Smoke inhalation victims (house fires) are at risk of carbon monoxide (CO) and cyanide poisoning (CN). CO exposure/poisoning can be readily evaluated by CO - Oximetry but CN level can be obtained in majority of the hospital.
Lactic acid level is often sent to evaluate for CN poisoning.
Bottom line:
It is well known that the early aggressive utilization of IV nitrates and non-invasive positive pressure ventilation (NIV) in patients presenting with acute pulmonary edema will decrease the number of patients requiring endotracheal intubation and mechanical ventilation.
Often our tepid dosing of nitroglycerine is to blame for treatment failure. Multiple studies have demonstrated the advantages of bolus dose nitroglycerine in the early management of patients with acute pulmonary edema. In these cohorts, patients bolused with impressively high doses of IV nitrates every 5 minutes, are intuabted less frequently than patients who received a standard infusion (1,2). No concerning drops in blood pressure in the patients who received bolus doses of nitrates were observed. Using the standard 200 micrograms/ml nitroglycerine concentration, blood pressure can be rapidly titrated to effect.
Significant associations were found between concussion and
Lateral ankle sprain (P = 0.012)
Knee injury (P = 0.002)
Lower extremity muscle injury (P = 0.031)
Keep in mind that 50 – 80% of concussions may go undiagnosed or unreported.
A discussion about risks of early return after concussion should include mention of risks beyond repeat head injury/2nd impact syndrome
Study limits: Retrospective design limits ability to establish causation/reporting bias
Vitamin B12 deficiency, including pernicious anemia, is typically seen in malnourished individuals. Globally, it is widespread in those who live in poverty.
In the U.S., we often consider it in individuals who are chronic alcoholics. However, it can be seen in others, including:
The Neurocritical Care Society and Society of Critical Care Medicine just came out with new Guidelines for Reversal of Antithrombotics in Intracranial Hemorrhage (ICH) [1]
--PCC is now recommended over FFP in reversal of vitamin K antagonists (VKA) with elevated INR. Either should be co-administered with 10mg IV vitamin K. (Strong recommendation, moderate quality evidence)
TAKE AWAY: PCC should be probably be given over FFP in VKA-ICH when available
Take home points:
Acetaminophen is one of the most common pharmaceutical ingestions in overdose and a leading cause of acute of liver failure in the U.S. Early recognition and treatment is critical for prevention of morbidity.
Impact of an ED pharmacist on time to thrombolysis in acute ischemic stroke
Mechanical Ventilation in the Obese Patient
30 Year-old female presents to the ED for a rash. The rash started suddenly, mainly in her extremities and it is painful. The patient denied having fever or chills. Her past medical history is unremarkable. She admits to using cocaine frequently. The rash is shown in the picture.

Recent study evaluated whether an acetaminophen (APAP) level obtained less than 4-hour post acute ingestion can predict which patient would not require n-acetylcysteine (NAC). APAP cutoff level of 100 ug/mL was used for analysis. This was a secondary analysis of the Canadian Acetaminophen Overdose Study database (retrospective study).
Bottom line:
The prognosis of patients who experienced OHCA, who have not achieved ROSC by the time they present to the Emergency Department, is dismal. As such, it behooves us as Emergency Physicians to identify the few patients with a potentially survivable event. Drennan et al examined the ROC data base and identified the cohort of patients who had not achieved ROSC and were transported to the hospital. The overall survival in this cohort was 2.0%. Factors that predicted survival were initial shockable rhythm and arrest witnessed by the EMS providers. Patients arriving to the ED without ROSC, that had neither of those prognostic factors had a survival rate of 0.7%.
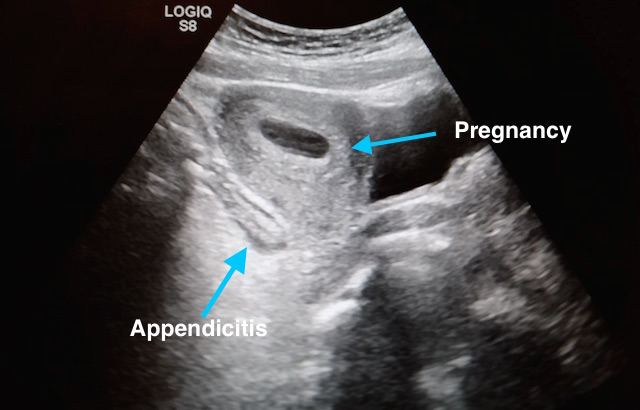
27 year-old G2P1 presents with 3 days of abdominal pain that is mostly suprapubic. Denies any urinary symptoms and vaginal bleeding. Physical examination reveals slight rebound in the right lower quadrant.
An ultrasound revealed the following. What's the diagnosis?

Consider esmolol IV 500 mcg/kg loading dose followed by a continuous infusion of 0-100 mcg/kg/min for patients in refractory ventricular fibrillation
Misclassification of adverse drug effects as allergy is commonly encountered in clinical practice and can lead to use of suboptimal alternate medications which are often less effective.
The World Health Organization announced on November 18th, 2016 that the Zika virus and associated consequences will no longer Public Health Emergency of International Concern. This changes the originally recommendation in February 2016.
However, Zika remains a “significant enduring public health challenge requiring intense action”. The consequences of the disease remains significant, especially for pregnant women and infants.
--In this study, PE was diagnosed in ~17% of patients hospitalized for syncope (though this represents only ~4%% of patients presenting to the ED with syncope).
--Patients with PE were more likely to have tachypnea, tachycardia, relative hypotension, signs of DVT, and active cancer -- take a good history and do a good physical exam!
--Consider risk stratifying (Wells/Geneva) and/or performing a D-dimer (i.e "rule out" PE) on your syncope patients, particularly when no alternative diagnosis is apparent.
Incidence and Cost of Ankle Sprains US Emergency Departments
In a sample of 225,114 ED patients with ankle sprains:
Lateral ankle sprains represent the vast majority of all ankle sprains (91%).
Lateral ankle sprains incur greater ED charges than medial sprains ($1008 vs. $914).
Lateral ankle sprains were more likely to have associated pain in the limb, sprain of the foot and abrasions of the hip/leg than medial sprains.
Medial sprains were more likely to include imaging.
Hospitalizations were more likely with high ankle sprains than lateral sprains.
There is a higher incidence of ankle sprains in younger patients (≤25 years) and in female patients (57%).