Background:
Infection with the Hepatitis C virus can result in mild to severe liver disease. Morbidity and mortality from Hep C is increasing the US--many of the 2.7-3.9 million persons with Hep C are not aware of their infection.
Pertinent Information:
- Hepatitis C is now curable for many patients
- Current treatment recommendations are a combination of medications (pegylated interferon plus ribavirin plus a protease inhibitor).
- Research in this field is very active--treatment is likely to change in the next 3-5 years.
- Risk reduction strategies to protect the liver (i.e. eliminating alcohol and Hep A and B vaccination) are also recommended.
Critical New Recommendation
As much of the disease burden is in the “Baby Boomers,” the CDC now recommends one time testing of all persons born between 1945 and 1965.
Bottom Line:
While emergency department management is focused on the treatment of acute complications of liver disease, it is also important to have all age appropriate patients follow-up for testing and treatment of Hepatitis C with their primary care provider.
Hydroxyethyl starch (HES) is a colloid used for volume resuscitation in critically-ill patients.
Previous studies (click here) have compared crystalloids to HES during fluid resuscitation and have demonstrated that HES has an increased cost with more adverse effects. Adverse effects may include:
In the United States, the Federal Drug Administration published a warning on June 24th 2013 with respect to the use of HES in critically ill adult patients. Specifically, it warned about the use of HES in patients,
If a decision to use HES is made, the FDA warning advises to:
Bottom line: With an increased cost and evidence of harm compared to crystalloids, it appears the indications for use of HES are rapidly declining.
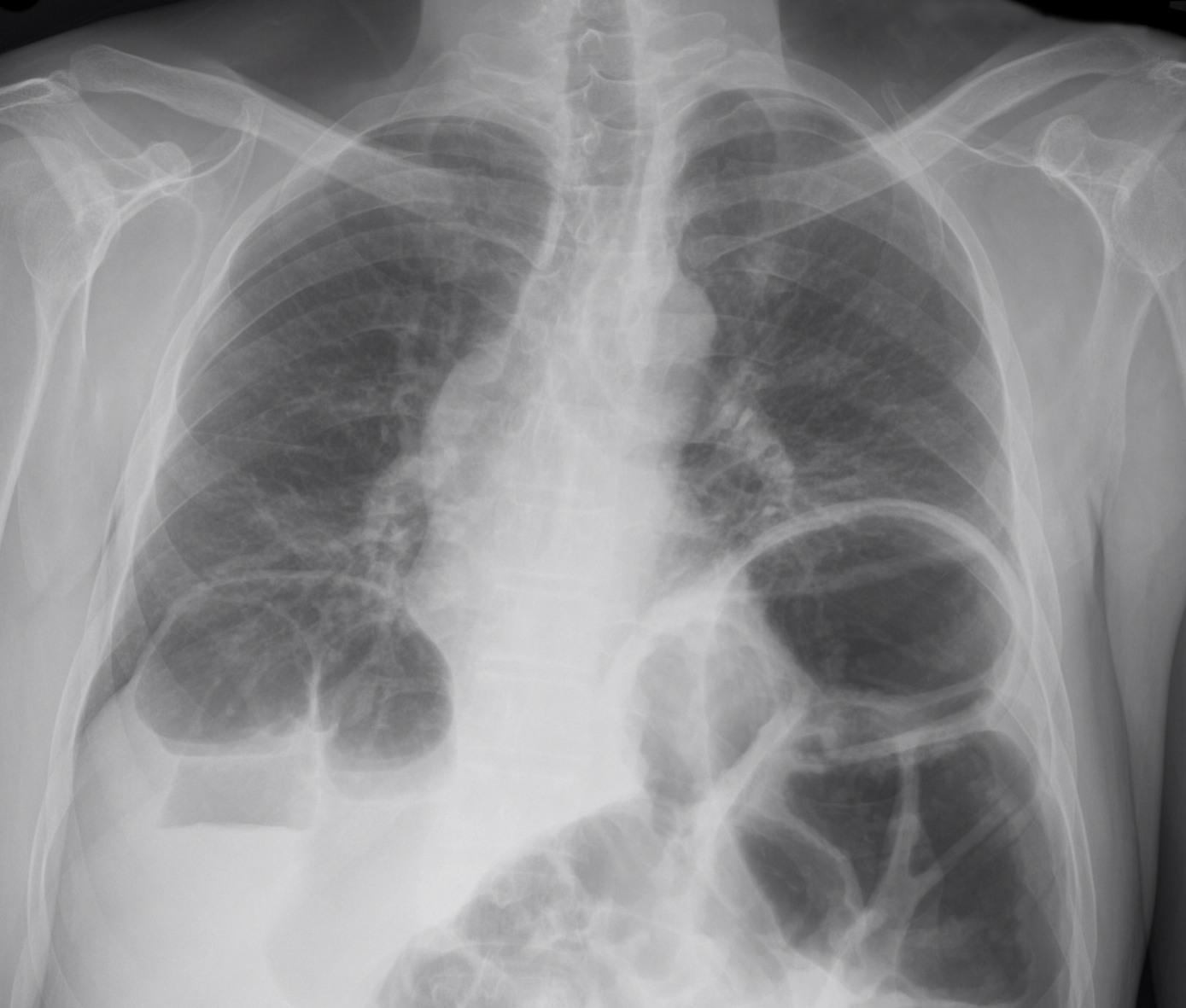
65 year-old male presents with nausea and diffuse abdominal pain, 3 days after knee replacement surgery. What's the diagnosis?
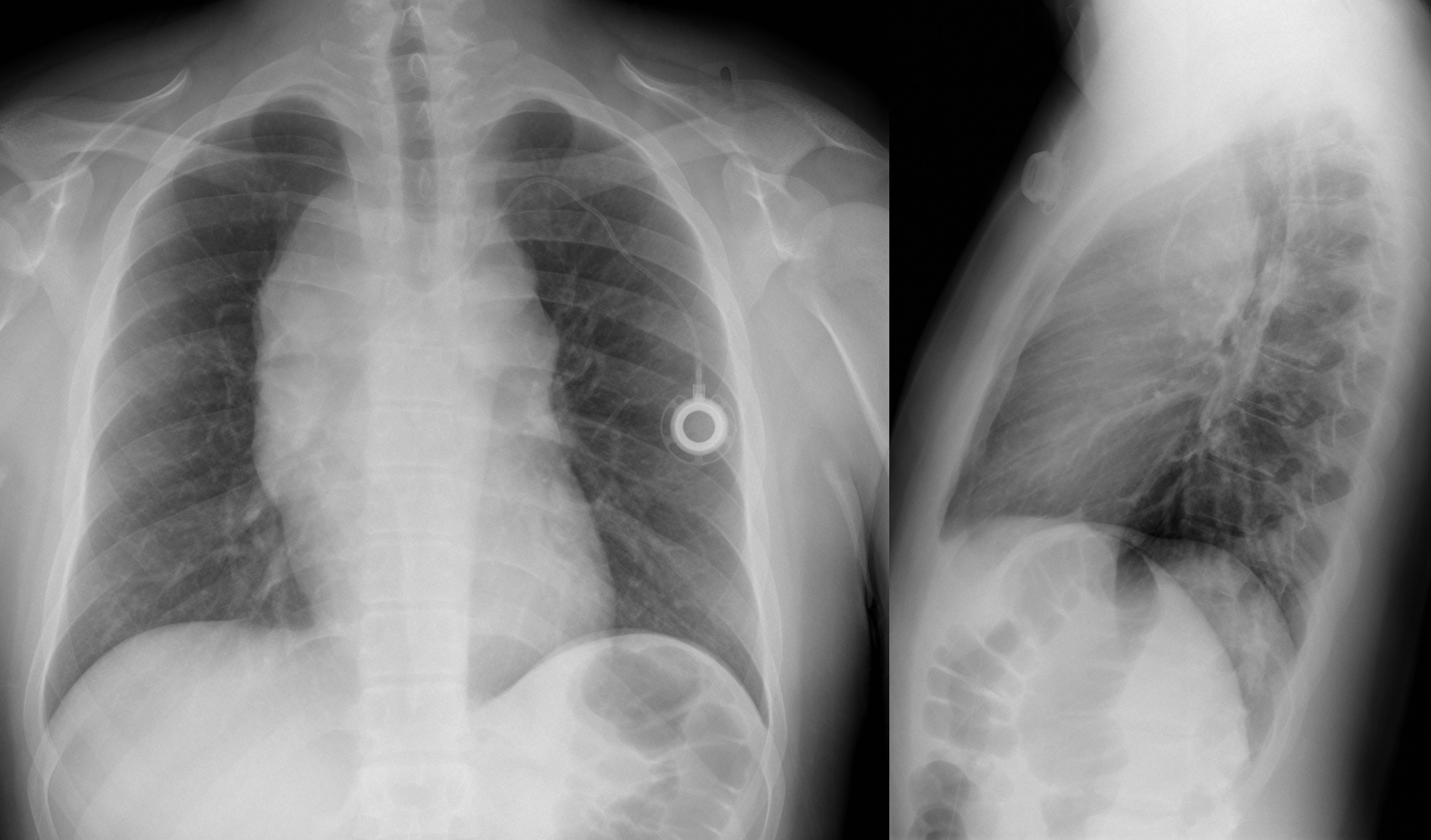
Sternal fractures
When reviewing a patient's medication list, there are always some that should catch your eye. Digoxin is one since we can measure it, has a low therapeutic index and elimination is effected when renal function is diminished. Another drug that should catch your eye is SOTALOL. Renally cleared and affected by even a minimally lower than normal magnesium. The toxic effect even at therapeutic levels is torsades de pointes.
One study, in a 736 bed hospital, showed 89% of patients prescribed sotalol were on an inappropriate dose due to renal function and an odds ratio of 3.7 increased re-admission rate at 6 months for the patients on the inappropriate dose of sotalol.
We can catch this in the ED. Involve your pharmacist, ED pharmacist or local toxicologist for dosing calculations.
General Information:
An estimated 70 children in the world die every 5 minutes-- 99% of these deaths are from developing countries, half in Sub-Saharan Africa , and two-thirds from preventable or easily treatable causes.
Area of the world affected:
One study examining the quality of hospital emergency care of 131 children in 21 hospitals in 7 developing countries found:
· 66% of hospitals did not have adequate triage; 41% of patients had inadequate initial assessment;
· 44% received inappropriate treatment and 30% had insuf cient monitoring.
· Frequent essential drugs, laboratory and radiology services supply outages
· Staffing and knowledge shortages for medical and nursing personnel
Relevance to the US physician:
The International Federation of Emergency Medicine (IFEM) used a consensus approach to develop the International Standards for Emergency Care of Children in Emergency Departments, published in July 2012.
· The standards covering initial assessment, stabilization and treatment, staf ng and training
· Guidelines for coordinating, monitoring and improving the pediatric emergency care are addressed
Bottom Line:
The IFEM International Standards for Emergency Care of Children provide an excellent resource for both clinicians and hospital managers in developing countries.
University of Maryland Section of Global Emergency Health
Author:Terrence Mulligan DO, MPH,FIFEM, FACEP, FAAEM, FACOEP, FNVSHA
--thanks and acknowledgments to Baljit Cheema, University of Cape Town and Stellenbosch University, South Africa
CVP and Fluid Responsiveness
Bifascicular block
Incomplete Trifascicular block
Complete Trifascicular block
Tennis Elbow
The tendon usually involved in tennis elbow is called the Extensor Carpi Radialis Brevis (ECRB).
The ECRB muscle helps stabilize the wrist when the elbow is straight.
Ask the patient to straighten the arm at the elbow and then perform resisted long finger extension. This will stress the ECRB and reproduce the pain. One can also ask the patient to lift the top of a chair in the air with the elbow extended.
General Information:
Hepatitis A is a food-borne illness that is prevalent in developing countries. Currently in the US we are experiencing an outbreak in 8 states related to a frozen blend of organic berries. (Linked to Townson Farms brand sold at Costco and Harris Teeter)
Clinical Presentation:
- Case definition: sudden onset of S/S + jaundice or elevated liver enzyme levels
- S/S: nausea, anorexia, fever, malaise, abdominal pain
Diagnosis:
- Hepatitis A IgM
Treatment:
- Exposed patients should be given the Hep A vaccine within 2 weeks of exposure
- Exposed patients >40 yrs old, <1 yr old, immunocompromised, or with chronic liver disease: give immunoglobulin instead (risk of more severe disease)
- Supportive care
Bottom Line:
Patients potentially exposed to Hepatitis A in the past 2 weeks should be given either the vaccination or immunoglobulin, depending on comorbid conditions. Treatment of active infection is supportive.
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH
Keep Immune Thrombocytopenic Purpura (ITP) in your differential for patients with thrombocytopenia and evidence of bleeding. Although ITP has classically been described in children, it can occur in adults; especially between 3rd- 4th decade.
Thrombocytopenia leads to the extravasation of blood from capillaries, leading to skin bruising, mucus membrane petechial bleeding, and intracranial hemorrhage.
ITP occurs from production of auto-antibodies which bind to circulating platelets. This leads to irreversible uptake by macrophages in the spleen. Causes of antibody production include:
Suspect ITP in patients with isolated thrombocytopenia on a CBC without other blood-line abnormalities. Abnormality in other blood-line warrants consideration of another diagnosis (e.g., leukemia).
ITP cannot be cured; treatments include:
Stanford type A (proximal) aortic dissection accounts for ~60% of all aortic dissections
Classic treatment includes direct surgical replacement of the ascending aorta w/prosthetic graft (+/- AV aortic repair/replacement)
~20-30% of these patients (*institutional dependent) are considered poor candidates for surgery and receive only medical management, which innately results in substandard outcomes
In this study those who were considered poor candidates for surgical repair underwent novel endovascular treatment
Endovascular repair in this study was considered both appropriate and improved traditional medical outcomes in patients who were considered poor candidates
Trapezium Fractures
Suspect the Diagnosis when you note
If you are suspected the diagnosis oblique radiographs or a CT scan of the wrist will note the fracture the best.
Treatment consists of placing the patient in a thumb spica splint.
In the treatment of acetaminophen poisoning with N-acetylcysteine (NAC), the PT/INR can be slightly elevated even in the absence of hepatotoxicity. Considering Prothombin Time (PT) is one of the criteria used to assess severity of liver damage in this setting, it is important to know how much the PT/INR can be affected by NAC and if it has an actual effect on coagulation factor levels.
Clinical Practice Pearls
General Information:
-Listeria can cause serious infections in vulnerable groups: adults >65 years old, pregnant women, newborns, immunocompromised
-In a recent CDC report, infection with Listeria was associated with a 20% mortality rate.
Clinical Presentation:
- History of cantaloupe, soft cheese, or raw produce ingestion
- Non-specific symptoms: fever, myalgias, occasionally preceded by GI symptoms
-Can have headache, stiff neck, confusion, AMS, miscarriage or stillbirth in pregnant women
Diagnosis:
- Blood, CSF, or amniotic fluid culture showing Listeria monocytogenes
- Listeria is a reportable disease
Treatment:
- Ampicillin and Penicillin G are the drugs of choice
- Add gentamycin in CSF infection, endocarditis, the immunocompromised, and neonates.
Bottom Line:
Listeria infections have a high mortality rate and can be found worldwide. Suspect in patients who have febrile syndromes and travel to areas where they may consume unpasteurized cheese.
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH
Rhabdomyolysis in the Critically Ill