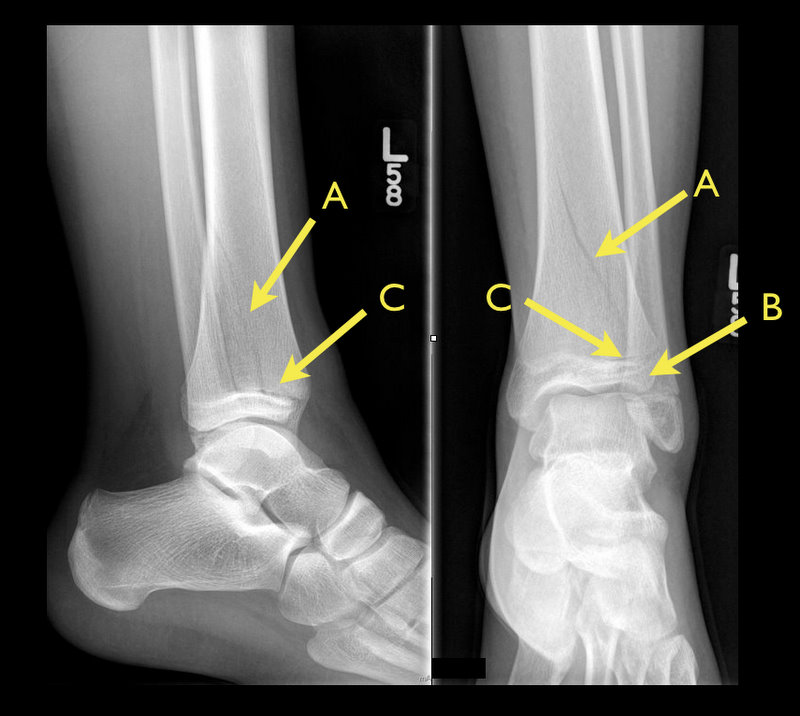
13 year-old female with ankle pain following fall down escalator. What's the diagnosis?

The adolescent brain has not yet reached full maturation and is in a period of rapid development from ages 14 - 16.
Adolescents have been found to be more sensitive to the effects of concussion than adults
Concussed adolescents have deficits in attention and executive function lasting up to 2 months post injury.
Be aware that the adolescent brain will require extended recuperation time following injury
In the future, discharge instructions might need to say more than "don't get hit in the head till your headache goes away." Because of deficits in attention and executive function, physicians should consider recommendations about adolescents and jobs, school work and driving an automobile.
Infant lumbar puncture is often difficut and may require repeated attempts. The traditional body positioning is lateral decubitus. Previous studies have examined the saftey of having the patient in a sitting position, and neonatal studies have suggested that the subarachnoid space increases in size as the patient is moved to the seated position. A study by Lo et al published last month looked to see if the same held true in infants.
50 healthy infants less then 4 months old had the subarachnoid space measured by ultrasound between L3-L4 in 3 positions: lateral decubitus, 45 degree tilt and sitting upright.
This study found that the size of the subarachnoid space did not differ significantly between the 3 positions. Authors postulated that a reason for increase sitting LP success rate that had been reported in anestesia literature with tilt position could be due to other factors such as increased CSF pressure, intraspinous space widening or improved landmark identification.
General Information:
-The global health world is faced with an unprecedented challenge of a trio of threats:
1. Infections, undernutrition, reproductive health issues
2. Rising global burden of non-communicable diseases and risk factors
3. Challenges arising from globalization (climate change and trade politics)
-Definitions of global health are variable and can emphasize anything from types of health problems, populations of interest, geographic area or a specific mission. This makes governance and analysis difficult.
-During the past decade there has been an explosion of more than 175 initiatives, funds, agencies, and donors. Health is increasingly influenced by decisions made in other global policymaking areas.
-The major governance challenges for global health are:
1. Defining national sovereignty in the context of deepening health interdependence
2. Maximizing cross-sector interdependence
3. Developing clear mechanisms of accountability for non-state actors
Relevance to the US physician:
The Global Health System and its governance affects our ability to work effectively within the US and how we structure efforts to expand the reach of timely, effective emergency care worldwide.
Bottom Line:
The Global Health System has become more complex. Any development of Emergency Care Systems must take into account the complexity of actors in the field of global health.
The University of Maryland Section of Global Emergency Health
Author: Emilie J. B. Calvello, MD, MPH
Therapeutic hypothermia (TH) following out-of-hospital cardiac arrest (OHCA) has increasingly been utilized since it was first described. TH following in-hospital cardiac arrest (IHCA), on the other hand, is not as commonplace or consistent despite a recommendation by the American Heart Association (AHA).
A recent prospective multi-center cohort-study demonstrated that of 67,498 patients with return of spontaneous circulation (ROSC) following IHCA only 2.0% of patients had TH initiated; of those 44.3% did not even achieve the target temperature (32-34 Celsius).
The factors found to be most associated with instituting TH were:
Bottom-line: Hospitals should consider instituting and adhering to local TH protocols for in-house cardiac arrests.
Ever wonder how to place a pigtail catheter?
Check out this video to learn how, click here
Background
In the current era of community-acquired MRSA (CA-MRSA), most of our outpatient treatment options for cellulitis aim to cover MRSA. Choices include sulfamethoxazole/trimethoprim (SMZ-TMP), doxycycline, linezolid, and clindamycin (depending on local susceptibility patterns).
A New Study
Take Home Clinical Points
Hyperglycemia in the setting of antipsychotic use has been reported mostly with olanzapine (Zyprexa) but does occur with other antipsychotics. A recent study from the NYC medical examiner's office details 17 deaths of DKA due to antipsychotics and found that (from highest to lowest incidence) quetiapine > olanzapine > risperidone were the atypical antipsychotics found with these deaths.
Remember hyperglycemia occurs with patients on antipsychotics and can lead to hyperglycemia hyperosmolar coma or DKA. Both can be lethal.
Background Information:
Each year, an estimated 50 million travelers from Western countries visit tropical regions all over the world.
Given the potentially serious consequences for the patients and, their close contacts and healthcare workers it is important that life threatening tropical diseases are swiftly diagnosed.
Pertinent Study Design and Conclusions:
- Descriptive analysis of acute and potentially life threatening tropical diseases among 82,825 ill western travelers reported to GeoSentinel from June of 1996 to August of 2011.
- Of these travelers, 3,655 (4.4%) patients had an acute and potentially life threatening disease.
- The four most common conditions being falciparum malaria (76.9%), typhoid fever (11.7%), paratyphoid fever (6.4%), and leptospirosis (2.4%).
Bottom Line:
Western physicians seeing febrile and recently returned travelers from the tropics need to consider a wide profile of potentially life threatening tropical illnesses, with a specific focus on the most likely diseases described in this case series.
University of Maryland Section of Global Emergency Health
Author: Walid Hammad, MB ChB
End-expiratory Occlusion Test
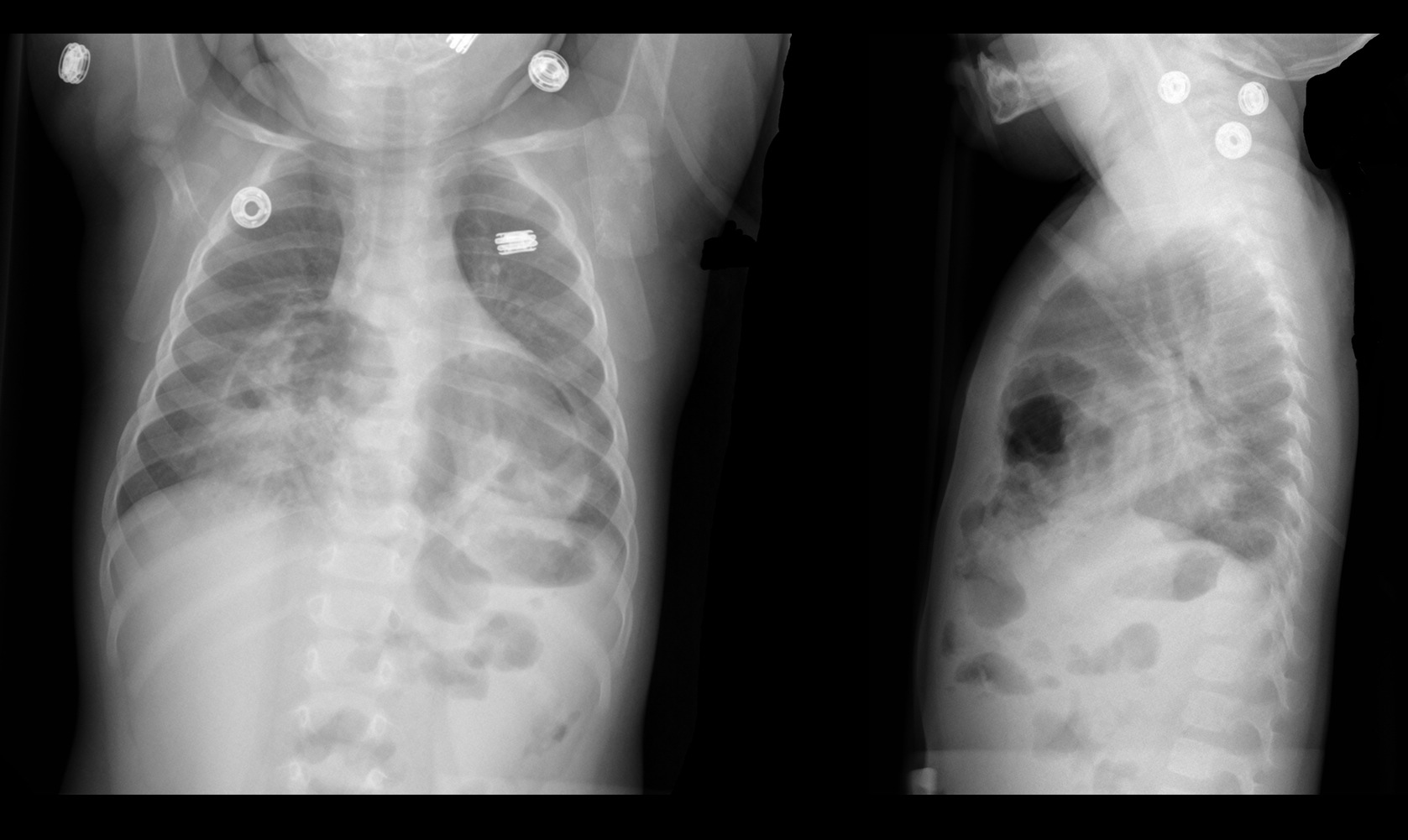
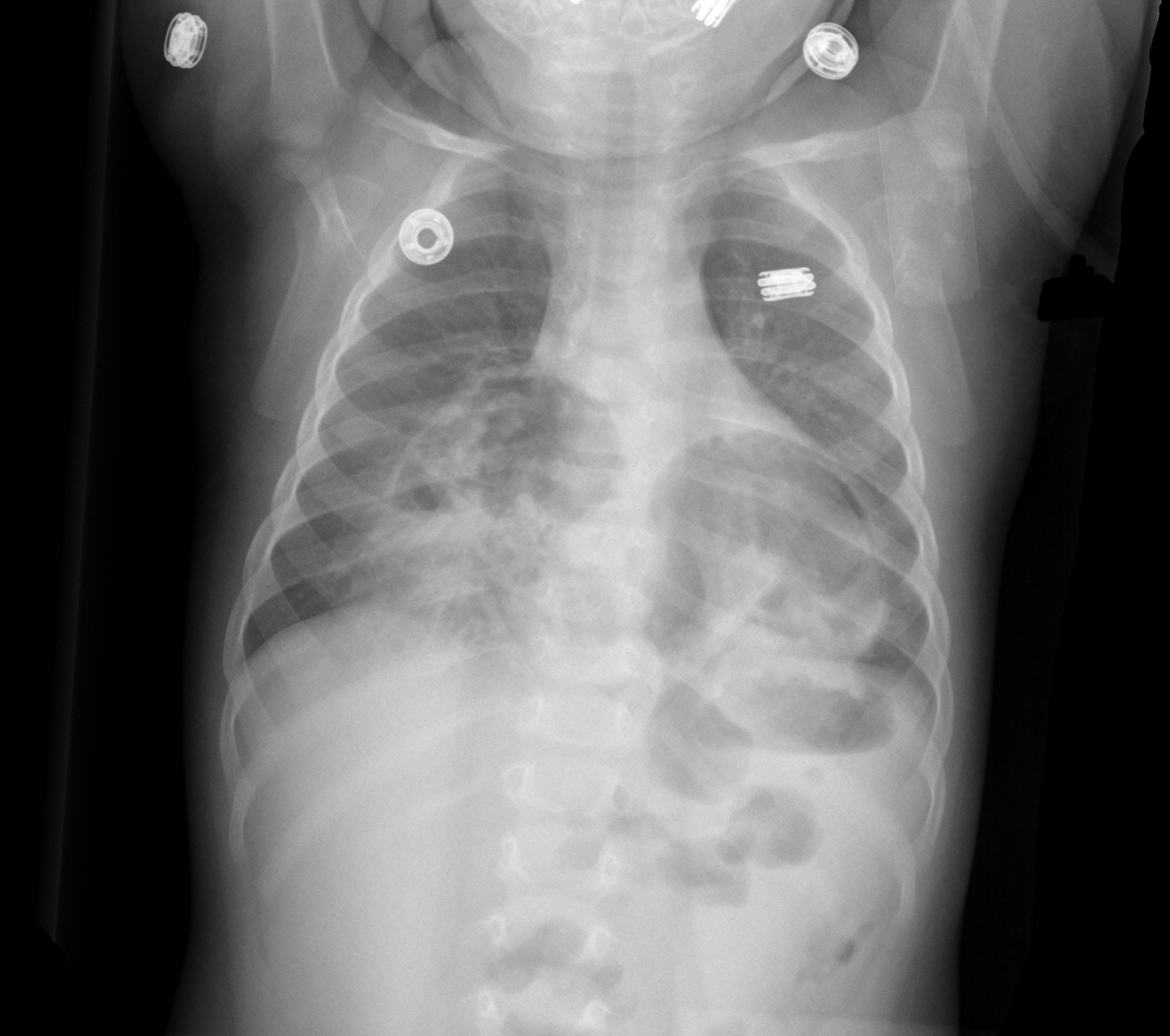
9 month-old presents with wheezing and the CXR is shown below. What's the diagnosis?
Adhesive capsulitis aka frozen shoulder
idiopathic loss of BOTH active and passive motion (this is a significant reduction of at least 50%)
Motion is stiff and painful especially at the extremes
Occurs due to thickening and contracture of the shoulder capsule
Affects patients between the ages of 40 and 60
Diabetes is the most common risk factor
Imaging is normal and only helpful to rule out other entities such as osteophytes, loose bodies etc.
Treatment includes NSAIDs, moist heat and physical therapy.
Patients should expect a recovery period of 1-2 years!
Ultrasound findings of appendicitis
Ultrasound images:
http://www.youtube.com/watch?v=d9jKM6x52nk
http://sonocloud.org/watch_video.php?v=MWHM3D7KD25H
http://sonocloud.org/watch_video.php?v=54862AYWGHGA
Utilizing 20% lipid emulsion at a dose of 1.5 mL/kg (100 mL Bolus) IV with repeat in 15 minutes in no response is being recommended in patients hemodynamic instabiity due to poisoning.
Probably more effective in lipophilic drugs is a current theory for the mechanism of action - the "lipid sink". The idea is that the lipids envelope the drug pulling it off its receptors or sequestering it in the intravascular space. A recent paper has added another mechanism - direct inotropic and lusiptropic effects.(1)
Also, if you think the therapy is experimental, think again. Another recent paper surveyed Poison Control Centers and found 30/45 Poison Centers in the US have a defined protocol for utilization of lipid emulsion therapy. The PCCs are recommending it more.(2)
What was once considered just a purely experimental therapy only used at the very end of code is becoming more mainstream. Comfort with its safety profile and anectodotal effiicacy continues to mount.
Clinical Presentation:
- A 40-year-old Hispanic man was admitted to the hospital after being found unconscious. He had a 2-day history of disorientation that manifested itself as his being unable to recognize family members.
- Upon admission he regained consciousness, becoming alert and oriented, but developed urinary retention and was unable to move or feel his lower extremities.
- Spinal MRI (with and without gadolinium) showed the spinal cord to be abnormally diffuse, with swelling and edema in the cervicothoracic region.
Diagnosis:
- After an extensive work up for lymphoma and CNS infection, he was discovered to have toxoplasmosis and was found to be HIV positive, which was previously undiagnosed.
Discussion:
- Approximately 10% of patients with AIDS present with some neurological deficit as their initial complaint, and up to 80% will have CNS involvement during the course of their disease.
- Myelitis is a known complication of AIDS and is occasionally the initial complaint.
The incidence of myelopathy may be as high as 20%, with 50% of the cases reported post-mortem
- Toxoplasmosis is the most common cause of cerebral mass lesions in patients with AIDS
Occurring in 3–10% of patients in the United States and in up to 50% of AIDS patients in Europe, Latin America, and Africa
Bottom Line:
New neurological deficit in any patient should raise suspicion of HIV infection
Most patients with AIDS that present with evolving myelopathy, characterized by extremity weakness, sensory involvement, spinal cord enlargement, enhancing lesions in brain or spinal cord CT or MRI, have toxoplasmic myelitis
University of Maryland Section of Global Emergency Health
Author: Terrence Mulligan DO, MPH
The Macklin Effect
Pneumomediastinum (click here for image) may be caused by many things:
The "Macklin Effect" is typically a self-limiting condition leading to spontaneous pneumomediastinum and massive subcutaneous emphysema after the following:
Pneumomediastinum secondary to the Macklin effect frequently leads to an extensive workup to search for other causes of mediastinal air. Although, no consensus exists regarding the appropriate workup, the patient's history should guide the workup to avoid unnecessary imaging, needless dietary restriction, unjustified antibiotic administration, and prolonged hospitalization.
Treatment of spontaneous pneumomediastinum includes: