Non-opioid medications such as gabapentin are frequently prescribed for the management of pain.
A retrospective study of the National Poison Data System (data collected by the U.S. Poison Centers) from 2013 – 2017 showed increasing trend of gabapentin exposure.
Gabapentin exposure increased between 2013 and 2017 by:
5 most commonly co-ingested substances with gabapentin
16.7% of the isolated gabapentin exposure required hospitalization.
Conclusion:
Hemophagocytic Lymphohistiocytosis (HLH) – Part I
A rare, but important disease that is becoming more widely recognized and more frequently diagnosed. This disease, while uncommon, is rapidly progressive and caries a high mortality rate.
Causes are not completely understood, but involve abnormal activation of the immune response due to a failure of the typical downregulation in hyperinflammatory processes.
Two types exist:
Congenital/Familial – genetic predisposition which usually requires a triggering event to occur
Acquired – occurs in adults with no known predisposition (often have underlying genetic predispositions) – triggering events include infections , immunodeficiency, rheumatologic disorders, and malignancy in addition to many others.
Diagnosis is challenging due to the wide variety of symptoms and constellation of symptoms, which often mimic more common infections/sepsis presentations. Common symptoms include the following:
Symptoms can, and do, occur in any body system – rashes, conjunctivitis, DIC, LFT abnormalities, hypotension/shock, and respiratory failure are all common concomitant findings in the presentation of HLH
More on the specific diagnosis and treatment to follow in part II...
Urinary retention in pediatrics is defined as the inability to void for more than 12 hours in the presence of a palpable bladder or a urine volume greater than expected for age.
Maximum urine volume calculation for age: (age in years + 2) x 30ml.
Causes of urinary retention include mechanical obstruction, infection, fecal impaction, neurological disorders, gynecological disorders and behavioral problems.
The distribution is bimodal occurring between 3 and 5 years and 10 to 13 years.
There are few conditions that can be as dramatic or difficult to control as variceal GI bleeding in a cirrhotic patient. It is important to be familiar with all options in these cases, from Blakemore/Minnesota tube placement to massive transfusion to when and which consultants to get involved. In cases that are refractory or not amenable to endoscopic intervention, emergent interventional radiology consultation for Transjugular Intrahepatic Portosystemic Shunt (TIPS) may be a consideration. In high risk cases, think about getting IR on the phone at the same time as you engage GI, in case endoscopic management fails. Variceal bleed patients can decompensate rapidly, get your consultants involved early!
Generally accepted indications for emergent TIPS (both of the following should be true):
-GI bleeding not amenable or not controllable by endoscopy
-Cause is felt to be variceal. May also consider in portal hypertensive gastropathy
Contraindications:
-Right heart failure or pulmonary hypertension
-Severe liver failure (MELD > 22, T Bili > 3 or Child-Pugh C. In these cases TIPS may not confer a significant survival benefit)
-Hepatic encephalopathy (relative contradindication. HE may be worsened by TIPS).
-Polycystic liver disease (makes TIPS technically challenging)
-Chronic portal vein thrombus (makes TIPS technically challenging. Acute PV thrombus is NOT considered a contraindication)
Bottom Line: In cases of variceal GI bleeding from portal hypertension, consider getting IR on the phone early to discuss emergent TIPS.
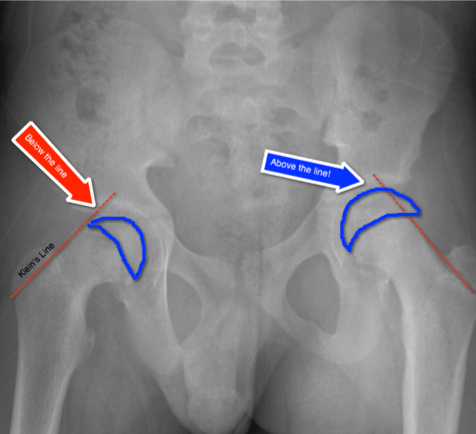
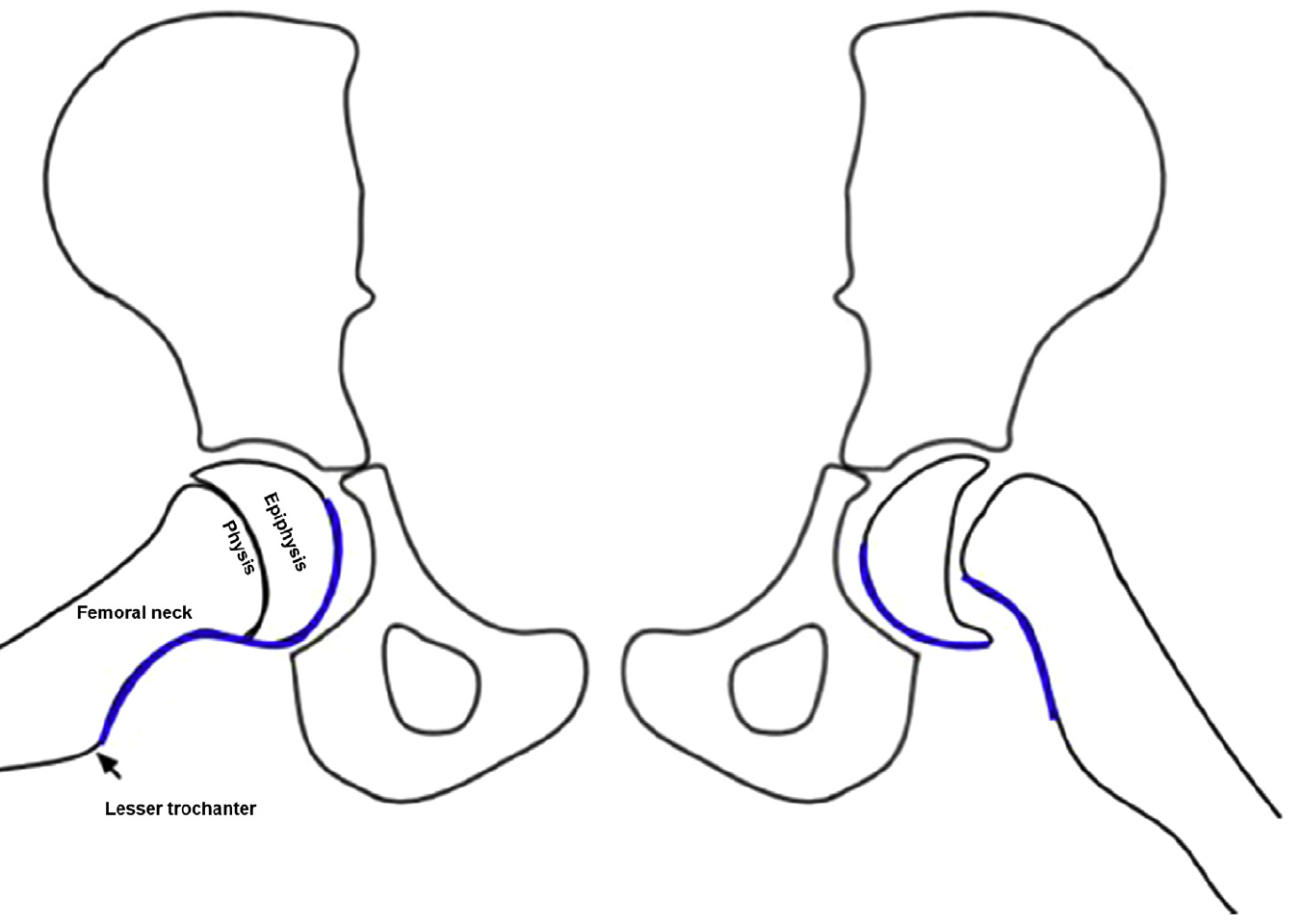
Slipped Capital Femoral Epiphysis (SCFE)
http://www.raymondliumd.com/images/SCFE%20illustrated%20and%20cropped.jpg
Early Diagnosis:
Klein’s Line on AP view
https://pedemmorsels.com/wp-content/uploads/2018/01/Slipped-Capital-Femoral-Epiphysis-3.png
Another virtual line may assist in diagnosis
S-sign
Klein's line and S-sign
Consider adding both of these virtual lines/signs to your review of the pediatric hip plain film
Pearl: consider desmopressin (DDAVP) for patients with an intracranial hemorrhage who are taking an antiplatelet. Caution, this is not for patients with an ischemic stroke with hemorrhagic conversion and it was not specifically evaluated for patients on anticoagulation or going to the OR with neurosurgery.
How strong is this evidence? International guidelines already give cautious approval for this practice, and now there is a retrospective review to support it. Though there were only 124 patients in the trial, the rate of hemorrhage expansion was much lower in the DDAVP group (10.9% vs 36.2%, P = .002) and there was no increased risk of hyponatremia (no events reported).
Adenosine is an atrioventricular nodal blocking agent that is commonly used in the treatment of supraventricular tachycardia. It is dosed as 6 mg IV Push x 1, followed by dose escalation to 12 mg IV Push if the initial dose was unsuccessful. In patients with central access or prior orthotopic heart transplantation, the initial recommended dose is 3 mg.
Due to its short half-life (< 10 seconds) it is imperative to administer in the most proximal access and follow with a 20 mL bolus of saline. Traditionally this is done using a two-way stopcock.
A new study compared single syringe (adenosine 6mg + 18 mL saline) vs two syringes (adenosine 6mg in one, 20 mL saline in the other) in 53 patients with SVT. The single syringe arm converted to NSR 73.1% after one dose compared to 40.7% in the two-syringe arm (p=0.0176). After up to three doses, the single syringe arm had 100% conversion compared to 70.4% in the two-syringe arm (p=0.0043).
Single syringe adenosine has been recommended in FOAM for several years. Although small, this study is the first to compare the two methods. This method simplifies administration and may improve cardioversion rates.
After many years of national shortage and FDA’s black box warning in 2001 (QT prolongation) droperidol is slowing becoming available.
In 2015, a prospective observational study was published involving ED patients who received droperidol for agitation (acute behavioral disturbance).
Method
Results
Four leading reason for ED presentation
Adverse events
Conclusion
Interventions Shown to Reduce Mortality in RCTs
Antibiotic stewardship has led various organizations such as the AAP, AAFP, and IDSA to introduce two different approaches to the treatment of acute otitis media (AOM):
Immediate treatment with antibiotics should always include the following patients:
The observation approach can be considered in the following very slect patient group:
Often the issue with pediatric AOM isn't necessarily the overprescribing of antibiotics, but the inaccurate/inappropriate over diagnosis of acute otitis media. An erythematous tympanic membrane does not equal AOM. Crying and fever can result in a red TM. Fluid seen behind the TM, is often just serous otitis media, which isn't AOM.
When antibiotics are warranted, first-line treatment is with high dose amoxicillin, 90 mg/kg per day divided into two doses; unless the child has received beta-lactam antibiotics in the previous 90 days and/or also has puruent conjunctivitis mandating amoxicillin-clavulanate instead. In the later case, prescribing the Augment ES, 600 mg/5mL formlation with a lower clavulanic concentration lessening GI upset and diarrhea is prefered.
Bottom Line: Fosphenytoin, valproate, and levetiracetaim have similar efficacy in treatment of benzodiazepine-resistant status epilepticus.
Settings
Study Results:
Discussion:
This study’s results differed from previous single center study (Girardis JAMA 2016) or meta analysis (Chu DK, Lancer 2018), which showed mortality benefit in patients with conservative oxygen (Girardis & Chu) and more ventilator-free days (Girardis).
Conclusion: Conservative oxygen did not significantly affect the ventilator free days of mechanically ventilated patients.
A ~55 year-old female with a history of ESRD and diabetes who presented to the ED with progressively worsening foot odor. An x-ray was performed. The picture below shows the right foot.
What is the diagnosis?

The role of skeletal muscle relaxants in the management of lower back pain in the ED
Patients with lower back pain (LBP) presenting to the ED are often treated with NSAIDs plus skeletal muscle relaxants.
A recent study in Annals of Emergency Medicine compared functional outcomes and pain in ED patients with acute non radicular LBP with 4 different treatment regimens.
Conclusion: Adding a muscle relaxant to ibuprofen did not improve pain or improve function at 1 week following an ED visit for LBP.
Note: Prior studies have found no benefit to adding opioids or diazepam to NSAIDs for ED patients with acute non radicular LBP
As of November 20, 2019:
2290 cases of e-cigarette, or vaping, product use-associated lung injury (EVALI) from 49 states (except Alaska), District of Columbia and 2 U.S. territories.
Analysis of 29 bronchoalveolar lavage (BAL) fluid samples from EVALI patients submitted to CDC from 10 states showed:
*** Vitamin E acetate appears to be associated with EVALI but the investigation is continuing.***
Some research has suggested that oral vitamin E use has potential beneficial effects (i.e. anti-inflammatory/antioxidant) in the lung (e.g. asthma and allergic lung disease), cardiovascular disease and prostate cancer (Cook-Mills JM et al. 2013; Jiang Q et al. 2001)
Common uses of vitamin E
There is limited to no data on pulmonary effect of vitamin E from inhalation in the scientific literature.
Stay tuned for additional updates from CDC.
Therefore, pain medications must be dosed carefully, which runs the risk of underdosing. Pain medications can also contribute to delerium, and decreased functional status.
Recommendations:
Streptococcal pharyngitis is common in the pediatric population however in children younger than 3 years, group A streptococcus (GAS) is a rare cause of sore throat and sequela including acute rheumatic fever are very rare. Inappropriate testing leads to increased healthcare and unnecessary exposure to antibiotics.
The national guidelines published by the Infectious Diseases Society of America do NOT recommend GAS testing in children less than the age of 3 years unless the patient meets clinical criteria and has a home contact with documented GAS.
Metformin is one of the most commonly prescribed oral hypoglycemic agents. Metformin associated lactic acidosis (MALA) is uncommon but potentially life-threatening complication of metformin overdose.
Lactic acidosis occurs due to inhibition of mitochondrial glycerophosphate dehydrogenase, resulting in decreased conversion of lactic acid to pyruvate.
A small retrospective study (using Illinois Poison Center data) attempted to characterize the development of MALA after an acute overdose.
MALA was defined as
Results
40 cases of MALA identified between Jan. 2001 to Dec. 2014
Time to development of MALA (n=30)
Death: 1 (2.5%)
Conclusion
When managing cardiac arrest, it is important to differentiate PEA, the presence of organized electrical activity without a pulse, from "pseudo-PEA,"where there is no pulse but there IS cardiac activity visualized on ultrasound.
Why:
How:
What:
Bottom Line: Pseudo-PEA is different from PEA. Utilize POCUS during your cardiac arrests to identify it and to help diagnose reversible causes, and treat it as a profound shock state with the appropriate supportive measures, i.e. pressors or inotropy.
Lateral hip pain is a common presentation of hip pain.
Typically seen in runners and women over the age of 40 who start unaccustomed exercise.
Pain from OA of the hip which is typically medial (groin pain)
Lateral hip pain has traditionally been diagnosed at trochanteric bursitis.
Research suggests that lateral hip pain may be multifactorial and better termed Greater trochanteric pain syndrome.
Pain from the gluteal medius and/or minimus due to non-inflammatory tendonopathy is likely causative. This may cause a secondary bursitis.
Pain is insidious, gradual worsens and is variable based on activity type.
Also, can be seen after a fall resulting in tearing.
Pain is described as a deep ache or bruise. It can stay localized or radiate down lateral thigh towards knee.
Patients report night/early morning pain and when rolling over onto the outer hip on affected side.
Fatigue from prolonged sitting, walking and single leg loading activities such as walking up stairs.
Provoking activities and postures cause compressive forces on the involved tendons.
These generally occur when the hip is adducted across midline such as with
Side sleeping,
Place pillow between legs to align pelvis and keep knee and hip in line
Crossed leg sitting
Sit w/ knees at hip distance and feet on floor
Selfie poses - Standing w a hitched hip (pushing hip to the side).
Attempt to correct biomechanical issues before progressing directly to bursal steroid injection
May only be a temporary fix if underlying issue not addressed.
A helpful clinical guide
https://bjgp.org/content/bjgp/67/663/479/F1.large.jpg?download=true
{kind=link}
{kind=link}
{kind=link}
{kind=link}