Tight glycemic control (HbA1C<7%) has previously been recommended in CAD based on data from the United Kingdom Prospective Diabetes Study (UKPDS)
A recent study (JACC) evaluated the relationship between glycemic control, cardiovascular disease (CVD) risk, and all-cause mortality
Patients with a mean HbA1C 7-7.4% were compared to those with mean HbA1C <6%; tight glycemic control had a 68% increased risk of CVD hospitalization
Lenient HbA1C>8.5% also had significantly higher risk
CVD risk and all-cause mortality is greater with both aggressive and lax glycemic control and the optimal reference range may lie between 7-7.4%
Dupuytren disease is a nodular thickening and resultant contraction of the palmer fascia.
Increased in those of Northern European dissent.
One or more painful nodules located near the distal palmer crease.
Over time may result in flexion at the MCP joint.
Most commonly affects the ring finger.
Sensation is normal.
Over time affects ADLs
Tx: night splints and surgery
Cringing at the thought of sewing up another screaming 2 year old?
Consider intranasal fentanyl.
Who: Young, otherwise healthy pediatric patients undergoing minor procedures (laceration repair, fracture reduction/splinting, etc...)
What: Fentanyl (2mcg/kg)
When: 5 minutes pre-procedure
Where: Intranasal
Why: More effective than PO, less invasive than IV while being equally efficacious.
How: Use an atomizer, splitting the dose between each nostril.
General Information:
· Caused by the ameboflagellate Naegleria Fowleri
· Case fatality rate is estimated at 98%
· Commonly found in warm freshwater environments such as hot springs, lakes, natural mineral water, especially during hot summer months
· Incubation period 2-15 days
Relevance to the EM Physician:
· Clinical presentation: resembling bacterial meningitis/encephalitis
· Final diagnostic confirmation is not achieved until trophozoites are isolated and identified from CSF or brain tissue
· Treatment: Amphotericin B
Bottom Line:
· History of travel to tropical areas or exposure to warm or under-chlorinated water during summer time should raise the suspicion for Naegleria Fowleri. The amoeba is not sensitive to the standard meningitis/encephalitis therapy and amphotericin B must be added to the treatment regimen.
University of Maryland Section of Global Emergency Health
HIV, ART, and the ICU
A 3 year-old boy was attacked by a dog and sustained the injury below. Name one injury that should be strongly considered (Hint: there are several)

Treatment of Severe Hypothyroidism
We do not see patient's with severe hypothyroidism often, but it is important that they be treated aggressively. Some treatment pearls are
Lactate is commonly used in the adult ED when evaluating septic patients, but there is a lack of literature validating its use in the pediatric ED. Pediatric studies have suggested that in the ICU population, elevated lactate is a predictor of mortality and may be the earliest marker of death.
A retrospective chart review over a 1 year period showed that one elevated serum lactate correlated with increased pulse, respiratory rate, white blood cell count and platelets. Serum lactate had a negative correlation with BUN, serum bicarbinate and age. Elevated lactate levels were higher for admitted patients. However, the mean serum lacate level was not statistically different between those diagnosed with sepsis and those that were not.
The study included 289 patients less then 18 years who had both blood cultures and lactate drawn. This community hospital had a sepsis protocol in place that automatically ordered a lactate with blood cultures. Only previously healthy children were included.
The study is limited by its small sample size and overall low lactate levels. Despite having a protocol in place, only 39% of patients who had blood cultures drawn had lactate levels available for analysis. The mean serum lacate in this study was 2.04 mM indicating that the study population may not have been sick enough to determine mortality implications. There were no serial measurements.
Bottom line: Consider measuring serum lacate in your pediatric patient with suspected sepsis. Pediatric ICU literature does suggest that an serum lactate as low as 3mM is associated with an increased mortality in the ICU.
The internet has become a wealth of information and some books have now gained internet noteriety. A chemist and author of the book - TIKHAL: Tryptamines I Have Known and Loved is an excellent example.
Tryptamines include drugs like LSD and alpha-methyltryptamine (AMT). Vivid visual hallucinations and serotonin agonism, these drugs were glamorized by this author. He would synthesize a tryptamine and then "taste it". Take a look at the link below where he first describes the biochemical synthesis he performed then describes his dose response effect when he tried the drug.
If you run into a drug or slang term in the ED you are not familiar with, the website www.erowid.org will likely have the translation.
http://www.erowid.org/library/books_online/tihkal/tihkal48.shtml
COPD treatment guidelines (e.g., GOLD) recommend 10-14 days of steroid therapy following a COPD exacerbation to prevent recurrences; the supporting data is weak.
A recent noninferiority trial (here) compared patients with a severe COPD exacerbation who received either a 5-day course (n=156) or 14-day course (n=155) of prednisone 40mg.
The results were:
What you need to know:
Bottom-line: 5 days of prednisone may be as effective as 14-days for COPD exacerbations.
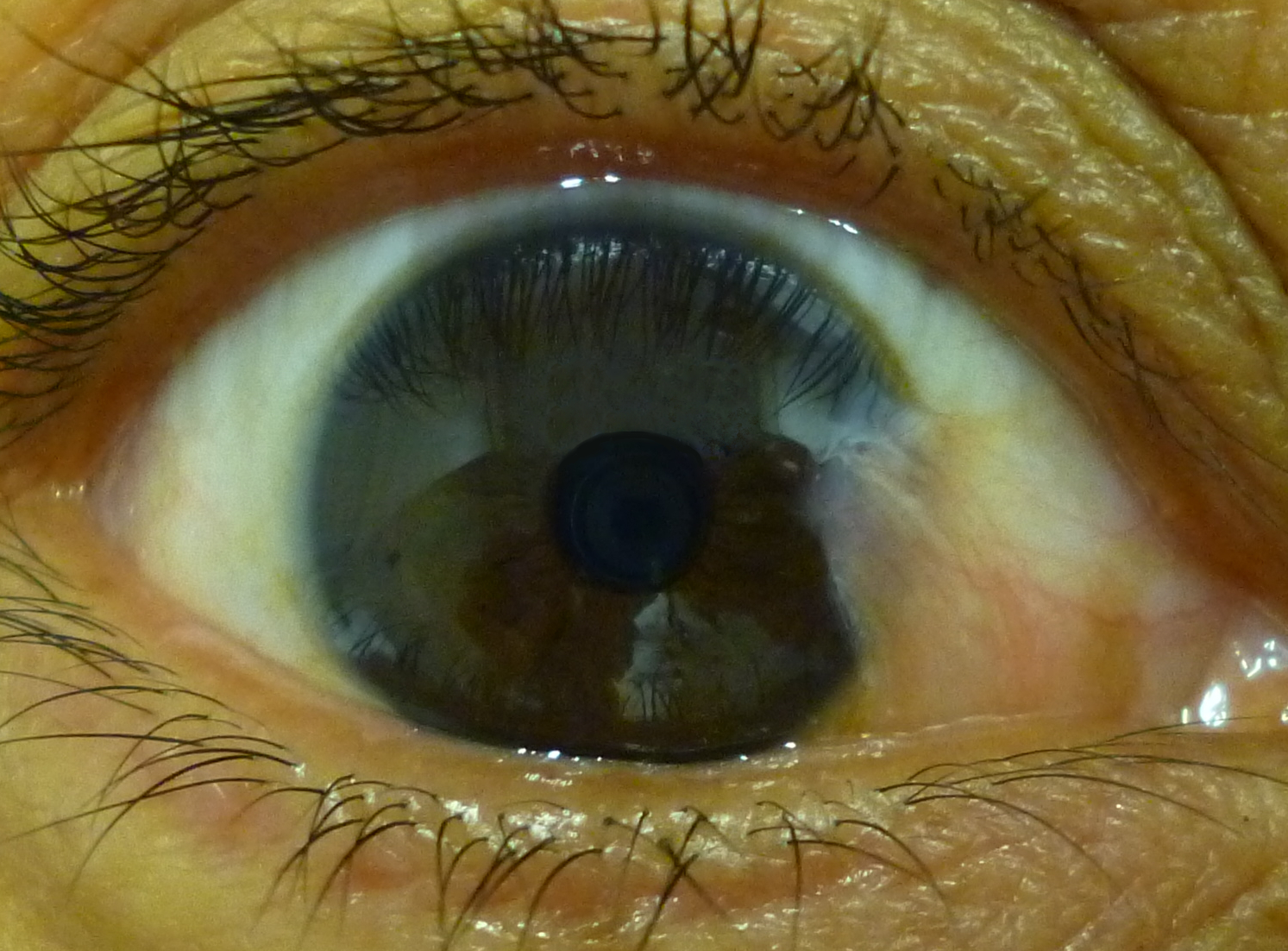
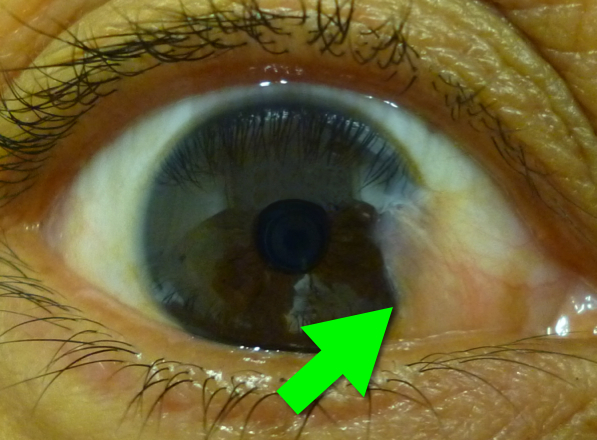
46 year-old female presents with a headache. The following is seen on visual inspection of the eye. What's the diagnosis?
Radiation therapy is frequently utilized in the management of numerous thoracic malignancies
Cardiovascular disease is now the leading cause of nonmalignancy death in radiation-treated cancer survivors
The spectrum of radiation-induced cardiac disease is broad
The relative risk of CAD, CHF, pericardial/valvular disease, and conduction abnormalities is particularly increased
Early identification of potential cardiac complications w/cardiac MR and echocardiography provides an opportunity for regular assessment and potentially improved long term mortality
Tests for distal ulnar nerve entrapment
Ask patient to hold a piece of paper between the thumb and the index finger
Normally this is a fairly simple task.
With an unlar nerve palsy, the patient will substitute with the FPL (flexor pollicis longus - median nerve innervation). This causes flexion of the thumb in order to maintain the grip since the adductor pollicis cannot be used. This causes thumb flexion rather than extension.
http://www.mims.com/resources/drugs/common/CP0042.gif
http://www.youtube.com/watch?v=yJTIhm1VfSI
Risk stratisfication score introducted by Maden Samuel in 2002.
The Pediatric Appendicitis Score had a sensitivity of 1, speciificity of 0.92, positive predictive value of 0.96, and negative predictive value of 0.99
Signs:
Symptoms:
Laboratory Values:
Scores of 4 or less are least likely to have acute appendicitis, while scores of 8 or more are most likely.
In June 2013 the American College of Medical Toxicology (ACMT) released a Guidance Document on the Management Priorities in Salicylate Toxicity. Here are some key highlights:
The full document can be accessed here.
The Poison Review blog by Dr. Leon Gussow discusses the guidance document here.
Follow me on Twitter (@PharmERToxGuy)
3 year-old male develops rash 5 days after starting amoxicillin for acute otitis media. What's the diagnosis?

A recent, randomized study evaluated two approaches for treating acute pain in an inner-city ED.
Application to clinical practice: For most patients with acute, severe pain in the ED, start with hydromorphone 1 mg. It may be all the patient needs and can potentially avoid giving them extra opioid they don't need.

{kind=link}