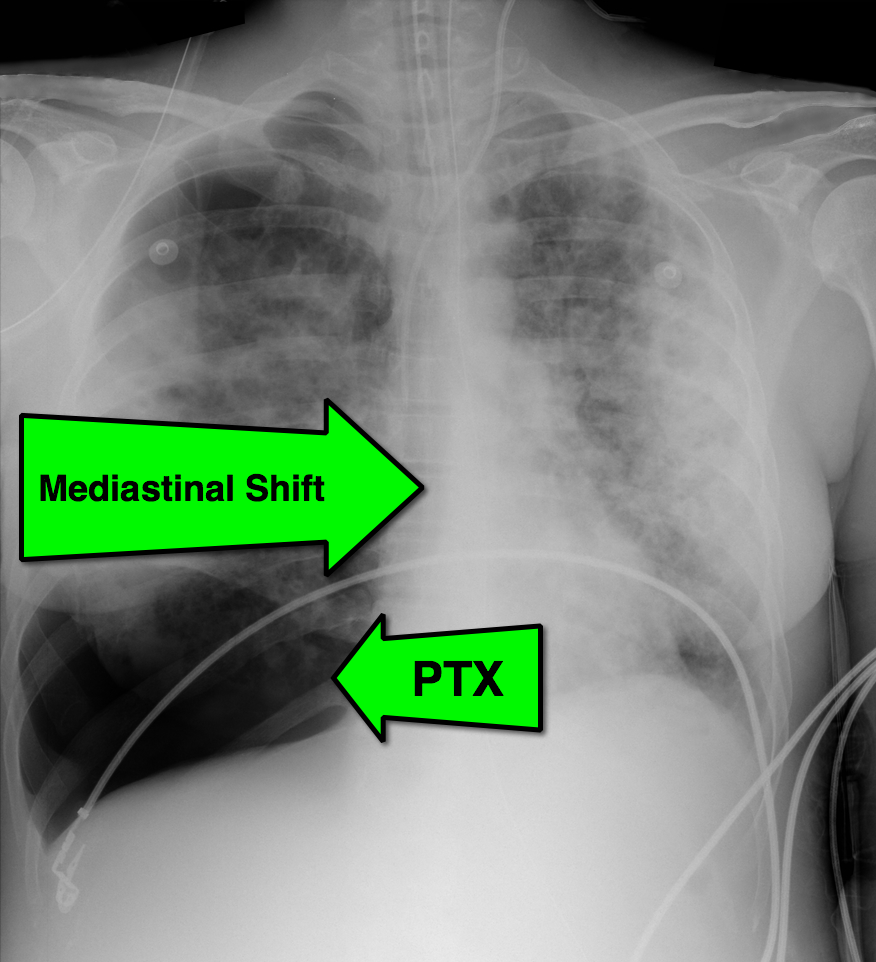
28 year-old cachectic female presents in respiratory distress and is immediately intubated on arrival to Emergency Department. What's the diagnosis and what are some potential etiologies?

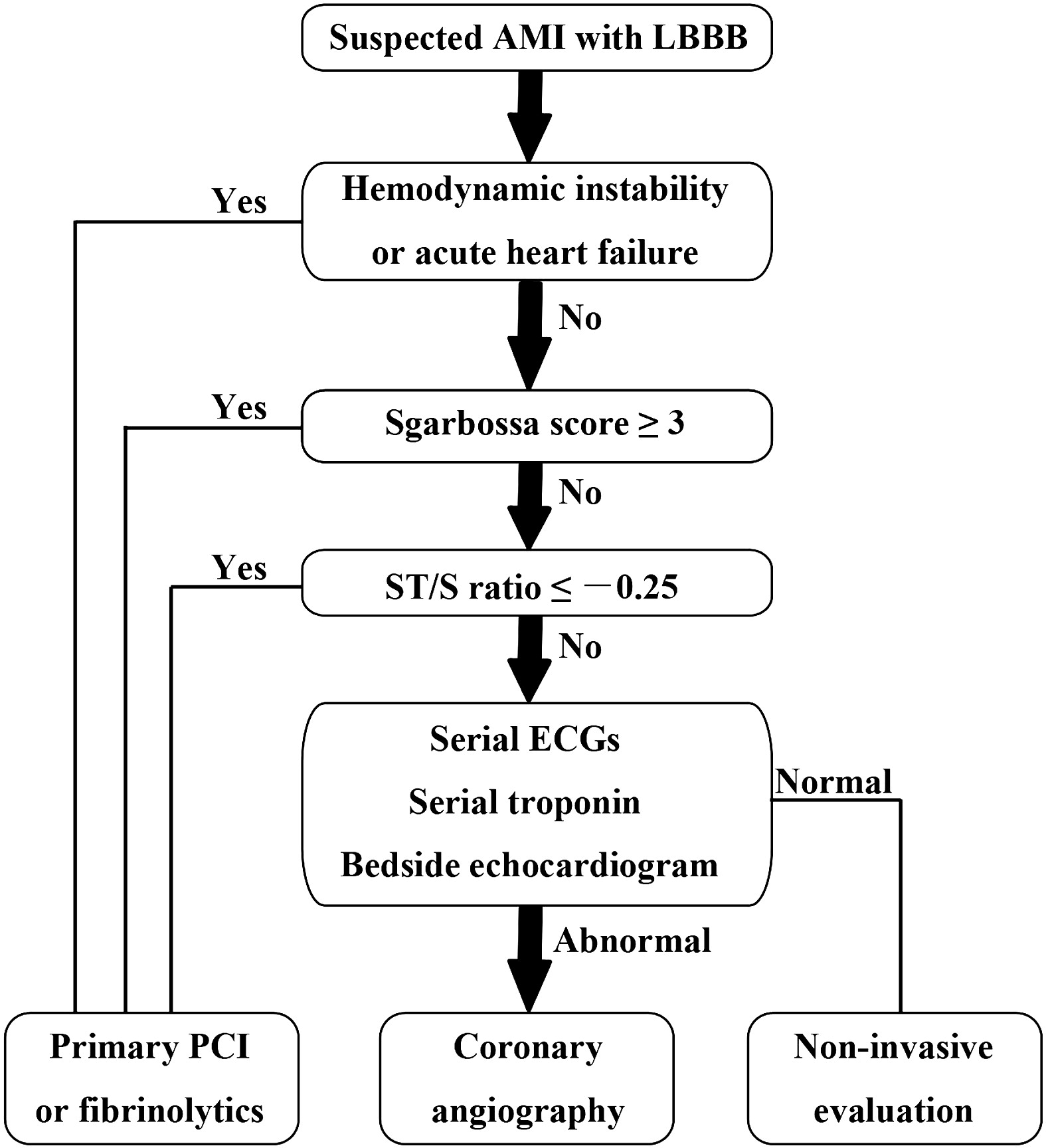
Diagnosis of STEMI in patients with LBBB can be challenging. Guidelines that previously recommended emergent reperfusion for these patients have been reconsidered to avoid inappropriate cath lab activation and fibrinolytic therapy.
The 2013 ACC/AHA STEMI guidelines no longer consider new or presumably new LBBB a STEMI equivalent. This dramatic change may prevent inappropriate therapy for some, but fail to help identify patients with LBBB who are having STEMI's. Delayed reperfusion in this population could be fatal and is estimated to affect 5,000-10,000 patients per year in the US alone.
The Sgarbossa ECG criteria are the most validated tool to aid in the diagnosis of STEMI in the presence of LBBB. A Sgarbossa score of ≥ 3 has high specificity (>98%) and positive predictive value for acute MI and angiography-confirmed coronary occlusion. The following algorithm has been recently proposed to identify the high-risk population in which reperfusion therapy would be denied by the 2013 STEMI guidelines.
Watch this video to review Sgarbossa criteria and the modified Sgarbossa rule.
Want more emergency cardiology pearls? Follow me @alifarzadmd
Cauda equina syndrome results from compression of multiple lumbar and sacral nerve roots
Causes: Central disc herniation, spinal epidural abscess, malignancy, trauma, hematoma.
Consider this entity in those with back pain and radiculopathy at multiple spinal levels
Urinary retention occurs in >90% of patients
Saddle anesthesia occurs in 75%
Decreased rectal sphincter tone occurs in 60 to 80%
A post void residual volume <100 mL makes this entity very unlikely
When patients with severe allergies to penicillin (urticarial, bronchospasm, anaphylaxis, angioedema) are excluded, the cross reactivity to cephalosporins is very low (approximately 0.1%)
The reaction is related to structures in the side chain, not the cyclical structure as thought in the past.
There are several cephalosporins with IDENTICAL side chains that should not be given to patients with allergies to specific penicillins, namely:
Case Presentation:
A 56y/o man with diabetes presents with fever, cough, and diarrhea x 2 days.
V/S: T:38.7 BP:165/88 P: 105 R:24 O2 sat:91% on room air
CXR: left lower lobe infiltrate.
On further history you learn he has just returned from visiting family in Saudi Arabia 7 days ago. While there, he visited a cousin that was ill.
Clinical Question:
Should this patient be isolated for Middle Eastern Respiratory Syndrome – Corona Virus (MERS-CoV)?
Answer:
Yes, there are 150 cases to date and 64 have died. None confirmed in the US yet but 6 confirmed in Europe.
Patients who should be isolated in an airborne iso room with N95 mask use (similar to TB) are:
Patients with fever + pneumonia/ARDS AND one of the following:
Bottom Line:
In patients with febrile respiratory illness requiring hospitalization and recent travel to the Arabian Peninsula: isolate for MERS-CoV and contact the health department.
University of Maryland Section of Global Emergency Health
Author: Jenny Reifel Saltzberg
Ineffective triggering is the most common type of ventilator dyssynchrony. The differential diagnosis includes:
Auto peep is the most common cause of ineffective triggering and will often occur as a patient cannot create enough inspiratory force to overcome their own intrinsic peep (PEEPi). Patients who are severely tachypnic or those with obstructive lung disease are at high risk for auto peep (not enough time to exhale).
Ineffective triggering can also occur if the patient cannot create enough of a negative inspiratory force to trigger the vent to deliver a positive pressure breath. Prolonged period of mechanical ventilation, over sedation, high cervical spine injuries, or diaphragmatic weakness are common causes.
Lastly, improper trigger sensitivities may make it difficulty for the ventilator to sense when the patient is attempting to take a spontaneous breath.
For an example of a patient with ineffective triggering, check out: http://marylandccproject.org/2013/10/28/vent-problems1/
This week's visual pearl reviews the structures of the heart when being viewed in a parasternal long-axis view. What do the labels correspond to in the clip below (note: "E" and "F" are valves) and do you see any obvious abnormalities?
Secondary Prevention in AMI
Just as aspirin is pivotal in the treatment of acute coronary syndrome, medications such as beta-blocker, statins, and angiotensin-converting enzyme inhibitors have been proven to be essential in secondary prevention of AMI.
Patients after AMI are typically discharged on appropriate secondary prevention medications; however the prescribed doses are often far below the proven efficacy based on clinical trials.
A review of 6,748 patients from 31 hospitals enrolled in 2 U.S. registries (2003 to 2008) illustrated that only 1 in 3 patients were prescribed these medications at goal doses.
Of patients not discharged on goal doses, up-titration during follow-up occurred infrequently ~25%.
Optimal medication dosing and appropriate titration is integral to prevention of further morbidity and mortality.
A recent meta-analysis has called into question whether contrast-induced AKI even occurs after an IV dye load for radiologic imaging. [1] This conclusion is most certainly up for debate.
Irrespective of that conclusion, prevention of contrast-induced nephropathy is still important. Is there any benefit to using N-acetylcysteine over normal saline in the ED? Probably not according to a new study. [2]
Conclusions