With ED-boarding of critically-ill patients becoming more common, it is likely that ED physicians may find themselves caring for a patient who develops ACS – that is, abdominal compartment syndrome. While intraabdominal hypertension (IAH) is common and is defined as intraabdominal pressure > 12 mmHg, ACS is defined as a sustained intraabdominal pressure > 20mmHg with associated organ injury.
WHY you need to know it:
ACS → Increased mortality & recognition is key to appropriate management
WHO is at risk:
HOW it kills:
→ Lactic acidosis, respiratory acidosis, multisystem organ failure, cardiovascular collapse & death
WHEN to consider it:
WHAT to do:
Bottom Line: Abdominal compartment syndrome is an affliction of the critically ill, is assosciated with worsened mortality, and requires aggressive measures to lower the intraabdominal pressure while obtaining emergent surgical consultation for potential emergent laparotomy.
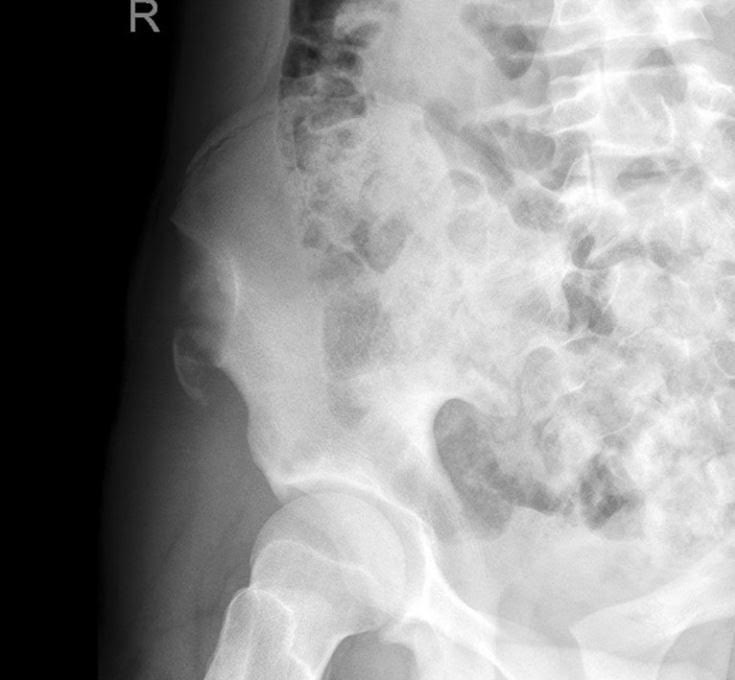
A 15 y.o. female presents to your emergency department with sudden onset hip pain after winding up to kick a soccer ball during her game today. You see a well-developed female in obvious discomfort, with tenderness to palpation over her lateral hip and pain with passive ROM at the hip. You obtain this x-ray. What is your diagnosis?
Metformin associated lactic acidosis (MALA) has a high rate of mortality, ranging from 25% to 50%. Lactate level and acidemia are frequently associated with poor clinical outcome in many disease/medical conditions (e.g. sepsis).
A study investigated, via meta-analysis, if lactate level and pH were predictive of mortality in MALA.
Results
44 studies were identified from PubMed, EMBASE and Web of Science.
170 cases of MALA were included
pH and lactate were poor predictors of mortality based upon ROC curve
Conclusion
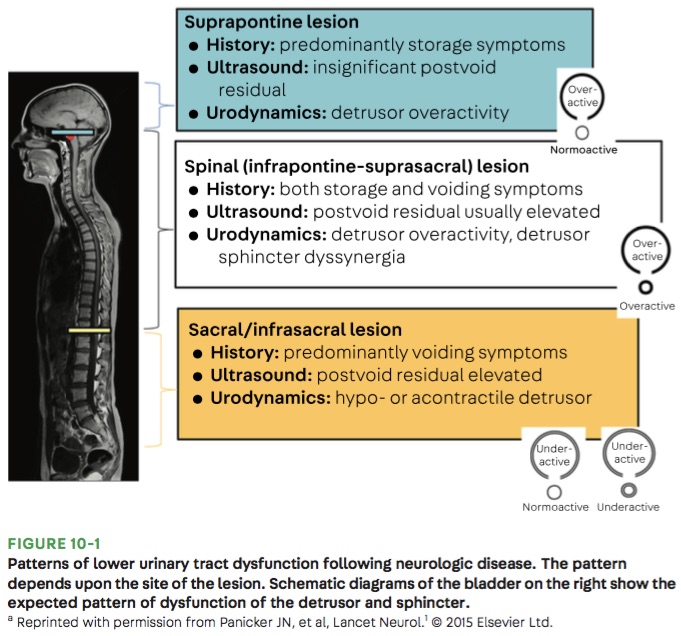
Bottom Line: Urinary retention can be seen with neurological injury involving the lower brainstem, spinal cord, cauda equina, and peripheral nerves.
Don't forget cerebral fat embolism syndrome (FES) on the differential for altered trauma patients. FES is typically associated with long bone fractures, but has been reported with other fractures, orthopedic reaming (i.e. aggressive orthopedic procedures), and in rare cases even with non-fracture (soft-tissue) trauma. Typically symptoms occur between 24 and 72 hours after injury, but there have been cases both earlier and later. Diagnosis is clinical, but MRI may be helpful, and will often show multiple cerebral white matter lesions. It is debated whether FES is truly an embolic phenomena (i.e fat molecules traveling to and blocking blood supply of organs), or rather an inflammatory response to free fatty acids in the blood stream (i.e. more of a vasculitis type pathology). Management is supportive care, but give these patients time as there can be favorable outcomes, even after prolonged coma.
Taking an accurate history to diagnose Cauda Equina Syndrome (CES)
Classic teaching is to inquire specifically about bowel and bladder function, sexual dysfunction, and/or loss of sensation in the groin.
Rather than asking about urinary incontinence, clinicians should ask specifically about difficulty passing urine, new leakage and retention.
Discussing issues related to sexual dysfunction are difficult for both clinicians and patients.
Rather than asking if there are any issues with sexual function, a more direct and informative way would be to ask if the patient has a “change in ability to achieve an erection or ejaculate” or “loss of sensation in genitals during sexual intercourse.”
Saddle anesthesia has the highest predictive value in diagnosing MRI-proven CES. Loss of sensation may be incomplete and patchy. Ask about change in sensation with wiping after a bowel movement.
The new IDSA and American Thoracic Society guidelines for community acquired pneumonia were recently released. Major updates to the guidelines include but are not limited to:
1. It is not recommended to obtain sputum cultures in routine care. Consider only in patients who are intubated or empirically being treated for hospital associated pathogens such as MRSA or P. aeruginosa.
2. Blood cultures are only recommended for severe CAP managed in the hospital or those empirically being treated for MRSA or P. aeruginosa, or prior infection with those pathogens, or hospitalized and received parenteral antibiotics in the last 90 days.
3. Test for influenza during time periods when influenza is prominent (as in our current 2020 influenza outbreak).
4. Healthy patients can receive either amoxicillin 1g TID, doxycycline 100mg BID, or azithromycin 500mg followed by 250mg daily x 4 doses.
5. Patients with comorbidities such as chronic heart, lung, liver, or renal disease, diabetes, alcoholism, malignancy, or asplenia should receive combination therapy with a beta-lactam (amoxicillin/clavulanate, cefdinir, or cefpodoxime) + azithromycin or doxycycline. If allergies preclude the use of a beta-lactam, a fluoroquinolone (levofloxacin or moxifloxacin) can be used.
6. Patient admitted for non-severe CAP can receive combination beta-lactam (ampicillin/sulbactam, or ceftriaxone) and azithromycin therapy. Patients with severe beta-lactam allergies can receive either levofloxacin or moxifloxacin).
7. It is no longer recommended to add anaerobic coverage for suspected aspiration pneumonia unless the patient is suspected to have a lung abscess or empyema. It is most likely a chemical pneumonitis and should resolve within 24-48 hours with supportive therapy.
Dr. Bryan Hayes wrote a Pearl 10/4/2013 to remind us autoimmune encephalitis can present like neuroleptic malignant syndrome.
Dr. Danya Khouja wrote a Pearl 6/28/2017 to inform us autoimmune encephalitis is associated with tumors and can be investigated with serum and CSF antibody panels.
Since those publications, the number of validated autoimmune biomarkers in these panels has increased dramatically. In 2020 we now know, autoimmune encephalitis is at least as common as infectious encephalitis.
Here is how to diagnose it
1. Suspect the diagnosis in patients with subacute/rapidly progressive altered mental status, memory loss, or psychiatric symptoms. It can be mistaken for a new diagnosis of schizophrenia or bipolar disorder.
2. Look for one or more additional findings: new seizures, focal CNS findings, CSF pleocytosis, MRI findings
3. Exclude other likely etiologies (but try not to get hung up on a positive drug test, especially if drug use was not recent).
Why is this important?
Early treatment with steroids and plasmapheresis can prevent progression of disease (prevent seizures, prevent months-long hospitalizations).
Young girls are especially likely to have teratomas as a cause for the disease. Finding and resecting those tumors is life-saving.
Timeliness of Concussion Referral
Do patients with a self-limited diagnosis of “concussion” require specialty follow up?
If so, is there a benefit to earlier evaluation?
Recently published research from the University of Pittsburgh Sports Medicine Concussion Program suggests so.
Subjects: 162 concussed athletes between the ages of 12 and 22
Findings: Athletes treated in the first week after injury recovered faster than those who did not receive care until 8 to 21 days post injury.
Note: Once in care the length of time spent recovering was the same for both groups. This suggests that the amount of time prior to the initiation of care may explain the longer recovery time of the 2nd group.
Earlier recovery can help minimize effects on mood, quality of life and lost time in school/work.
Take home: Consiuder early follow up referral to a qualified provider for all concussed patients seen in the ED
Intentional drug overdose (IDO) can lead to significant morbidity and can increased patient's risk of death. A study was recently performed to identify the predictors of death in a cohort of patient who intentionally overdose on drug(s).
National Self-Harm Registry and National Drug-Related Death Index were reviewed (between January 1st, 2007 and December 31st, 2014) to identify the study cohort.
Results
|
| Non fatal IDO | Fatal IDO |
| Number of cases | 63,831 | 364 |
| Incidence | 148.8/100,000 | 1.01/100,000 |
| Male | 42.0% | 55.2% |
| Age, years (median) | 35 | 44 |
| Multiple drug ingestion | 48.5% | 78.3% |
Risk of death
Conclusion
Mechanical Ventilation Pearls for Acute Ischemic Stroke
Tonsillectomy and adenoidectomy (T&A) is the second most common ambulatory surgery performed in the US. Children younger than 3 years, children with craniofacial disorders or sleep apnea are typically admitted overnight as studies have shown an increase rate of airway or respiratory complications in this population.
The most common late complications include bleeding and dehydration. Other complications include nausea, respiratory issues and pain.
Post-operatively, the overall 30-day emergency department return rate is up to 13.3%. Children ages 2 and younger were more likely to present to the ED. There is significantly higher risk of dehydration for children under 4 years. Children over the age of 6 had significantly higher bleeding risk and need for reoperation for hemorrhage control.
Many patients are treated in the emergency room for non-fatal opioid overdose. However, it is unknown what proportion of these patient population experience subsequent fatality after their ED visit.
A recent study investigated the 1-year mortality rate among Massachusetts ED patients who were treated and discharged from ED for non-fatal opioid overdose.
Results
Of those who died,
Manner of death
Place of death
Conclusion
Settings: multicenter, double-blind, phase 3 trial (apparently vitamin D worked in phase 2 trials).
Study Results:
Discussion:
Conclusion:
Early administration of high dose vitamin D did not improve 90-day all cause mortality.
Known effects and side effects of prescribed medicines may masquerade as cauda equina syndrome (CES) .
Analgesic medicines used by patients with chronic back pain may also cloud the diagnosis of CES.
Cholinergic medications (glaucoma/myasthenia) may lead to voiding issues.
Anticholinergic medications (COPD/urinary incontinence) may lead to urinary retention.
Opioids – Constipation, reduced bladder sensation
Anticonvulsants (Gabapentin/Pregabalin)- Urinary incontinence
Antidepressants (Amitriptyline) – Urinary retention, sexual dysfunction, reduced awareness of need to pass urine
NSAIDs – Urinary retention.
Adequate treatment of adrenal crisis (AC) is often delayed, even when a h/o adrenal insufficiency is known.
Besides refractory hypotension, also consider in pts with:
Beware of triggers:
Treatment:
Influenza is a common cause of community-acquired pneumonia and invasive bacterial coinfection may occur. In addition, secondary bacterial pneumonia due to MRSA is becoming more prevalent. Due to the higher incidence of MRSA, it is recommended that antibiotics with activity against MRSA (vancomycin or linezolid) be included in the empiric treatment regimen, especially if the patient is critically ill.
Take Home Point: Don’t forget to add MRSA coverage to your empiric treatment regimen in those influenza patients with severe disease or secondary bacterial pneumonia.
Pharmacobezoars (clumps of medication/pills) formation has been demonstrated in few medications such as aspirin, and ferrous sulfate tablets. Their presence can alter management due to prolonged absorption and may cause GI obstruction.
Acetaminophen (APAP) is a commonly available over-the-counter medication that is often implicated in an acute overdose event. A recently published in-vitro study (using pig stomach) investigated whether APAP can form a pharmacobezoar.
APAP group/dosage
Positive control group
Negative control group
Results
Conclusion
The arrival of a critically ill pregnant patient to the ED can be anxiety-provoking for emergency physicians as two lives and outcomes must be considered.
Some basic tenets of care, regardless of underlying issue, include:
Finally, once critical illness is identified the OB and NICU teams should be consulted immediately. Fetal distress in a viable pregnancy may be an indication for delivery, and initiation of the transfer process should occur if the supportive specialties are not in-house.