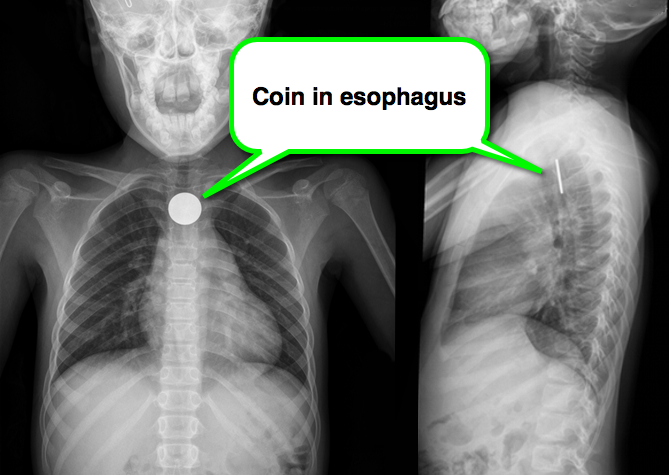
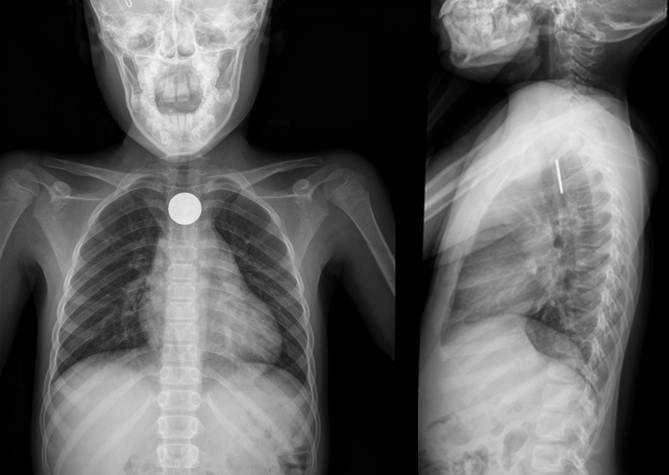
8 year-old girl presents with dysphagia and drooling, Xray is shown. What’s the diagnosis (and where is it located)?
Colchicine is known to be effective in treatment of recurrent pericarditis, but until recently its efficacy during the first attack of acute pericarditis has been uncertain.
A recent multicenter, double-blinded, RCT of patients with acute pericarditis found colchicine to be effective in reducing the rate of incessant or recurrent pericarditis (primary outcome), as well as the rate of hospitalization. Here are some highlights:
Bottom-line:
Colchicine is a safe and effective drug for the treatment of acute pericarditis. Consider adding colchicine to conventional therapies to reduce duration of symptoms, recurrences, and rate of hospitalization.
The thumb MCP joint is subject to arthritric changes.
Sx's of arthritis will frequently present with pain in a similar region to deQuervain's disease.
The basal joint grind test
Perform by stabilizing the triquetrum with your thumb and index finger and then dorsally subluxing the thumb metacarpal on the trapezium while providing compressive force with the opposite hand.
http://www.youtube.com/watch?v=oEJH7KFGx_Y
With several new diabetes medications available, it is important to know which ones are likely to cause hypoglycemia after overdose. Based on mechanism of action and reported cases, the likelihood of hypoglycemia after overdose is listed below by drug class.
Keep in mind that other drugs can interact with antidiabetics resulting in hypoglycemia. This table applies only to single agent ingestion/administration.
| Drug Class | Examples | Hypoglycemic Potential |
|---|---|---|
| Insulins | Glargine, Aspart, Detemir | High |
| Sulfonylureas | Glyburide, Glipizide | High |
| Meglitinides | Nateglinide, Repaglinide | High |
| Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists | Exenatide | Low-Moderate |
| Alpha-glucosidase inhibitors | Acarbose, Miglitol | Low |
| Thiazolidinediones | Rosiglitazone, Piaglitazone | Low |
| Biguanides | Metformin | Low |
| Dipeptidyl Peptidase 4 (DPP-4) Inhibitors | Sitagliptin, Saxagliptin | Low |
Background Information:
A recent review article in NEJM evaluated what effects globalization and climate change can be expected to have on human health. If global population increases and temperatures continue to rise, diseases that were once limited by either remoteness or climatologic regions may have new geographical spread.
Pertinent Conclusions:
There are three primary ways which climate change may be expected to affect health:
- Primary: Direct biologic consequences (i.e. heat waves, extreme weather events, air pollution)
- Secondary: Risks caused by process changes (i.e. decreased crop yields, tropical vectors with increased spread)
-Tertiary: More diffuse effects (mental health issues in failed farmers, conflict due to scarce water)
Bottom Line:
No matter what your views are on the causes, the current trend is that the overall climate is getting warmer and human population is increasing. Anticipation of possible consequences is key to planning for the future.
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH
Necrotizing Pneumonia
Necrotizing pneumonia is a rare, but potentially deadly complication of bacterial pneumonia.
It is characterized by the finding of pneumonic consolidation with multiple areas of necrosis within the lung parenchyma. Necrotic foci may coalesce, resulting in a localized lung abscess, or pulmonary gangrene if involving an entire lobe.
Most common pathogens: S. aureus, S. pneumoniae, and Klebsiella pneumonia.
Others include S. epidermidis, E. coli, Acinetobacter baumannii, H. influenzae and Pseudomonas.
Contrast-enhanced chest CT is the diagnostic test of choice and is also helpful in evaluating for parenchymal complications.
Empiric antibiotic therapy should include:
Consider an early surgical evaluation for the patient with necrotizing pneumonia complicated by septic shock, empyema, bronchopleural fistula, or hemoptysis.
This week's case is challenging, but very interesting...
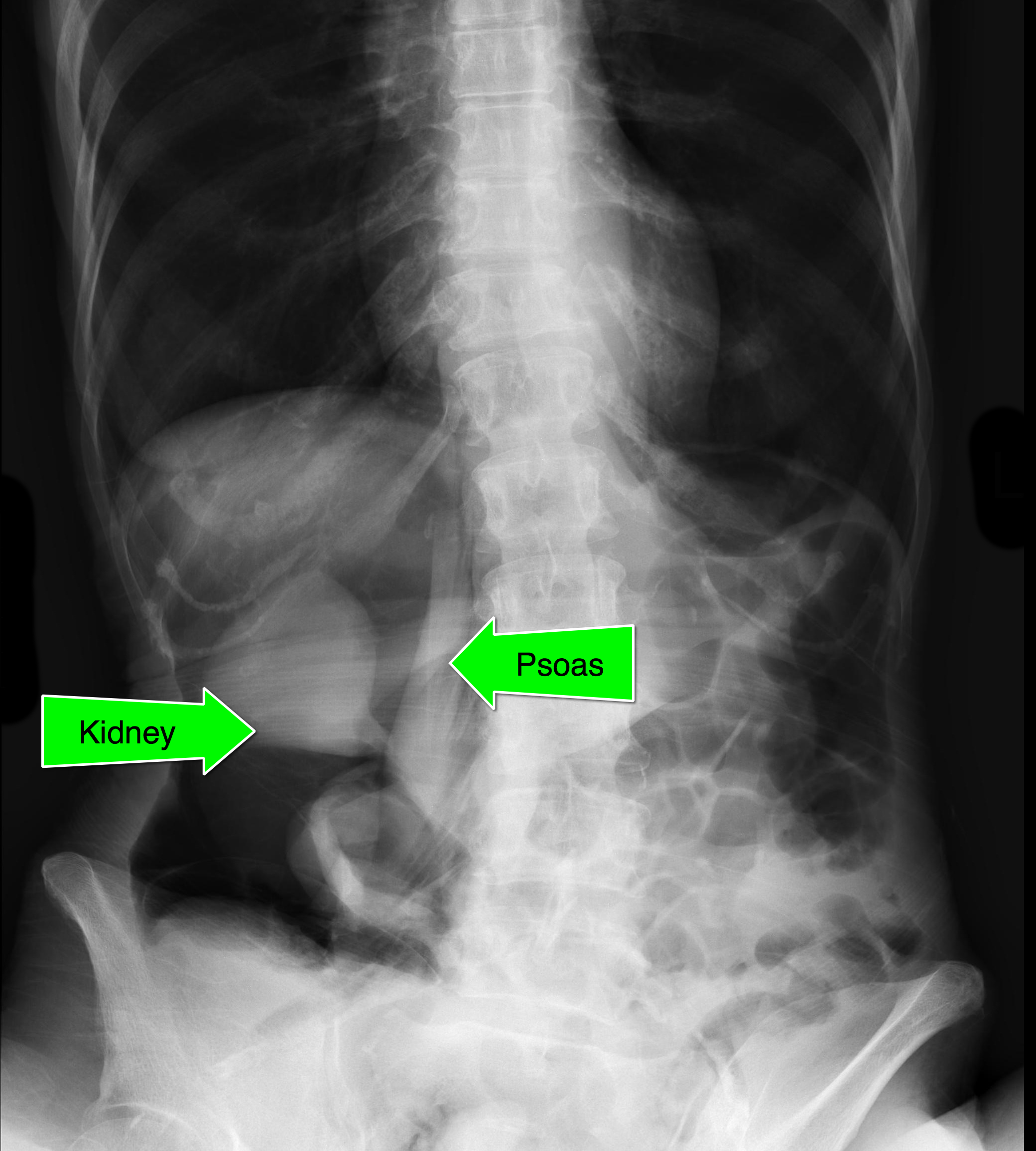
An elderly patient presents with a history of significant weight loss and chronic constipation; abdominal Xray is below. What's the diagnosis? (Hint: why is the right kidney and psoas muscle so well defined?)

*Please see the attachment below for Figures A-D
Although there is a paucity of data to guide dosing of antimicrobials in the critically ill obese patient, we can draw some conclusions from existing kinetic studies. Assuming normal renal and hepatic function, here's what to do:
Penicillins: Use the high end of dosing range. For example, if the plan is to use piperacillin/tazobactam 3.375 gm IV every 6 hours for a complicated intra-abdominal infection, use 4.5 gm instead.
Cephalosporins: Use the high end of the dosing range.
Carbapenems: Use the high end of the dosing range.
Quinolones: Use the high end of the dosing range.
Aminoglycosides: Dose using adjusted body weight. ABW (kg) = IBW + 0.4 X (actual body weight - IBW)
Vancomycin: 15-20 mg/kg actual body weight every 8 to 12 hours. Adjust based on trough level.
When dosing most antibiotics in critically ill obese patients, use the high end of the dosing range (if not more).
NMS is most often seen with the typical high potency neuroleptic agents (e.g haldol, fluphenazine)
All classes of antipsychotics can cause NMS, including low potency and newer atypical agents; antiemetics can cause this as well.
Symptoms usually occur after the first 2 weeks of therapy, but may occur after years of use
Signs and symptoms include:
mental status changes
muscular rigidity (“lead pipe”)
hyperthermia (>38 - 40 degrees).
Autonomic instability (tachycardia, tachycardia and diaphoresis)
Treatment includes discontinuation of the offending agent and providing supportive care.
While no clinical trials have ever been undertaken, dantrolene (muscle relaxant) is commonly used.
Bromocriptine (dopamine agonist) may also be used, and amantadine (dopaminergic and anticholinergic agent) is used as an alternative to bromocriptone
Recently, several case reports have documented the successful use of diazepam as a sole pharmacologic agent. This may be an alternative or a supplement to the above agents
UEDVT comprise 10% of all DVTs (majority are lower extremity), but incidence of UEDVT is rising; UEDVTs are categorized into distal (veins distal to axillary vein) or proximal (from superior vena cava to axillary vein)
Compared to lower extremity DVT, UEDVTs have lower:
75% of UEDVT are secondary (indwelling catheters, pacemakers, malignancy, etc.) and 25% are primary in nature; #1 primary cause of UEDVT is Paget – Schroetter disease
Up to 25% of patients with primary UEDVTs are eventually found to have an underlying malignancy; patients with idiopathic UEDVT should be referred for cancer workup
Treatment includes removal of the catheter (if no longer needed) and:
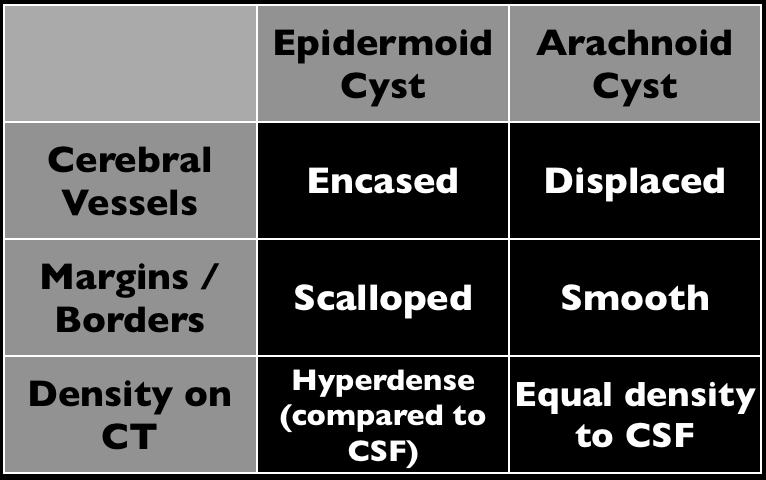
Elderly male presents with headache, confusion, and trouble with gait. What's in your differential diagnosis?
Adult ED patients are commonly found to have markedly elevated blood pressures (>160/100) without any signs or symptoms of acute organ injury (ie, cardiovascular, renal, or neurological).
A recently revised ACEP clinical policy aims to guide emergency physicians in the evaluation and management of such patients.
They make the following recommendations (Level C):
Bottom-line:
There's little evidence to guide the decision of which patients with markedly elevated blood pressures to test or treat in the ED. This new clinical policy suggests that routine screening and treatment is not required. Asymptomatic patients should be referred for close follow-up, but consider a BMP in patients with poor follow up.
Want more emergency cardiology pearls? Follow me @alifarzadmd
There are Type 1C Anti-Dysrhythmics, like propafenone and flecainide, that are utilized to suppress atrial fibrillation. They are called Type 1C due to their sodium channel blocking effects. Flecainide has a potent effect on the ECG and has caused significant and resistant widening of the QRS complex.
Typically, a sodium channel blocker like a TCA can be treated with hypertonic sodium bicarbonate but flecainide has been resistant to this at times and there is a reported overdose utilizing magnesium sulfate. (1) Keep that in mind if you were to see a widened QRS complex in the face of a flecainide ingestion.
There has been a Brugada ECG pattern also reported (I know Amal is smiling) (2) ontop of the widened QRS, PR intervals though minimal effect on the QT.
General Information:
-MERS-CoV (Middle East Respiratory Syndrome) is a novel coronavirus that produces a SARS-like syndrome. (You might have seen a pearl about this from us in March...)
-Since that time there have been a total of 102 laboratory-confirmed cases with 42 deaths (almost half!)
-All known cases had links to the Arabian Peninsula, although there has been some local non-sustained transmission
Relevance to the EM Physician: Consider MERS-CoV in patients with SARS-like syndrome who have traveled or had contact with someone who has traveled to the Arabian Peninsula within the past 14 days.
Bottom Line: Ask about recent travel in patients with severe acute respiratory illness. If you suspect MERS-CoV, contact your local health department.
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH
Background
Trial
Results
Conclusions
Bottom Line:
23 year-old patient presents with a rash on his palms and soles. He also states that he had a something strange on his genitals several weeks before. What's the diagnosis and what’s the treatment (including dosing) for this disease?

We will all see a patient that comes into the Emergency Department stating they have ingested some wild or self-picked mushrooms. Usually they will be actively vomiting and there will be no mushroom to identify. If there is, identification may still be difficult. There are no other clinical relevant symptoms that you can see until its too late. Amanita species is lethal and may require liver transplant. The most important question you can ask after trying to identify the mushroom is:
When did you eat the mushroom and how long after did the vomiting start?
As a general rule (with some exceptions), Amanita species cause vomiting and diarrhea in a delayed fashion 5-6 hours after ingestion. The other non hepatotoxic species usually cause vomiting within 1-3 hours.
Immediate vomiting <6 hrs from time of ingestion is good (usually).