How many times have you been frustrated in the peds ED when you have a child with a URI that has a significant night time cough and you feel like you have nothing to offer them for symptom control? The parent is frustrated because the child is not sleeping which means they are not sleeping and they are looking at you for help. We all know that OTC cough and cold medications are not helpful and may be harmful in children <2 yrs old and should be used with caution in children <6 yrs old. So what can you do? You can recommend a course of HONEY at night. Of course this does not apply to children < 1 yr who are at increased risk of botulism. A recent double-blind placebo-controlled trial published in Pediatrics in 2012 demonstrated reduced night time cough and subjective improved sleep quality in children age 1-5 who were given honey compared to placebo. This study supports previous less rigorous publications that found honey was an effective remedy on cough in children. Mechanism for honey's beneficial effect on cough is unknown but possibly related to close anatomic relationship between sensory nerve fibers that initiate cough and gustatory nerve fibers that taste sweetness. Of note, a recently published survey in Pediatric Emergency Care revealed that 2/3 of parents were unaware of the FDA guidelines regarding OTC cough and cold remedies in children! After you recommend HONEY for night time cough, take an extra minute and educate your parents about the potential dangers of cough and cold medicines in small children!
You have a treat bag full of candy, which one can cause hypertension, hyopkalemia, metabolic alkalosis, rhabdomyolysis, low renin activity, thrombocytopenia and hypoaldosteronism. (scroll down for answer)
Licorice syrup or licorice extract contains glycyrrhizic acid which has a mineralcorticoid-like effect and can cause of all of the effects. Don't worry, Twizzlers and other usual licorice candies do not have true licorice extract in them. It is found in herbal remedies and some "natural" candies and licorice flavored cigars. Don't pick the licorice !
Case Presentation: 28 year old woman from South Africa presents with 5 days of body weakness, nausea, vomiting and cough. BP 86/38, HR 142, RR 36, Temp 101.4 (oral) Sats 96% on RA. PMH: HIV+ last CD4=33, on HAART, history of pulmonary TB which was treated 2 years ago.
Clinical Question: The CT scanner, Xray and labs are down. What work-up can you do to best manage this patient?
Answer: The FASH Exam (Focused Assessment with Sonography for TB-HIV)
Technique: 6 probe positions--Similar to the FAST exam but with additional evaluation of the liver, the aorta, the spleen, as well as evaluation for pleural effusions over the diaphragm.
Evaluate for extrapulmonary TB (EPTB):
-Pericardial/Pleural effusion and ascites
-Periportal/para-aortic lymph nodes
-Focal liver and spleen lesions
(Go to http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3554543/ to view images of probe position.)
Bottom Line: The FASH exam can be taught to physicians with limited to no ultrasound experience. If there is concern for EPTB in an undifferentiated hypotensive patient, the FASH exam can performed in the emergency setting and treatment can be started.
University of Maryland Section of Global Emergency Health
Author: Laura Diegelmann, MD RDMS
The pregnant patient normally has increased cardiac output and minute ventilation by the third trimester. Despite this increase, however, these patients have little cardiopulmonary reserve should they become critically-ill.
Remember the mnemonic T.O.L.D.D. for simple tips that should be done for the pregnant patient who presents critically-ill or with the potential for critical illness:
15 year-old right-hand dominant male received a direct blow to the right arm with a hockey stick. What’s the diagnosis?

First-degree atrioventricular (AV) block is defined as an abnormally prolonged PR-interval >200ms. Although traditionally considered to be a benign clinical entity, not all first degree AV blocks are treated the same.
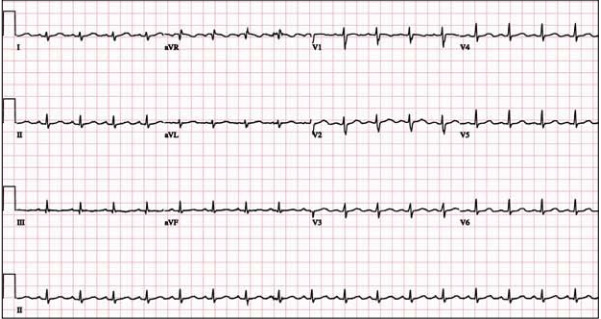
Markedly prolonged PR-intervals (PR >300ms) can cause symptoms and hemodynamic compromise due to inadequate timing of atrial and ventricular contractions. Consider the following ECG from a 32 YOF with intermittent episodes of syncope and dizziness…
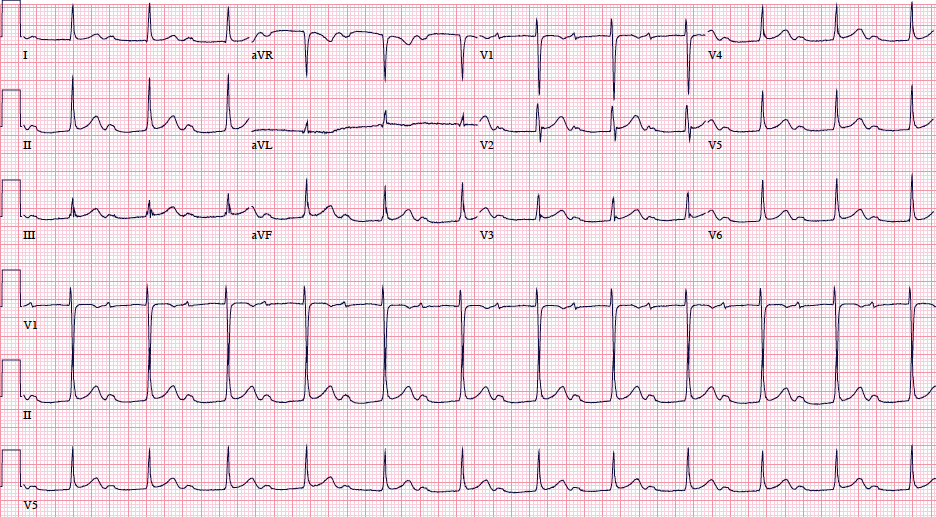
There is marked first degree AV block (PR=434 ms). When the PR-interval gets too long, AV dyssynchrony compromises ventricular filling and decreases cardiac output, similar to the so-called pacemaker syndrome.
Current ACC/AHA guidelines state that permanent pacemaker implantation is reasonable for marked first degree AV block with hemodynamic compromise or symptoms similar to those of pacemaker syndrome. (Class IIa, Level of Evidence B). The guidelines caution that pacemakers are not indicated in asymptomatic patients with isolated first degree AV block.
Want more emergency cardiology pearls? Follow me @alifarzadmd
Lateral hip pain
Findings of weakness and/or pain while testing hip abduction may point to gluteus medius muscle dysfunction with associated with greater trochanteric pain syndrome.
The Trendelenburg test may help. The patient stands on the affected leg. A negative test result occurs when the pelvis rises on the opposite side. A positive test result occurs when the pelvis on the opposite side drops and indicates a weak or painful gluteus medius muscle.
http://www.youtube.com/watch?v=TY-G4ErruUA
Yesterday's pearl generated several questions that I thought were worth answering briefly:
1) Why give it IM? Absorption rate is faster than SQ infiltration though theoretically could still cause necrosis
2) Is it only infilitration? Gangrene has occurred with inadvertent intra-arterial injection, SQ infiltration and even regular IV administration
3) Mechanism? Appears to be the drug and not diluent, diluting down the concentration as well as decreasing dose appears to help if you are going to give it IV
Here is a website if you wish to read more details:
https://www.ismp.org/newsletters/acutecare/articles/20060810.asp
If you are still using IV Phenergan, you need to be aware of the necrotic effect that occurs if it infiltrates. EDs have even removed it from their drug dispensing machines. It appears to be the drug and not the diluent. Mechanism is not completely understood. Below is a picture the plaintiff attorney will use about this well know adverse effect. If so many alternatives for IV antiemetic it is wise to reconsider IV phenergan.
General Information:
Area of the world affected:
Bottom Line:
University of Maryland Section of Global Emergency Health
Author: Emilie J.B. Calvello, MD, MPH
Background
Definition
Pathogenesis
Two-hit hypothesis: first hit is underlying patient factors causing adherence of neutrophils to the pulmonary endothelium; second hit is caused by mediators in the blood transfusion that activate the neutrophils and endothelial cells.
Differential
Can be confused or overlap with TACO or transfusion-associated volume/circulatory overload, which presents similarly but has evidence of increased BNP, CVP, pulmonary wedge pressure, and left sided heart pressures. Patients with TACO tend to improve with diuretic treatment
Supportive tests
Treatment
55 year-old male presents with chest pain. You take a look at his cardiac function with ultrasound and here's the patient's apical four-chamber view. What's in his right ventricle and why would it be there?
Ebstein's Anomaly
Pediatric patients with an isolated skull fracture and normal neurological exam have a low risk of neurosurgical intervention and outpatient follow up may be appropriate (assuming no suspicion of abuse and a reliable family). In a study published in 2011, a retrospective review over a 5 year period at a level 1 trauma center showed that 1 out of 171 admitted patients with isolated skull fractures developed vomiting. This patient had a follow up CT showing a small extra-axial hematoma that did not require intervention. 58 patients were discharged from the ED within 4 hours.
You can also check out another recent article published in Annals of Emergency Medicine on the same topic this month!
Drugs that cause hearing loss:
Reversible - Chloroquine, erythromycin, quinine, CO, loop diuretics, NSAIDS, ASA
Irreversible - aminoglycosides, bleomycin, vincristine, vinblastine, cisplatin, lead, mercury, arsenic
General Information:
Trachoma is the leading cause of preventable blindness caused by an infectious disease. It is spread by direct contact with people, objects, or flies carrying Chlamydia trachomatis. Blindness occurs due to corneal scarring with repeated infections (severe scaring of the eyelid-->eyelid inversion-->repeated corneal abrasions).
Clinical Presentation:
-Mild: Hypopigmented follicles on the inner eyelid; Moderate: inner eyelid scarring/eyelash inversion; Severe: corneal scarring/blindness (irreversible)
Diagnosis:
- Clinical: eyelid eversion and careful examination looking for the above
Treatment:
- Azithromycin 20mg/kg ONE TIME DOSE (preferred)
- 1% Tetracycline ointment bid x6 weeks
- If scarring or eyelid inversion is present, surgery is needed.
Bottom Line:
Trachoma is a clinical diagnosis and easy to treat early with a single dose of antibiotics. Patients with late findings should be referred for surgery.
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH, FACEP
There have been so many great talks at ACEP 2013, but Dr. Michael Winters' talk "The ICU is NOT Ready for Your Patient" was chock full of great critical care pearls. Here are just a few:
A 23 year-old male presents with the rash below. He originally presented to his primary care doctor for a sore throat and was given a prescription for a medication; this rash subsequently broke out. What's the diagnosis and which medication did he receive?

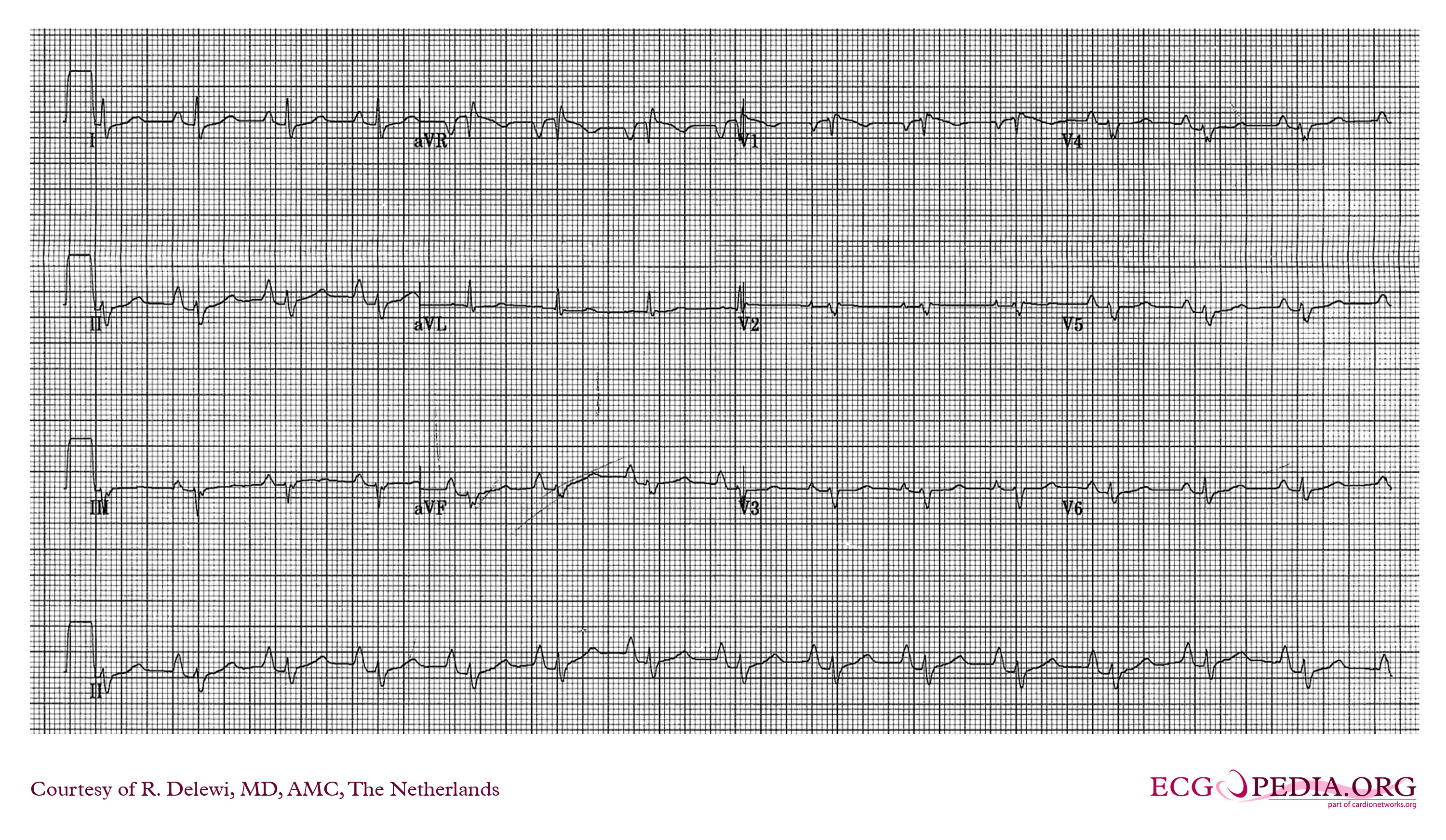
A 48 year-old female presents to the ED with progressive dyspnea and chest discomfort over the past 3 months. HR = 105, BP = 100/60 mmHg, with mild JVD on exam. Her ECG is shown below. What ECG abnormalites are present? What does your differential diagnosis include? What is the best initial diagnostic test?
Toxicologists should be aware of non-toxicological mimics of delirium, including anti-NMDA receptor encephalitis. It is an under-recognized progressive neurological disorder caused by antibodies against NMDA receptors.
Cases often present with altered mental status, autonomic instability, increased muscle tone, and movement disorders. It can easily be mistaken for neuroleptic malignant syndrome (NMS). A new case series describes two such patients for which toxicologists were consulted.
Must read links:
Dr. Leon Gussow provides a great review of the case series on his Poison Review blog.
Dr. Chris Nickson reviews the basics of the disease on the Life in the Fast Lane blog.