Lateral hip pain is a common presentation of hip pain.
Typically seen in runners and women over the age of 40 who start unaccustomed exercise.
Pain from OA of the hip which is typically medial (groin pain)
Lateral hip pain has traditionally been diagnosed at trochanteric bursitis.
Research suggests that lateral hip pain may be multifactorial and better termed Greater trochanteric pain syndrome.
Pain from the gluteal medius and/or minimus due to non-inflammatory tendonopathy is likely causative. This may cause a secondary bursitis.
Pain is insidious, gradual worsens and is variable based on activity type.
Also, can be seen after a fall resulting in tearing.
Pain is described as a deep ache or bruise. It can stay localized or radiate down lateral thigh towards knee.
Patients report night/early morning pain and when rolling over onto the outer hip on affected side.
Fatigue from prolonged sitting, walking and single leg loading activities such as walking up stairs.
Provoking activities and postures cause compressive forces on the involved tendons.
These generally occur when the hip is adducted across midline such as with
Side sleeping,
Place pillow between legs to align pelvis and keep knee and hip in line
Crossed leg sitting
Sit w/ knees at hip distance and feet on floor
Selfie poses - Standing w a hitched hip (pushing hip to the side).
Attempt to correct biomechanical issues before progressing directly to bursal steroid injection
May only be a temporary fix if underlying issue not addressed.
A helpful clinical guide
https://bjgp.org/content/bjgp/67/663/479/F1.large.jpg?download=true
Droperidol has recently become available again in select U.S. institutions. It has been used as an antiemetic and to treat agitation prior to the FDA’s black box warning (for QT prolongation) and national shortage.
Recently, a retrospective study was conducted (Melbourne, Australia) in the use of droperidol in the management of cannabinoid hyperemesis syndrome (CHS).
Results
689 medical records were identified from January 2006 to December 2016.
76 cases met diagnostic criteria of CHS (below)
Droperidol group (DG) = 37; no droperidol group (NDG)= 39
Median length of stay:
Median time to discharge after final drug administration:
Frequency of droperidol (dose) used:
Metoclopramide and Ondansetron use in non-droperidol group was twice that of droperidol group
Conclusion
Phenytoin can be a complex medication. There are different levels than can be ordered, adjustments based on albumin, various pharmacokinetic equations, and multiple formulations. Below are the simplified answers to some of the most common questions (see in-depth section for explanations):
Which phenytoin level (free or total) do I order?
Total Phenytoin Level.
What do I do after the level results?
Undetectable Level: Load patient with 20 mg/kg of total body weight (max dose 1,500 mg).
Subtherapeutic Level (<10 mcg/mL): Calculate an approximate loading dose using this equation….Phenytoin Dose (mg)=(15-measured total level)*(0.7*patient weight).
Therapeutic Level (10-20 mcg/mL): Add an additional agent.
Supratherapetutic/Toxic Level (>20 mcg/mL): Contact Poison Center (1-800-222-1222).
What formulation do I order for loading?
IV: Use fosphenytoin.
PO: Any formulation will work. Give as a single loading dose or, if concerned for GI upset, give in 2-3 divided doses separated by 2 hours.
***Disclaimer: These answers are simplified for the initial management of most patients in the ED. More complex answers may be required in some situations.***
Ever been in an acute rescucitation and found yourself unable to remember all of those famous ACLS Hs and Ts? I know I have. A few years ago Littman et al published an alternative approach to critically ill, hypotensive medical patients with non shockable rhythms. Unfortunately, it seems like some of the enthusiasm for this approach has died down, but I still think it's something you're more likely to recall in a pinch than the Hs and Ts and is a better way of getting started with a hypotensive non-trauma patient. And it's so simple you may actually remember it!
1) Look at the monitor. Is the rhythm narrow or wide?
2a) Narrow - more likely a mechanical problem (tamponade, tension PTX, autoPEEP, or PE). Give IVF and search for one of these causes (and correct it!). Keep in mind that ultrasound can help you differentiate a lot of these.
2b) Wide - more likely a metabolic problem (hyperK, sodium channel blockade, etc*). Give empiric calcium, bicarb, and other therapies targeted for these problems (if desired) and get stat labs.
Take a minute and either go to this REBEL EM post:
https://rebelem.com/a-new-pulseless-electrical-activity-algorithm/
To review this, or look at the attached diagrams.
*Dr. Mattu would want me to remind you that hyperkalemia IS a sodium channel poisoned state, so there's no need to think of these two separately
A recent epidemiology study in Pediatrics looked at concussions in 20 high school sports during the 2013–2014 to 2017–2018 school years.
For every athlete, one practice or competition was counted as one exposure.
Overall, 9542 concussions were reported for an overall rate of 4.17 per 10 000 athletic exposures (AEs).
Football continues to have the highest incidence with a concussion rate of 10.40 per 10 000 AEs.
As in previous studies, rates in competition (33.19 to 39.07 per 10 000 AEs) are increasing and higher than rates in practice which are lower and decreasing over the study period (5.47 to 4.44 per 10 000 AEs).
This may reflect better reporting or increasing injury rate
In all 20 sports, recurrent concussion rates decreased from 0.47 to 0.28 per 10 000 AEs.
Confirming prior studies, among sex-comparable sports, concussion rates were higher in girls than in boys (3.35 vs 1.51 per 10 000 AEs).
Also, among sex-comparable sports, girls had larger proportions of concussions that were recurrent than boys (9.3% vs 6.4%).
This study may reflect effective implementation of strategies to reduce concussion incidence such as mandatory removal from play and more stringent requirements associated with return to play.
Bottom line: Balance fluid resuscitation with LR was not associated with improved outcomes compared to NS and pediatric sepsis. Selective LR use necessitates a prospective trial to definitively determine comparative effects among crystalloids.
Patients with drug-induced cardiogenic shock [DIC] (e.g. overdose of CCB/BB, membrane stabilizing agents, etc.) are often managed with medical interventions such as vasopressors, bicarbonate infusion, high-dose insulin, lipid emulsion therapy. A fraction of these patients may be refractory to the standard medical therapy. VA-ECMO (venoarterial extracorporeal membrane oxygenation) has been utilized in such situation; yet clinical experience of using VA-ECMO in DIC is limited.
A recent retrospective study of the Extracorporeal Life Support Organization’s ECMO registry showed
Conclusion
Bottom Line: Consider cryptococcal meningitis even in immunocompetent patients.
ICU admission rates for all acute PEs vary wildly across the country (<5% to ~80%).
To predict which hemodynamically stable, normotensive PE patients should be admitted to the ICU, a single-center retrospective analysis of 7 years’ data sought to describe the reasons why normotensive patients with PE required vasopressors within 48 hours of admission to the ICU. The authors studied 293 patients admitted to the ICU at Beth Israel Deaconess in Boston and found only 8 patients (2.7%) who decompensated within the first 2 days. Of MANY variables studied, only respiratory rate was significantly different between those who decompensated and those who did not (mean RR 29 with range 26-32 in the decompensated group vs mean 21 with range 17-24).
Bottom Line: cost control experts may lean on you to admit fewer PE patients to the ICU. There is no perfectly reliable way to predict which normotensive patient with a PE will decompensate. The PESI score has been validated but even the low risk cohort had 1.6% mortality at 3 days. The BOVA score has been validated but its endpoint of mortality at 30 days is less useful for planning admission. Tachypnea should concern you.
The Critically Ill Geriatric Patient with Sepsis
Synthetic turf playing surfaces have been growing in popularity over the last decade and seem to have become a new standard.
Due to the need for durable fields that can accommodate multiple teams/activities, in addition to the high cost of maintaining grass and the need to conserve water, many parks and schools have switched from grass to turf. Turf is advertised as maintenance free but ….this is not the case.
Locally, at M&T Bank Stadium, groundskeepers drive a LitterKat turf sweeper across the field for 4 hours 2-3 times a week to ensure that the synthetic rubber is cleaned and distributed evenly. The field is also repainted every 4 games because the paint may become hard. The cost of this level of maintenance is beyond what many parks and local high schools can afford.
A recent study examined high school concussion data at almost 2000 high schools with over 14,000 recorded concussions. Researchers concluded that more concussions occurred in games than practices. Interestingly, they also found that playing surface was significantly associated with concussion. Almost 90% of all injuries occurred on turf-based surfaces. Turf outweighed all other mechanisms of injury, including helmet-to-helmet hits and grass playing surface. Between 10 and 15.5% of concussions occur from helmet to ground contact. In the NFL, this mechanism accounts for about 1 in 7 concussions.
Attempting to limit total exposure time in practice and games on turf surfaces may be beneficial until more study is needed.
The rate of suicide attempt has been increasing over the past decade. A recently published article investigated the temporal trend of suicide attempts in adolescent/young adult population (10 – 25 years old) from 2000 to 2018.
Methods
Results
Top 5 substance involved in suicide attempt
Agents associated with serious medical outcome (after 2011)
Conclusion
Rationale: Data regarding temperature management in patients suffered from cardiac arrest with nonshockable rhythm was inconclusive.
Objective: whether moderate hypothermia at 33C, compared with normothermia at 37C would improve neurologic outcome in patients with coma after cardiac arrest with nonshockable rhythm.
Outcome: survival with favorable 90-day neurologic outcome (Cerebral Performance Category scale 1-2/5)
SummaryThere was higher percentage of patients achieving CPC 1-2 in the hypothermia group (10.2%) vs normothermia group (5.7%, Hazard Ratio 4.5, 95% CI 0.1-8.9, p=0.04)
This randomized multicenter trial involved 581 patients with cardiac arrest and nonshockable rhythm. Hypothermia group included 284 patients vs. 297 in the normothermia group. Median GCS at enrollment = 3.
Majority of patients was cooled with the use of a basic external cooling device: 37% for hypothermia and 50.8% for normothermia group.
There was higher percentage of patients achieving CPC 1-2 in the hypothermia group (10.2%) vs normothermia group (5.7%, Hazard Ratio 4.5, 95% CI 0.1-8.9, p=0.04)
Limitation:
A. The study used strict enrollment criteria:
B. normothermia group had higher proportion of patients with temperature at 38C.
C. Hypothermia group underwent temperature management of 56 hours vs. 48 hours for normothermia patients.
Take home points:
In a selected group of patients with cardiac arrest and nonshockable rhythm, moderate hypothermia at 33C may improve neurologic outcome.
E-cigarette (vaping) use has become increasingly popular over the past 10 years, especially among adolescents. Intentional exposure (i.e. ingestion in self harm) of nicotine (e-cigarette liquid) can be life threatening where it can produce mixture of stimulatory (early), cholinergic toxicity and muscle paralysis/respiratory failure by blocking the neuromuscular junction. However, the severity of clinical toxicity in unintentional exposure can vary widely depending on the dose/route/circumstance of their exposure.
A recently published study investigated the characteristics of e-cigarette liquid exposure between Jan 1, 2010 to Dec 31, 2018 using the National Poison Data System
Result
Top 4 clinical/demographic characteristics are listed below.
Age group:
Route of exposure
Level of care:
Clinical effects - overall
In <5 years group
Conclusion
Blood Transfusion Thresholds in Specific Populations
Sepsis - 7 g/dL
Acute Coronary Syndrome - no current specific recommendations pending further studies
Stable Cardiovascular Disease - 8 g/dL
Gastrointestinal Bleeds
Acute Neurologic Injury - Traumatic Brain Injury - 7 g/dL
Postpartum Hemorrhage - 1:1:1 ratio strategy
Intersection Syndrome
De Quervain’s is a common tenosynovitis is involving the the 1st dorsal compartment of the wrist/forearm.
Intersection syndrome is a tenosynovitis that occurs at the intersection of the 1st and 2nd dorsal compartments.
Pathology located at crossing point of the 1st compartment structures (APL and EBP) with the radial wrist extensors (ECRB and ECRL)
Occurs most commonly from repetitive wrist extension and is common in rowers, weight lifters, and in those playing racquet sports.
Occurs about 4 to 6cm proximal to the radiocarpal joint VERSUS De Quervain’s which occurs near the level of the radial styloid.
Pain worse with resisted wrist and thumb extension
Radiographs not required
Splint and start NSAIDs
Recalcitrant cases can be referred for corticosteroid injection
https://stemcelldoc.files.wordpress.com/2012/09/intersection-syndrome-referral-pain-pattern1.jpg
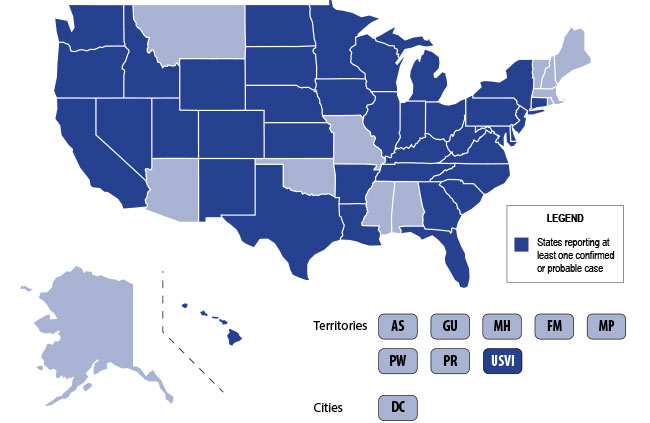
The U.S. is currently experiencing an epidemic of a severe lung disease termed Vaping-Associated Pulmonary Illness (VAPI), with over 500 cases and 7 deaths across 38 states and 1 U.S. territory since July 2019.
The clinical presentation of VAPI varies --
Diagnostics --
Treatment is supportive +/- steroids --
Bottom Line: Include vaping-associated pulmonary illness in your differential for patients presenting with acute lung disease.
- Tibial tubercle avulsion fractures are rare and pediatrics, accounting for less than 3% of all epiphyseal injuries in children ages 11-17 years.
- The typical mechanism is a sudden forceful quadriceps contraction. Patients present with sudden pain after sprinting or jumping with pain, bruising, deformity or swelling over the tibial tubercle and with a decrease ability to extend the leg.
- 10 to 20% of cases result in anterior compartment syndrome related to the rupture of the anterior tibial recurrent artery.
- Although directly measured intra-compartmental pressures can facilitate the diagnosis of compartment syndrome, interpretation of these values can be challenging with healthy children having higher average lower leg compartment pressures than adults. Treatment of subsequent compartment syndrome is often based on a high index of suspicion.
{kind=link}
{kind=link}