The New England Journal of Medicine and Lancet both published studies evaluating idarucizumab for reversal of dabigatran. It is a monoclonal antibody fragment that binds dabigatran with high affinity. Dr. Ryan Radecki summarizes the two articles on his EM Lit of Note blog.
Here are a few take home points from these early studies:
Cerebrospinal Fluid (CSF) Shunts
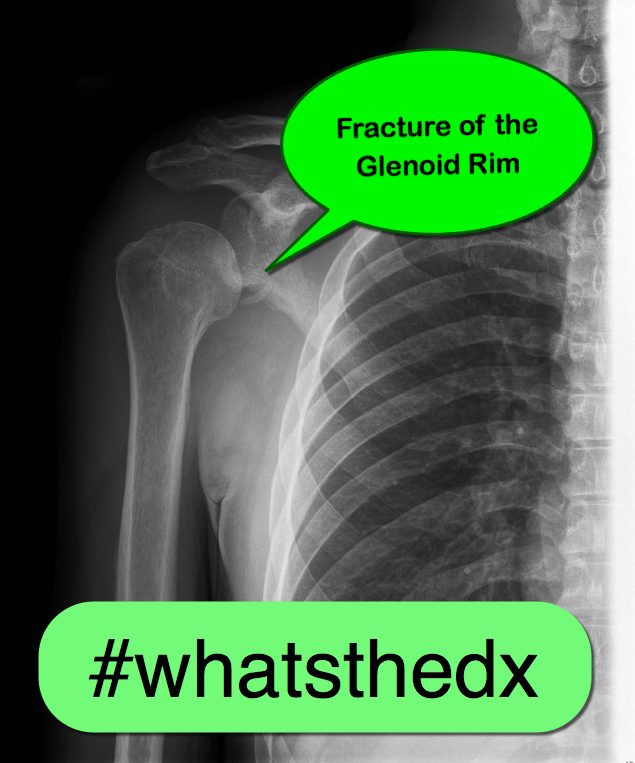
15 year-old female field hockey player presents with left shoulder pain. Besides fatigue over several weeks, she has no past medical history and there is nothing remarkable on physical exam. What's the diagnosis?
Transitioning Diabetic Ketoacidosis (DKA) patients off an insulin infusion can be challenging. If a long-acting insulin, such as glargine or levemir, is not administered at the correct time to provide extended coverage, patients can revert back into DKA.
Pilot Study
A prospective, randomized, controlled pilot study in 40 patients evaluated administration of glargine within 2 hours of insulin infusion initiation compared to waiting until the anion gap (AG) had closed.
What they did
What they found
Mean time to closure of AG, mean hospital LOS, incidents of hypoglycemia, rates of ICU admission, and ICU LOS were all similar between the groups.
Application to Clinical Practice
Although just a pilot study (using a convenience sample), early glargine administration seemed to be absorbed adequately (based on time to AG closure) and was not associated with increased risk of hypoglycemia. If confirmed in a larger study, this technique could help optimize care of DKA patients in the ED by eliminating the often-mismanaged transition step later on.
As noted in a previous pearl (see 1/7/2015), tuberculosis (TB), caused by Mycobacterium tuberculosis, is the second greatest infectious killer after HIV/AIDS globally. While the incidence and death rate from TB is decreasing, it is still a widespread problem.
Mycobacterium tuberculosis primarily attacks the lungs. However, it can attack any part of the body such as the kidney, spine, and brain. TB is primarily spread person to person through the air, for example when a person with TB coughs, sneezes, speaks, or sings.
Once a person is infected with TB, the likelihood of developing disease is greater if the person:
Classic symptoms for pulmonary TB include:
Other TB symptoms can also include:
Bottom line
In the emergency department, maintain a strong clinical awareness for tuberculosis for someone with night sweats, cough, chest pain, and intermittent fever lasting for 3 weeks or longer. In particular, consider this diagnosis for someone from a low- or middle-income country or if he or she is HIV positive.
Next time: Testing and treatment for TB.
Also see prior pearls on TB: Multidrug Resistant Tuberculosis (MDR TB) (1/21/2015), Tuberculosis (1/7/2015); XDR Tuberculosis (8/14/2013); PPD positive? Good news... (2/6/2013)
With a new academic year starting, it is important to review some details on central lines
Complications of central lines (TLC-Triple lumen catheter)
Avoiding infections: hand hygiene, chlorhexidine skin antisepsis, maximal barrier precautions, remove unnecessary lines, full gown and glove w/ mask and sterile technique.
Catheter position: 16-18cm for Right sided and 18-20 cm for Left sided. But can vary based on height, neck length, and catheter insertion site. Approximate length based on these factors.
Flow rates: Remember that putting in a central line does not necessarily improve your flow rates in resuscitation
16 G IV: 220 ml/min
Cordis/introducer sheath: 126 ml/min
18 G IV: 105 ml/min
16G distal port TLC: 69 ml/min
Ports (Can vary with type of catheter)
1. Distal exit port (16G)
2. Middle port (18G)
3. Proximal port (18G)
Arterial puncture: hold pressure for 5 mins and evaluate for hematoma formation (harder for subclavian approach)
Arterial cannulation: Has decreased due to ultrasound use but if you do cannulate an arterial site, don’t panic. Don’t remove the line. You can check a blood gas or arterial pulse waveform to confirm placement. Call vascular surgery for open removal and repair or endovascular repair. You could potentially remove a femoral arterial line and hold pressure but seek vascular advice regarding possible closure devices to use after removal.
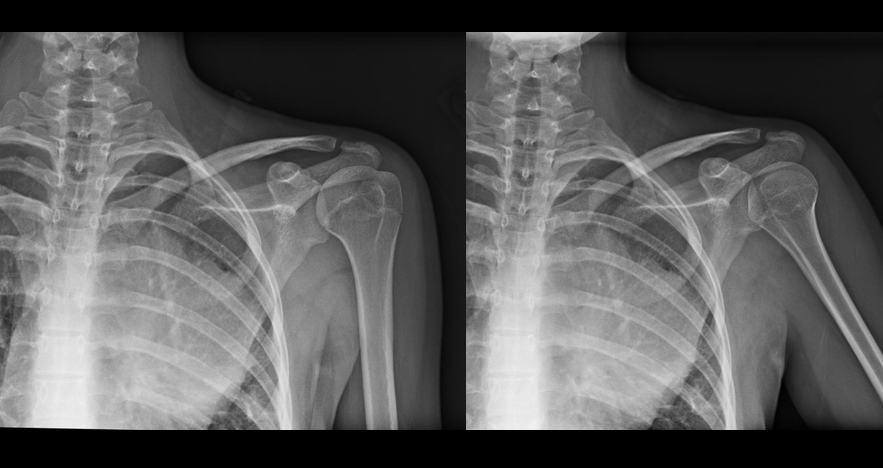
25 year-old male falls from 10 feet and lands on his right shoulder, what's the diagnosis?

Giant Cell Myocarditis
Giant cell myocarditis (GCM) is an infrequent, but often fatal form of acute myocarditis that has been shown to respond to cyclosporine-based immunosuppressive therapy
Even after heart transplantation GCM recurrence in the donor heart has been cited as high as 20% to 25%
Patients are surviving longer without transplantation because of efficacious medical therapy
A multi-institutional prospective data set revealed several novel findings in GCM:
· Long-term immunosuppression appears capable of lengthening transplantation-free survival ~19 years beyond initial diagnosis
· Cessation and/or reduction of immunosuppression are associated with GCM recurrence
· Patients who developed cyclosporine associate renal failure were able to be switched to a sirolimus-based regimen
Colles fracture
Almost 90% of distal radius fractures
Mechanism: Fall on the outstretched, hyperextended, radially deviated wrist with the forearm in pronation
Often seen in older patients and in those with osteoporosis
Distal radius fracture with dorsal angulation/displacement and/or radial shortening. "Dinner fork deformity"
https://en.wikipedia.org/wiki/Colles'_fracture#/media/File:Colles_fracture.JPG
Smith fracture (aka reverse Colles fracture)
Mechanism: Fall on the outstretched, flexed, radially deviated wrist with the forearm in pronation
Usually younger patients with high energy mechanism
Distal radius fracture with volar angulation or volar displacement. "Garden spade" deformity
Often unstable requiring ORIF
http://www.radiologyassistant.nl/data/bin/w440/a50979780ec887_Smith'-tek.jpg
Radial styloid fracture aka Chauffeur fracture
Fall causing compression of scaphoid against the styloid with wrist in dorsiflexion and ulnar deviation
Often associated with intercarpal ligamentous injuries (i.e., scapholunate dissociation, perilunate dislocation)
Often requires ORIF
http://images.radiopaedia.org/images/611818/cc52cce7bcfd8c905bcc7b5d2b6a65.jpg
30 year-old patient presents with palpitations. A parasternal long-axis clip is shown below along with the rhythm strip. What's the diagnosis and what drug was given during this clip?

Steroid Use in the treatment of Acute Sciatica
Have you used oral steroids in the treatment of your patient with acute sciatica thought to be secondary to a herniated disk.
Well a recent randomizaed, double-blind, placebo-controlled trial from 2008 to 2013 in a large integrated health care system in Northern California enrolled 269 patients to look at whether steroids improved pain or function. The intervention arm (twice as large as placebo arm) received a tapering 15-day course of oral prednisone (5 days each of 60 mg, 40 mg, and 20 mg; total cumulative dose = 600 mg; n = 181).
In the end there were no differences in surgery rates at 52-week follow-up, and the steroid arm had a modest improvement in function but no improvement in pain. There were also more adverse events at 3-week follow-up in the prednisone group than in the placebo group.
Conclusion: Giving steroids for acute sciatica does not appear to improve the patients pain, only has a modest improvement in function, and was associated with more adverse events. Put another way there was minimal benefit and more harm.
You can check out the full article at http://jama.jamanetwork.com/article.aspx?doi=10.1001/jama.2015.4468
Sodium valproate (VPA) had been studied and found to be effective in the adult population for migraines, but not in the pediatric population. This article was a small (12 patient) retrospective study of pediatric migraine patients looking at pain scores before and after VPA administration. Prior to VPA, patients received NSAIDs, dopamine antagonists, IV fluids and narcotics. Mean pain reduction prior to VPA was 17%. After VPA, pain scores were reduced by an additional 36%.
Recently, there has been a surge in synthetic cannabinoid in the U.S., including the Baltimore area. According to U.S. poison control center data, there has been 229% increase in calls related to SC between January to May of 2015 compared to similar time period in 2014.
The most commonly reported adverse/clinical effects included:
End-organ injuries have been also reported in case reports, including AKI, seizure, MI, and CVA.
Synthetic cannabinoid includes a list of chemical compounds that are structurally different compared to THC – the active compound in marijuana. However, they possess full CB1 (cannabinoid) receptor agonism effect, unlike the THC, which is a partial CB1 receptor agonist.
These chemicals (particularly JWH series) were originally synthesized to study the effect of cannabinoid receptors. Overall, it is difficult to identify the compound and the dose within each packets of SC.
Commonly marketed names include: Spice, K2, K9, herbal highs, Scooby snax, WTF.
Table. Identified synthetic cannabinoids
| Chemical name | Chemical origin |
| JWH-018; JWH-073; JWH-250 | Laboratory of J.W. Huffman |
| CP47,497; CP47,497-C8; CP59,540; cannabicyclohexanol | Pfizer laboratory |
| HU-210 | Hebrew University laboratory |
| Oleamide | Fatty acid |
| UR-144 | CB2 receptor agonist |
| XLR-11, AKB-48, AM-2201, AM-694 |
|
Management: Majority of the patients with acute SC intoxication mostly requires supportive care, including benzodiazepine for acute agitation. However, ED providers should be mindful of potential end-organ injury.
While most infections from parasites are associated with poor communities in low-income countries, there are still some important parasitic infections found in the United States.
The U.S. Centers for Disease Control and Prevention (CDC) has identified 5 parasitic diseases as priorities for public health action based upon:
These are
Bottom line:
Remember to keep your differential broad and maintain awareness of these generally unusual but important infections.
Renal Resuscitation using Renal Interlobar Artery Doppler (RIAD)
Shocked patient…. check! Adequate volume resuscitation…. check! Vasopressors.… check! Mean arterial pressure (MAP) > 65 mmHg….. check! Adequate urine output…. Wait, why isn’t my patient making urine?
As we begin to understand more about shock, hemodynamics, and the importance of perfusion over the usual macrocirculatory goals (MAP > 65), finding ways to assess regional blood flow is critical. A recent study examined the effect of fluid administration on renal perfusion using renal interlobar artery Doppler (RIAD) to assess the interlobar resistive index (RI). See how to perform a RIAD here.
They also recorded the fluid challenge’s effect on the traditional hemodynamic measurements of MAP and pulse pressure (PP) then observed the patient’s urine output (as a clinical marker of perfusion). The authors reported 3 key findings:
Bottom Line: The use of ultrasound to determine intrarenal hemodynamics is an interesting strategy to guide renal resuscitation in the shocked patient. There is mixed data on the use of RIAD, however this study could explain the findings of SEPSISPAM and also addresses the growing concern that traditional hemodynamic goals may be inadequate resuscitation targets.
References
For more critical care & resuscitation pearls, follow me on Twitter @JohnGreenwoodMD
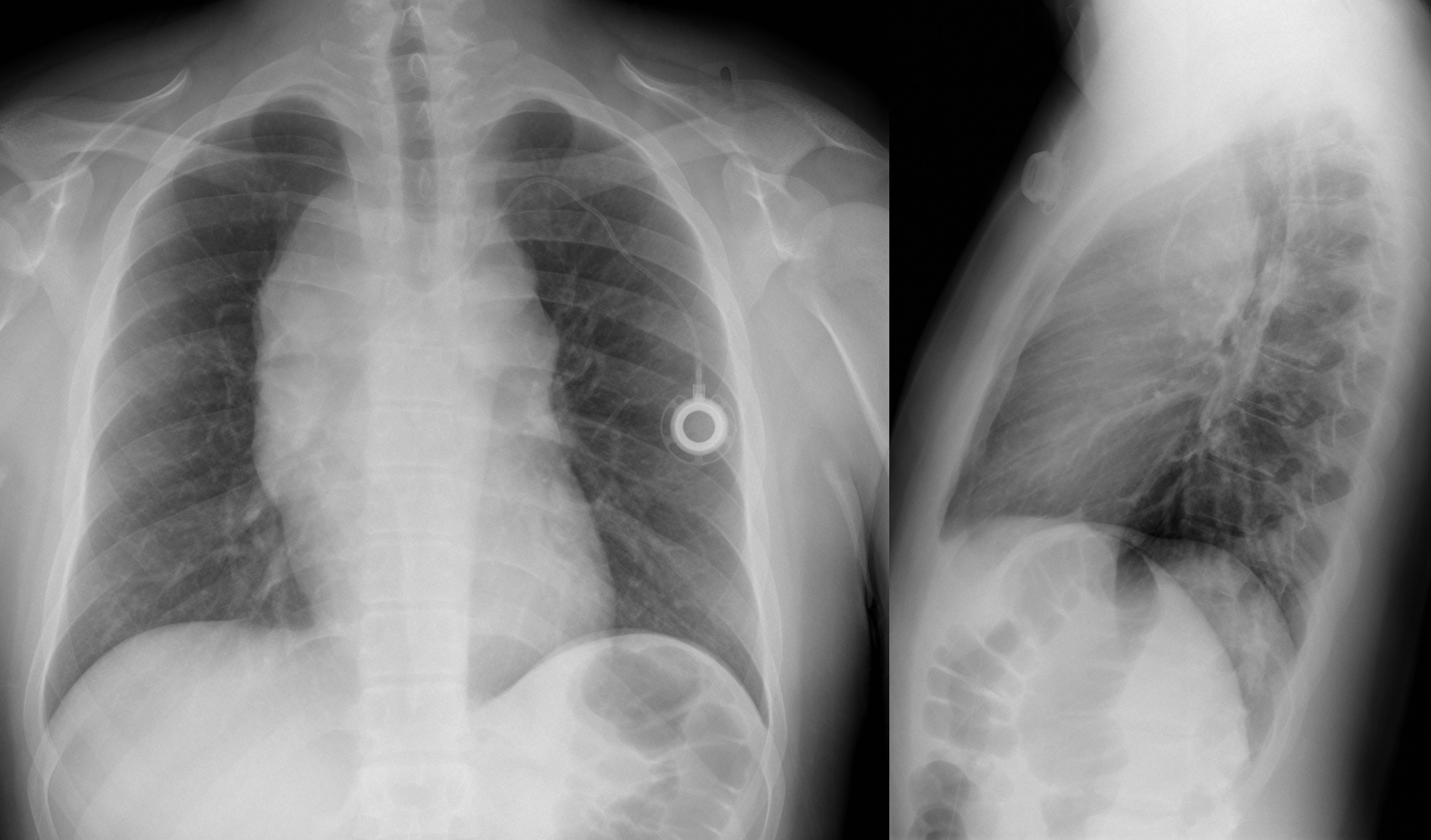
Patient presents with headache and papilledema. What's the diagnosis?
Hx: hyperextension injury (contact and non contact), varus directed blow to flexed knee, direct blow to anteriomedial knee. Report instability symptoms when knee is in full extension.
PE: Varus stress testing
Varus laxity at 0 indicate LCL and cruciate ligament (ACL/PCL) injury
Varus laxity at 30 indicates LCL injury
Dial test - inspects the external rotation at the knee joint/performed in both 30 and 90 knee flexion. The dial test inspects the external rotation at the knee joint
https://www.youtube.com/watch?v=pW4yv0zg4RY
Positive at 30 = > 10 external rotation asymmetry = isolated PCL injury
Positive at 30 & 90 = Posterior lateral corner injury and PCL injury
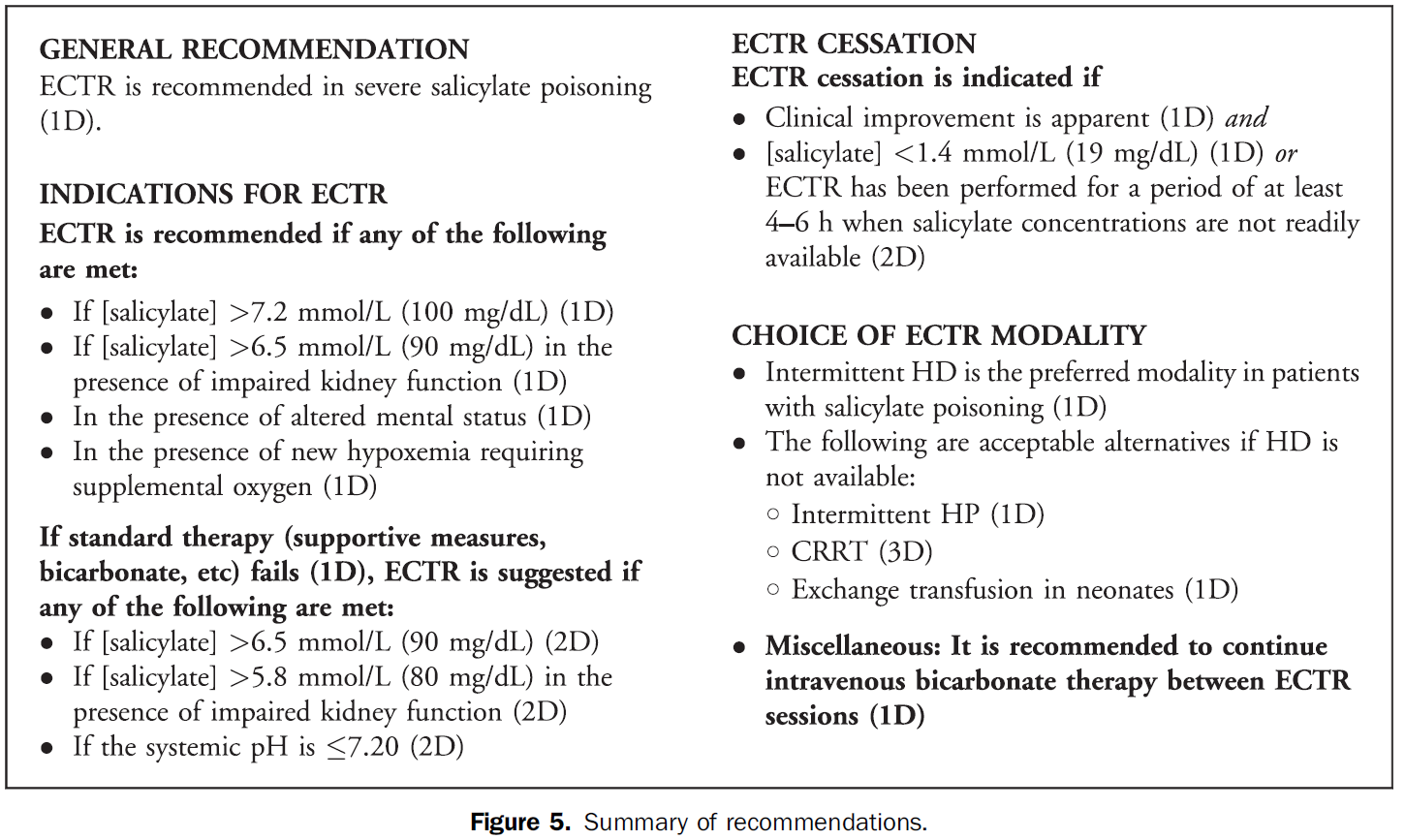
The Extracorporeal Treatments in Poisoning (EXTRIP) Workgroup has published their latest review, this time on extracorporeal treatment for salicylate poisoning. Here are their recommendations on when to dialyze: