Key components in the determination of return to play following concussion include assessment of 1) brain function, 2) reaction time and 3) balance testing
Balance testing has become increasingly utilized in the diagnosis and management of sports related concussion. Studies have identified temporary or permanent deficits in static and/or dynamic balance in individuals with mild-to-moderate traumatic brain injury and sports related concussion. An example of this is the Balance Error Scoring System (BESS). Three stances are testing (narrow double-leg stance, single leg stance and a tandem stance) with the hands on the hips and eyes closed for 20 seconds. The FNL Sideline Concussion Assessment Tool utilizes a modified BESS. Example video below:
http://www.youtube.com/watch?v=xtJgv-D7IdU
--The diagnosis and treatment of pediatric urinary tract infections (UTIs) can be broken down into different age groups. The AAP has recently updated its recommendations for children age 2 - 24 months.
--In ill-appearing febrile infants age 2 – 24 months, who require early initiation of antibiotics, clinicians should obtain urinalysis and urine culture by catheterization or suprapubic aspiration prior to administration of the first dose of antibiotics.
--Key components of diagnosing a UTI include: urinalysis with the presence of pyuria (>10 WBCs per µL) and bacteriuria. The ultimate diagnosis relies on identification of >50,000 CFUs per mL of a single urinary pathogen in culture.
--Treatment of most UTIs in well appearing infants 2-24 months can be done with oral antibiotics for a course of 7-14 days. Common antibiotics used include: amoxicillin-clavulanate, trimethoprim-sulfamethoxazole, or cephalosporins (cefpodoxime, cefixime) based on local patterns of susceptibility.
--Febrile infants with UTIs should undergo renal and bladder ultrasound (RBUS) to evaluate the renal parenchyma and identify complications of UTI in children who are not responding to treatment within 48 hours.
--Voiding cystourethrography (VCUG) to diagnose vesicoureteral reflux (VUR) as a cause of UTI should not be obtained routinely, but only in children with abnormal RBUS or with recurrent febrile UTIs.
-A genetic autosomal recessive blood disorders that result from a defect in either the alpha (α) or Beta (β) globin chain in the hemoglobin molecule.
-Most common in people from a Mediterranean origin.
-Three types depending on the affected globin chain, α, β, or Delta (δ)
-Presents as hemolytic anemia with hepato-splenomegaly.
-Can present as mild anemia and may be misdiagnosed as iron deficiency anemia.
-Diagnosis is made through studies such as bone marrow examination, hemoglobin electrophoresis, and iron studies.
-The disease can cause hemochromatosis, which may be worsened by repeated blood transfusions.
-Hemochromatosis damages multiple organs including the Liver, spleen, endocrine glands and the heart causing cardiomyopathy and consequently heart failure.
-Severe thalassemia usually requires blood transfusion on regular basis (first measure effective in prolonging life)
-Treatment of trait cases is symptomatic with analgesics, anti-inflammatory (steroids or NSAIDs)
-The introduction of chelating agents capable of removing excessive iron from the body has dramatically increased life expectancy.
-Deferasirox (Exjade) was approved by the FDA in January 2013 for treatment of chronic iron overload caused by nontransfusion-dependent thalassemia.
Ventilator-associated Pneumonia
65 year-old male with acute pulmonary edema. Ultrasound at the bedside shows this. What's the diagnosis?
The newest iteration of 'Guidelines for the Early Management of Patients with Acute Ischemic Stroke' was recently published. Here are the key revisions specific to blood pressure management:
If administering rtPA, blood pressure needs to be <185/110 mm Hg. That recommendation didn't change.
A foley is inserted in a fire victim patient. Urine return is in picture. Describe the reason for this colored urine.
Special Thanks to Dr. Doug Sward for the urine picture
Background Information:
Ever wonder what you would do if you were the first on scene after the earthquake in Haiti or in the Superdome as Hurricaine Katrina survivors started to arrive? How could you save the most lives? As is typical of emergency medicine, blood and gore tend to get the most attention, but if you want to save lives you have to think about what is the greatest life threat. In a large-scale disaster, it turns out, lack of water and abundance of feces kill the most the fastest and need to be addressed first.
The Sphere Project Handbook:
-one of the core documents of humanitarian response
-outlines what should be done to save the most lives in the first days, weeks, and months of a disaster.
-available free online (see reference below)
Pertinent Conclusions: (need-to-know recommendations for the first few days)
-Water: 15L/person/day (any quality--sanitize as per our previous pearl)
-Latrines: max 20 people/latrine, <50m from dwellings, >30m from water sources
-What kind?
-First 2-3 days: demarcated defecation area
-days-2 months: trench latrines (shallow trenches to defecate in)
Other hygeine:
-Solid waste disposal: one 100L refuse container/10 households, emptied at least 2x/week
-Dead bodies: dispose of according to local custom. Generally not an immediate source of infection
-Shelter: >3.5 sq. meters/person of covered floor space
Bottom LIne:
People's need for water and defecation will not stop in a disaster and too little water and too much excrement are the greatest immediate life threats to disaster survivors. Plan to deal with these early to save the most lives.
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH
Excessive and improper administration of local anesthetic (a.k.a. local anesthetic systemic toxicity or L.A.S.T.) can lead to cardiac toxicity with symptoms ranging from benign arrhythmias to overt cardiac arrest.
Administration of a 20% intra-lipid emulsion has been experimentally known to reverse L.A.S.T in animal models, but in 2006 the first documented human case of ILE was successfully used during cardiac arrest secondary to L.A.S.T. with hemodynamic recovery and good neurologic outcome. Many case reports have emerged since then, including the use of ILE in toxicity with other lipophilic drugs (e.g., calcium channel blockers, tricyclic antidepressants, etc.)
Several mechanisms have been proposed explaining how ILE works. They include:
Dosing of ILE:
Check out this video by our own Dr. Bryan Hayes(@PharmERToxGuy) and Lipidrescue.org for more information.
Just before you upgraded your old computer, recall what happened when you had Excel, Word and PowerPoint all open at the same time. In the concussed state, the brain is essenatially functioning like your old computer... and the more tasks it must perform, the slower it will work and slower it will recover. Hence the concept of cognitive rest. Below is taken from the AMSSM position statement of concussion in sport.
Return to school
There are no standardized guidelines for returning the injured athlete to school. If the athlete develops increased symptoms with cognitive stress, student athletes may require academic accommodations such as a reduced workload, extended test-taking time, days off or a shortened school day.
Some athletes have persistent neurocognitive deficits following a concussion, despite being symptom free. Consideration should be made to withhold an athlete from contact sports if they have not returned to their ‘academic baseline’ following their concussion (level of evidence C).
The CDC developed educational materials for educators and school administrators that are available at no cost and can be obtained via the CDC website. Additional resources for academic accommodations should be developed for both clinicians and educators (level of evidence C).
Adam Friedlander shared the practical application of this which I found amusing:
" I always recommend what Peds neuro called "a brain holiday" - my favorite part. All of our nurses look at me like I'm nuts, but it is now on our official concussion/CHI DC instructions. I always say to the kiddo: "You'll love this part. No homework, no reading." Then I turn to mom and dad and tell them they'll love the next part: "No TV, no video games."
Thank you for sharing Adam!!
Luu JL, Wendtland CL, Gross MF, et al. Three percent saline administration during pediatric critical care transport. Ped Emerg Care 2011;27(12):1113-1117
Typical opioid withdrawal include clinical symtpoms of piloerection, nausea, vomiting and diarrhea. If you were to see seizure, another etiology other than opioid withdrawal should be investigated.
Except in the case of neonates borne to women who have been taking opioids chronically such as a methodone patient. Once the child is born, symptoms of withdrawal may take days to weeks to materialize though seizures typically occur <10 days. The child is at increased risk of SIDS as well.
Japanese Encephalitis
Managing Traumatic Hemorrhagic Shock
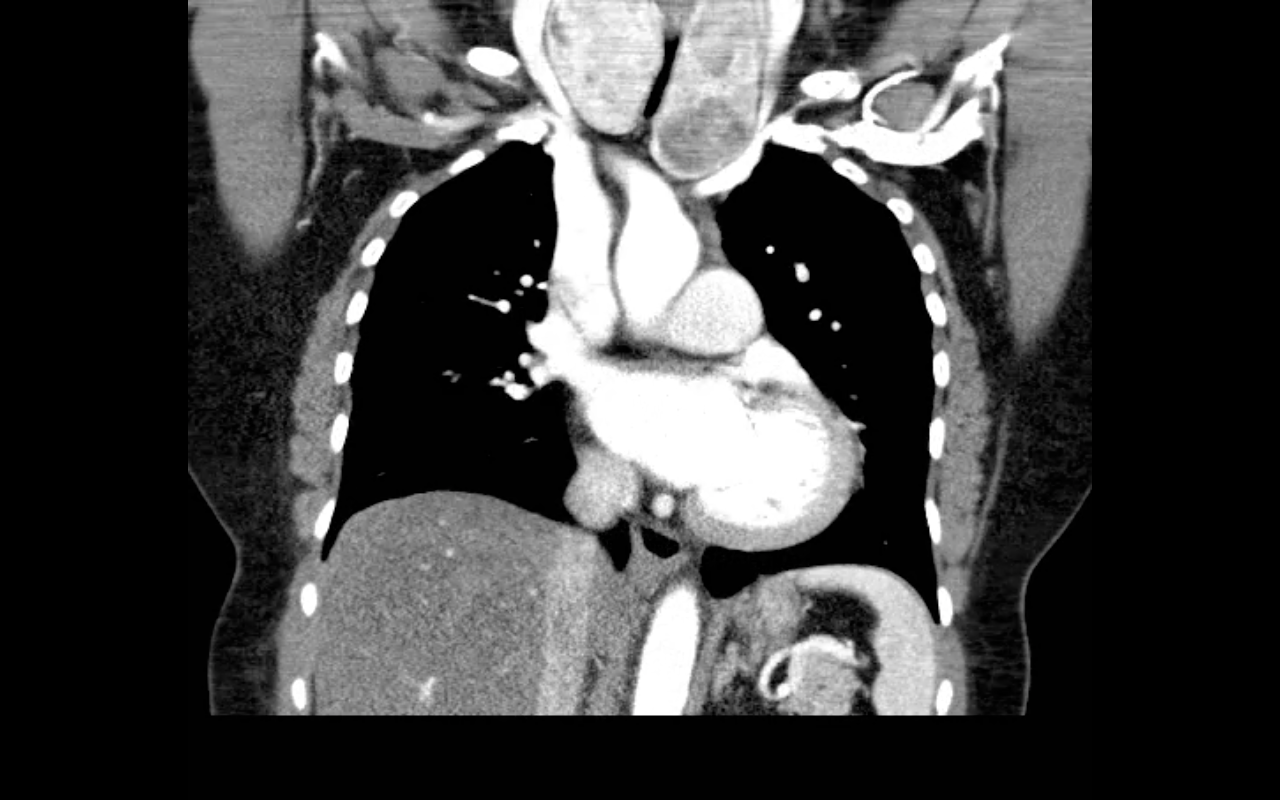
68 year-old female presents with stridor and palpable goiter. Here's a clip from CT of the chest. What's the diagnosis?