What is the cause of Mad honey poisoning?
Grayanotoxin
Grayanotoxin is a neurotoxin that is found in honey contaminated with nectar of Rhododendron plants. It binds to activated/open neuronal sodium channels and prevents inactivation of sodium channels. Case reports of mad honey poisoning is often reported in the eastern Black Sea region of Turkey. Commercial honey producers frequently mix honeys from multiple sources to decrease the grayanotoxin contamination.
Mad honey poisoning is rarely fatal and generally resolves within 24 hours. Commonly reported symptoms include dizziness, weakness, impaired consciousness/disorientation, excessive perspiration, nausea/vomiting, and paresthesia. In severe intoxication, patients can experience complete AV block, bradycardia/asystole, hypotension, and syncope.
Management is primarily supportive with atropine and IV fluids.
As the number of COVID-19 cases rises worldwide, prehospital and emergency department healthcare workers remain at high risk of exposure and infection during CPR for patients with cardiac arrest and potential SARS-CoV-2.
Existing evidence supports similar cardiac arrest outcomes in airways managed with a supraglottic airway (SGA) compared to endotracheal intubation (ETT).1 It is generally accepted that the best airway seal is provided with endotracheal intubation + viral filter, but how well do SGAs prevent spread of aerosols?
In CPR simulation studies:
The current COVID-19 pandemic and known aerosolized transmission has triggered many ED process changes, including the discouragement of utilizing nebulizers to administer inhaled bronchodilators such as albuterol for concern of spread. Historically, both patients and providers preferred the use of nebulizers as they are easier to use and the belief was that they were more effective than meterd dose inhalers. However, evidence based data has consistently shown that for both adult and pediatric patients that when MDI's are used WITH a spacer:
Albuterol: 2.5 mg nebulizer solution = 3-5 MDI puffs
Albuterol: 5 mg nebulizer solution = 5-10 MDI puffs
Ipratropium: 0.25 mg nebulizer solution = 2 MDI puffs
Ipratropium: 0.5 mg nebulizer solution = 4 MDI puffs
Transfer of chemical from their original container to an unlabeled or different container (e.g. Gatorade bottle) is one of the common causes of unintentional poisoning.
A retrospective study of National Poison Data System from 2007 – 2017 identified 45,512 cases of unintentional exposure/ingestion of chemicals contained in unlabeled/incorrectly labeled containers.
Result
Annual reported cases increased from 3,223 in 2007 to 5,417 in 2017.
Most commonly involved products included
These exposures led to
The majority of these exposures were non-toxic in nature (72%) but serious outcomes were noted in 4.4% of the cases, including 23 deaths.
Highest morbidity was associated with:
Deaths
Conclusion
Ulnar Collateral ligament injuries of the elbow
Overhead throwing athletes are at risk of insufficiency and rupture of the ulnar collateral ligament (UCL) of the elbow
This can lead to valgus instability similar to what can occur in the knee
Overhead throwing places a significant valgus stress on the elbow
Though classically seen in baseball pitchers, may also be seen in javelin throwers and other high velocity throwing sports
In the acute setting may be seen after an elbow dislocation
History includes a “pop” and medial elbow pain following throwing activities
In cases of overuse injury, athletes will report a progressive loss of velocity, accuracy, and/or endurance with throwing.
The ulnar collateral ligament is the primary restraint to valgus stress from 30 to 120 degrees of flexion
One classic test for UCL instability is the milking maneuver
Patient may be sitting or standing
Patient’s forearm is supinated and elbow flexed at 90 degrees
A valgus force is applied by pulling the patient’s thumb while the examiner’s other hand stabilizes the elbow and palpates the medial joint line.
Instability, pain or apprehension at the UCL is considered a positive test
https://www.youtube.com/watch?v=gbn24X_qqn0
N-acetylcysteine (NAC) is well known as the accepted antidote for acute acetaminophen (tylenol/paracetamol) overdose and is well studied for this indication. While the literature base is not nearly as strong in other causes of acute liver failure, NAC is increasingly used in these scenarios as well. In the emergency department in particular, the cause of fulminant hepatic failure is often not known. NAC may have some protective benefit in non-acetaminophen acute liver failure. Existing data do not show a mortality benefit to NAC in non-acetaminophen acute liver failure, but do show improvement in transplant-free survival. The AASLD guidelines (last revised in 2011) do not comment on NAC in non-acetaminophen acute liver failure. A common practice is to continue NAC until the INR is < 2 and AST/ALT have decreased at least 25% from their peak values.
Patients in fulminant liver failure should also be strongly considered for transfer to a center that does liver transplant, if presenting to a non-transplant center. The King's College criteria is the most commonly used prognostic score for determining need of transfer to a transplant center, but in addition to calculating a King's College score providers should generally consider consultation with a transplant hepatologist for any fulminant liver failure patient to discuss the risks/benefits of transfer for transplant evaluation.
Bottom Line: While not as strongly indicated as it is in acute acetaminophen induced liver failure, NAC should be considered in both non-acetaminophen liver failure and liver failure of unknown etiology. In addition, strongly consider consultation with a transplant hepatologist in any case of fulminant hepatic failure.
A labial adhesion is defined as a thin avascular clear plane, a raphe, between the labia minora. These adhesions which can be caused by minor trauma or infection in the absence of estrogen can cause varying degrees of obstruction.
Dihydropyridine (calcium channel blocker) overdose is one of the leading causes of death from cardiovascular drug poisoning. In contrast, angiotensin-II receptors blockers (ARBs) and angiotensin converting enzyme inhibitor (ACEIs) causes minimal toxicity in overdose. Frequently, these medications are co-ingested with dihydropridines.
Recently, a retrospective study was conducted to evaluate the hemodynamic impact of dihydropyridines with ARBs/ACEIs co-ingestion.
Results
Cohort
Mixed overdose group had:
Higher proportion of the mixed overdose group received:
Conclusion
Combined overdose of dihydropyridines with ARBs/ACEIs can result in more significant hypotension.
| Central Nervous System | Peripheral Nervous System | |
| Pattern of Symptoms | • Hemibody involvement • Weakness of UE extensors • Weakness of LE flexors | • Distal involvement in polyneuropathy • Distal and proximal involvement in polyradiculoneuropathy • Proximal involvement in polyradiculopathy • Sensory often precedes motor symptoms • Pure proximal>distal weakness may be due to myopathy or NMJ disorder |
| Sensory Symptoms | • Central poststroke pain (hyperalgesia, allodynia) • Sensory level in spinal cord pathology • Proprioception involved early in dorsal column disorders | • Neuropathic pain (burning, tingling, shock-like) • Ascending sensory loss involving distal BLE>BUE in polyneuropathy • Proprioception involved late in polyneuropathy |
| Reflexes | • Hyperreflexia in affected limb(s) after acute period • Positive Babinski’s sign | • Hyporeflexia in affected limb(s) |
| Tone | • Increased after acute period | • Decreased |
Blood Pressure Management in Acute Ischemic Stroke
Carpal Tunnel Syndrome (CTS)
The hallmark of classic CTS: pain or paresthesia (numbness and tingling) in a distribution that includes the median nerve territory, with involvement of the first three digits and the radial half of the fourth digit.
The symptoms of CTS are typically worse at night and often awaken patients from sleep.
Fixed sensory loss is usually a late finding
Involves the median-innervated fingers BUT spares the thenar eminence.
This pattern occurs because the palmar sensory cutaneous nerve arises proximal to the wrist and passes over, rather than through, the carpal tunnel.
Consider a more proximal lesion in cases involving sensory loss in the thenar eminence
Example: pronator syndrome
Nitroglycerin is a potent vasodilator used most commonly for the treatment of angina and ACS. It can also be administered as a continuous infusion for acute management of a hypertensive emergency or sympathetic crashing acute pulmonary edema.
Most are aware of asking men for history of medications for erectile dysfunction (PDE5 inhibitors: sildenafil, tadalafil, vardenafil) but many overlook the fact that men and women may be on these medications chronically for pulmonary hypertension. Men can also be on these medications for the treatment of BPH. Be broad in your history taking and do not limit the discussion to erectile dysfunction or a specific gender.
Drug interaction:
-PDE5 inhibitors prevent the breakdown of cGMP
-Nitrates are nitric oxide donors that increase the production of cGMP
-The combination can lead to excessive vasodilation
If accidentally co-administered:
There is no antidote for this medication error. Support the patient with Trendelenburg positioning, fluid administration, and if needed, vasopressors such as norepinephrine until blood pressure stabilizes.
How long should you wait to administer nitrates after a patient takes a PDE5 Inhibitor?
Sildenafil and vardenafil: 24 h after last dose*
Tadalafil > 48 h after last dose*
*Even if acute ACS event
Acute appendicitis is the most common etiology requiring urgent abdominal surgery in children in the United States. Peak incidence occurs in the second decade of life, with male patients being more commonly affected than female patients. Classic manifestations of appendicitis occur in school-aged children and adolescents, but are often absent in younger children. Infants and young children <5 years are more likely to present with nonspecific or atypical findings, resulting in delays in diagnosis and higher rates of perforation.
Diagnosis is aided by clinical factors, lab findings, and ultrasound (+/- CT or MRI if ultrasound is equivocal).
Historically, the standard of care for acute appendicitis has been urgent operative management. However, in the past several years, there has been increasing literature supporting nonoperative management (antibiotics only) in adult patients with acute uncomplicated appendicitis. Additionally, there is a growing body of evidence demonstrating the safety and efficacy of nonoperative management for uncomplicated appendicitis in children.
Hartford and Woodward provide a review of the current literature on the nonoperative management of uncomplicated appendicitis in children. They conclude:
- The majority of recent prospective studies demonstrate early treatment success (0-30 days) of approximately 90% in pediatric patients undergoing nonoperative management.
- Factors associated with failure of nonoperative management in pediatric appendicitis: longer duration of symptoms (>48 hours), younger age (<5 years), and presence of appendicolith.
- Nonoperative management has been associated with
o Lower healthcare costs at 1 year
o Fewer disability days at 1 year
o No significantly different rate of complicated appendicitis
- Most trials to date involve a 24-48 hour initial course of broad spectrum IV antibiotics followed by oral antibiotics for a total of >/= 7 days as nonoperative management. Currently, there is no consensus on antibiotic regimen.
Bottom Line: Given the current evidence, nonoperative management may be a viable treatment option for low risk pediatric patients with uncomplicated appendicitis. The literature is not conclusive, thus we as medical providers in conjunction with our surgical colleagues, should consider numerous factors when discussing treatment options for acute appendicitis with patients and their families.
Historically, there has been debate on transporting outside hospital cardiac arrests, as well a trauma, with the question of whether to "scoop and run" or "stay and play".
Could hasty transportation of cardiac arrest patients put a damper on resuscitation quality?
A recent propensity-matched study in JAMA analyzed 192 EMS agencies across 10 N American sites.
Methods:
-Resuscitation Outcomes Consortium Cardiac Epidemiologic Registry, which counted 43,969 consecutive cases of nontraumatic adult EMS-treated OHCA (median age 67, 37% of whom were women) in 2011-2015.
-25% of these patients were transported to the hospital
-Matched 1:1 with patients in refractory arrest who were resuscitated on scene
-Primary outcome was survival to hospital discharge, secondary outcome survival to hospital discharge with a favorable neurological status
Results:
-Duration of out-of-hospital resuscitation was only 6 minutes longer in the intra-arrest transport group (29.1 and 22.9 minutes; not a statistically significant difference)
-Survival to hospital discharge was 3.8% for patients who underwent intra-arrest transport and 12.6% for those who received on-scene resuscitation
-In the propensity-matched cohort, which included 27,705 patients, survival to hospital discharge occurred in 4.0% of patients who underwent intra-arrest transport vs 8.5% who received on-scene resuscitation (risk difference, 4.6% [95% CI, 4.0- 5.1])
-Favorable neurological outcome occurred in 2.9% of patients who underwent intra-arrest transport vs 7.1% who received on-scene resuscitation (risk difference, 4.2% [95% CI, 3.5%-4.9%])
-Intra-arrest transport during resuscitation was associated with worse odds of survival to hospital discharge compared to on-scene resuscitation (4% vs 8.5%, RR 0.48, CI 0.43-0.54)
-Findings persisted across subgroups of initial shockable rhythm vs. non-shockable rhythms (most common initial rhythm was aystole), as well as EMS witness arrests vs. unwitnessed arrests
Conclusion:
-This study does not support the routine transportation of patients in cardiac arrest during rescuscitation.
-The neurologically intact survival benefit associated with on-scene resuscitation is both impressive and intriguing.
-However, what implications could this have on ECPR?
Limitations:
-Potential bias due to observational nature of study
-Duration of resuscitations very similar, unknown exactly how long transport times were or if this was in urban or rural populations
-External validity not generalizable due to heterogeneity of patient populations and EMS systems
-Further randomized clinical trials are required
Physical injury patterns associated with physical elder abuse
Elder abuse is both common and underrecognized
Between 5 and 10% of US older adults are victims of elder abuse annually
For many older adults, contact with a health care provider may represent their only contact outside the home
Differentiating physical elder abuse from unintentional trauma can be very difficult
A recent study compared these two groups with a case-control design
Study cases: 100 successfully prosecuted physical elder abuse cases from a single urban ED
Physical abuse victims were more likely to have:
Bruising (78% vs. 54%)
Injuries to maxillofacial, dental or neck region (67% vs. 28%)
Particularly the LEFT side
Neck injuries 6x more common is assault
Ear injuries occurred in assault but not in falls
Absence of fracture (8% vs. 22%)
Less likely to have lower extremity injuries (9% vs. 41%)
22% of victims had no visible injuries
Most common mechanism assault with hands or fists and pushing or shoving causing a fall
Take home: Consider elder abuse especially in cases of the above red flags
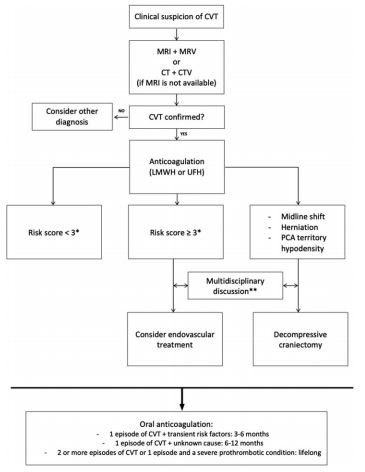
Bottom Line: Severity of CVT presentation depends on the location and clot burden. Anticoagulation is key, though consider endovascular intervention if patient does not improve or deteriorates despite anticoagulation.
A retrospective study analyzed data from 757 patients with spontaneous intraparenchymal hemorrhage.
Within the first 6 hours of admission, patients who had systolic blood pressure reduction between 40 – 60 mm Hg (OR 1.9, 95% CI 1.1-3.5) or reduction ≥ 60 mm Hg (OR 1.9, 95%CI 1.01-3.8) were associated with almost double likelihood of poor discharge functional outcome (defined as modified Rankin Scale 3-6).
Additionally, large systolic blood pressure reduction ≥ 60 mm Hg in patients with large hematoma (≥ 30.47 ml) was associated with higher likelihood of very poor functional outcome (mRS 5-6).
Take home points: while more studies are still needed to confirm these observations, perhaps we may not want to drop blood pressure in patients with spontaneous intraparenchymal hemorrhage too much and too fast.
Systematic review and meta-analysis of 5 studies with a total of 929 patients comparing early vs. late initiation of norepinephrine in patients with septic shock
Primary outcome:
Secondary outcome:
Caveat:
Take home point:
Early norepinephrine usage may improve mortality in septic shock
- Urethral prolapse will appear as a protrusion of the distal urethra through the urinary meatus causing a “doughnut” sign.
- Risk factors include trauma, UTI, anatomical differences, and increased intraabdoiminal pressure from cough or constipation. There is a higher incidence in people of African descent.
- The chief complaint may include urethral mass and vaginal bleeding.
- There is a bimodal age distribution (prepuberty and postmetapause) due to a relative estrogen deficiency.
-Treatment is with estrogen cream and sitz baths for 4- 6 weeks.