Injuries are a leading cause of morbidity and mortality globally
Injuries are the leading cause of preventable death in travelers
Bottom Line: Stay safe while travelling. The same safety habits used in the US, such as wearing your seatbelt or not drinking and driving, are important patterns while traveling.
Your ESLD patient is hypotensive with a tense abdomen, and he needs a paracentesis!
--ALWAYS use ultrasound to localize a fluid pocket [Fig 1]! Take the time to use color Doppler to look for underlying abdominal wall varices [Fig 2]. Cirrhotic patients frequently have abnormal abdominal wall vasculature [1-2].
--Hemorrhage from paracentesis is exceedingly rare, and reversal of mild coagulopathy probably isn't that important [3-4].
--In hypotensive patients, consider placement of a small pigtail catheter for slow, continuous drainage (e.g. 8.3F pericardiocentesis catheter) instead of large-volume paracentesis. Non-tunneled catheter infection risk goes up after 72h [5].
--Albumin replacement improves mortality and incidence of renal failure in patients with SBP or other infection [6-7].
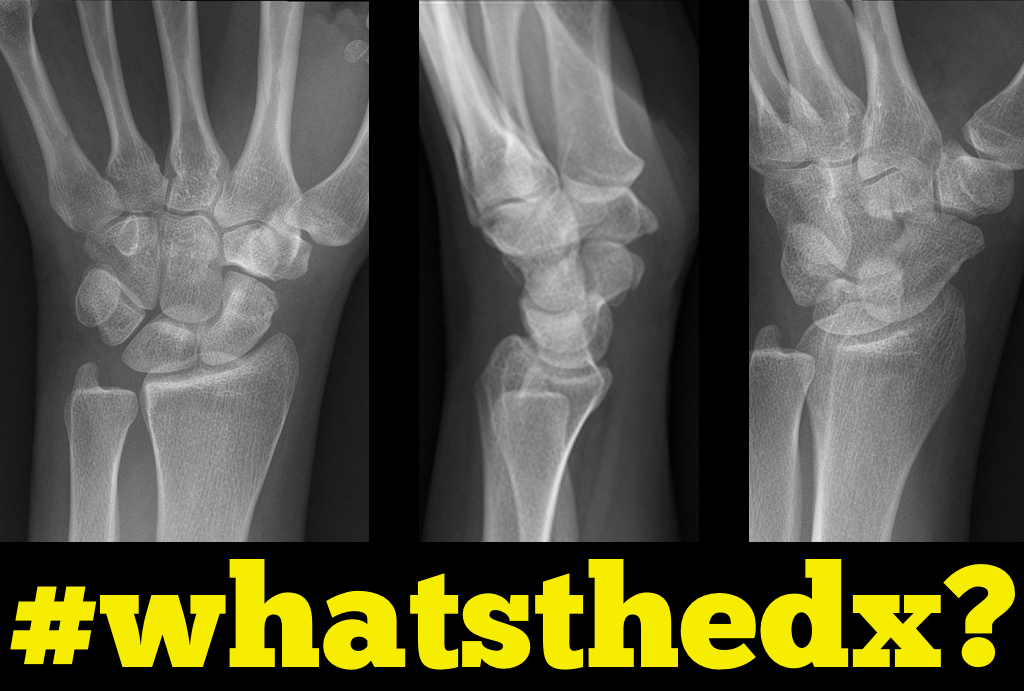
Person presents following a fall on an outstretched hand and there is snuffbox tenderness. What's the diagnosis?

Policeman's Heel:
When patient's present complaining of heel pain we often think immediately of plantar fascititis,and heel spurs. If they jumped and landed on the heel with are concerned for calcaneal fracture. However, a policeman's heel can occur from repetitive bounding of the heel or from landing on it as in a fall or jump.
Policeman's heel has been descirbed as a plantar calcaneal bursitis, inflammation of the sack of fluid (bursa) under the heel bone, or a contusion of the heel bone due to flattening and displacement of the heel fat pad, which leaves a thinner protective layer allowing the bone to get bruised.
Regardless of cause this responds well to NSAIDs, limiting weight bearing, or taping the foot. If the repetitive activity is not reduced this can easily become a chronic cause of heel pain. A short video showing how to tape the foot can be found at https://youtu.be/nQtkwfJrhXo
Making the wee patient pee – a non invasive urinary collection technique in the newborn
Obtaining a urinary sample in a neonate can be challenging and time consuming. The most commonly used non-invasive technique is urine collection using a sterile bag. This technique is limited by patient discomfort and contamination of the urinary sample. Catheterisation and needle aspiration are other options, but are more invasive.
A prospective feasibility and safety study enrolled 90 admitted infants aged under 30 days who needed a urine sample into the study [1]. They performed the following stimulation technique.
1. Feed the baby through breast-feeding or an appropriate amount of formula for their age and weight.
2. Wait twenty-five minutes. After twenty-five minutes clean the infant’s genitals thoroughly with warm water and soap. Dry with sterile gauze.
3. Have an assistant hold a sterile urine container near the infant
4. Hold the baby under their armpits with their legs dangling (if short handed, parents can do this)
5. Gently tap the suprapubic area at a frequency of 100 taps or blows per minute for 30 seconds
6. Massage the lumbar paravertebral zone lightly for 30 seconds
7. Repeat both techniques until micturition starts. Collect midstream urine in the sterile container
In the study, success was defined as obtaining a midstream urinary sample within 5 minutes after initiation of the stimulation procedure. There was a 86% success rate (n=69/80). Mean time to sample collection was 57 seconds. There were no complications, but controlled crying occurred in 100% of infants. The study was limited by the lack of a control group. Previous studies have described longer collection times with traditional non invasive techniques, up to over an hour [2].
Conclusion
Consider the above mentioned stimulation technique to obtain a urinary sample in the neonate.
Status migrainosus is a migraine that lasts more than 72 hours, and can be rather challenging to control. A few tips to tackle this are:
1. Adequately hydrate all patients (IV fluids are usually required, especially with severe nausea/vomiting)
2. Establish realistic expectations for the patient. A patient with chronic daily headaches will not be pain-free in the ED.
3. Use IV nonopioid medications for pain control
1st Line:
- Dopamine Antagonists: in increasing efficacy
- Metoclopramide
- Phenothiazines: prochlorperazine, promethazine and chlorpromazine
- Butyrophenones: droperidol and haloperidol
- NSAIDs: such as Ketorolac IV or IM
2nd Line:
- Corticosteroids: Do not treat the migraine in the ED, but prevent headache recurrence within 72 hours.
- Magnesium Sulfate: Has shown mixed efficacy. More likely to have a sustained benefit in patient with serum magnesium level of 1.3mg/dL or less.
- Valrpoic Acid: Be careful of combining it with Topiramate.
- Vasoconstrictors: Triptans, ergotamine, dihydroergotamine. Effective, but use is limited by contraindications.
- Opioids: Last resort
The RV is a low-pressure chamber that doesn’t tolerate acute increases in pulmonary pressures (e.g., ARDS, pulmonary embolism, etc.); acute increases can lead to RV dysfunction / failure
Managing RV dysfunction requires a three-pronged approach:
You find this interesting view while scanning a patient. Which view is this and why should you care about it?
Sodium Supplementation and Exercise-Associated Hyponatremia (EAH) during Prolonged Exercise (ultramarathon running)
Weight loss of around 4% body weight (relative to pre race weight) can be anticipated to maintain euhydration in such a prolonged event
Those who become symptomatic with EAH have either gained weight or lost less that 3-4% body weight
Overhydration rather than inadequate supplemental sodium intake is a greater contributor to the development of EAH
There is a suggested link between EAH and rhabdomyolysis. The mechanism remains unknown and it is unclear which condition may augment the other. Further research is needed.
Take home: Avoid overhydration during prolonged exercise to prevent EAH.
The answer may be no, as long as you have a serum HCO3. In this retrospective study, linear regression was used to to assess serum HCO3 as a predictor of venous pH. Logistic regression was also used to evaluate serum HCO3 as a predictor of DKA. Using a HCO3 cutoff of <18 mmol/L had a sensitivity of 91.8% and specificity of 91.7% for detecting a pH <7.3. A HCO3 < 8 had a sensitivity of 95.2 % and specificity of 96.7 % for detecting a pH <7.1.
Introduction: As discussed in previous Pearls, Middle East respiratory syndrome coronavirus (MERS-CoV) is a recently emerged respiratory viral infection that is caused by a single stranded, positive-sense RNA novel coronavirus.
Updates:
As of August 12th, 2015, WHO has received reports of:
The current reported case fatality rate is approximately 36%
Recent outbreaks have included
Bottom Line:
MERS-CoV is significantly contagious respiratory virus with high lethality. It is spread primarily as an airborne virus, though the CDC currently recommends both standard contact and airborne precautions. There is currently no vaccine and only supportive treatment is advised.
Don’t be a vector or have your emergency department be a nidus of infection! Take appropriate precautions, including:
People who hide illicit drugs can be classified in to three different types.
1. Body stuffers – people who ingest drugs that are poorly wrapped to “eliminate” evidence from police – e.g. street dealers.
2. Body packers – people who ingest large amounts of “well” packed drug packets to transport drugs (usually internationally) – aka “mule.”
3. Body pushers – people hiding drugs in rectum or vagina.
Body stuffers are more frequently encountered in local ED compared to body packers. Stuffers can become symptomatic as the ingested drugs (cocaine, heroin, amphetamines) are often poorly wrapped (e.g. in plastic bag/wrap, cellophane paper, aluminium oil, etc.).
Recent retrospective article looked at the utility of 6-hour observation period in the ED as a management strategy for body stuffers. (n=126)
Characteristics
1. Ingested drugs (self-reported): heroin (48%), cocaine (46%), other drugs [cannabis, MDMA, diazepam, methamphetamine] (16%), unknown (8%)
2. Time of ingestion to ED presentation
Clinical findings
76% of the patients experience clinical signs of toxidrome at time of presentation.
Most common findings:
Patients who ingested heroin were more symptomatic vs. cocaine (87% vs. 70%)
Patients were discharged:
Conclusion
Pressure Regulated Volume Control (PRVC)
Here are some basic pearls about PRVC Ventilation
Benefits: minimum PIP, guaranteed tidal volume, patient can trigger more breaths, improved oxygenation, breath by breath changes
55 year-old male presents with chest pain. Echo is shown below (parasternal long-axis on the left and aortic root / ascending aorta on the right), what's the diagnosis?
Flumazenil is generally avoided in most adult patients with suspected benzodiazepine overdose due to resedation, seizures/withdrawal, inconsistent reversal of respiratory depression, and the potential for proconvulsant coingestants.
Three relatively recent poison center studies have attempted to demonstrate the safety of flumazenil in this setting. [1-3] In the first study there were 904 adult patients with 13 reported seizures and 1 death. [1] A second study specific to pediatric patients reported 83 patients with no seizures and no deaths. [2] A third study found 80 patients with 1 seizure and 0 deaths. [3]
On the surface, it may appear that flumazenil is safe to give. But, retrospective poison center studies from voluntary reporting cannot be used to prove a drug's safety. The true denominator is unknown. In the pediatric study, we wouldn't expect children to experience withdrawal since they aren't on chronic benzodiazepine therapy. [2] So, it's no surprise there weren't any seizures or deaths.
A recent systematic review and meta-analysis of randomized trials summed it up perfectly: "Flumazenil should not be used routinely, and the harms and benefits should be considered carefully in every patient." [4] Cases in which to consider flumazenil are pediatric patients and reversal of procedural sedation if needed.
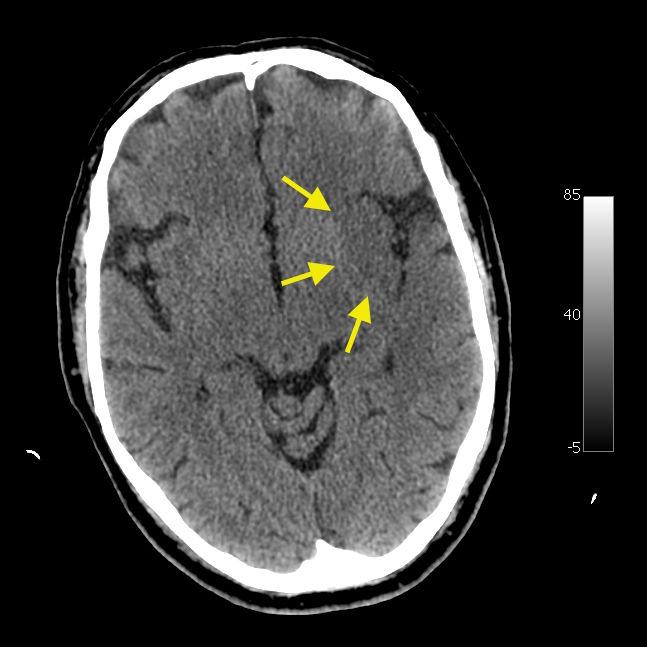
Neuroimaging Tip - Loss of the Insular Ribbon Sign
Is It Really ARDS?
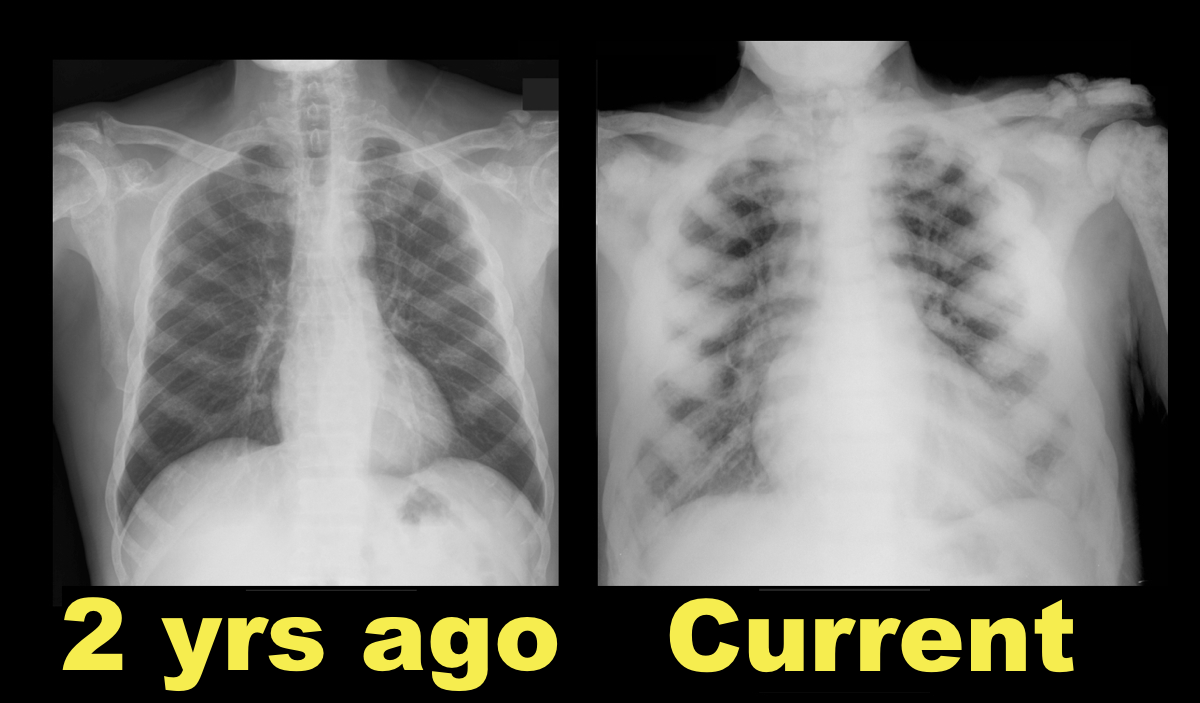
64 year-old male with no past medical history presents complaining of chronic weight-loss and diffuse chest pain; CXR is shown. What's the diagnosis and what other disease(s) may present similarly?

Handcuff Neuropathy
Compression of the superficial radial nerve against the radius.
Tends to occur with prisoners (too tight cuffs or person struggling)
Usually purely sensory lesion
Nerve regeneration can take 8 weeks (about an inch a month)
Document sensory exam to sharps or 2 point sensation.
DDx: De Quervain's, Carpal tunnel, Gamekeeper's thumb,
No need to splint
A recent meta-analysis published in Pediatrics reviews the diagnostic accuracy of lung ultrasound for pneumonia. According to the commentary, pneumonia is the leading cause of illness and death in children worldwide; it accounts for 18% of the total number of deaths in children <5 years, more than TB, AIDS, and malaria combined.
They performed a systematic search on several major databases using a combination of controlled keywords for age <18 years, pneumonia, and ultrasound. Of the initially 1475 identified studies, 8 were ultimately chosen for further evaluation.
Characterizing the meta-analysis:
- Three were conducted in the ED, 2 on the wards, 1 in the PICU and 2 in the NICU.
- Of the 765 children encompassed, the mean age was 5 years and they were 52% boys.
- Five of the 8 studies noted using highly skilled sonographers.
- The studies originated from Italy (5), US (1), China (1) and Egypt (1).
- All studies used CXR +/- clinical criteria as the diagnostic standard; LUS assessment was blinded to associated CXR results in 7 of 8 studies.
Results:
- LUS in the diagnosis of pediatric pneumonia had an overall pooled sensitivity of 96% (95% confidence interval [CI]: 94-97%) and specificity of 93% (95% CI: 90-96%).
- Positive and negative likelihood ratios were 15.3 (95% CI: 6.6-35.3) and 0.06 (95% CI: .03-0.11), respectively. For reference, remember that an LR >1 indicates an increased probability that the target disorder is present and >10 is a large or often conclusive increase in the likelihood of disease. Likewise, an LR <1 indicates a decreased probability that the target disorder is present and <0.1 is large or often conclusive decrease in the likelihood of disease.
- The area under the receiver operating characteristic (ROC) curve was 0.98. The ROC curve represents a measure of the accuracy of a test, >0.9 is considered to be excellent.
- In order to determine whether there are genuine differences underlying the results of the studies (heterogeneity) the I-squared statistic was implemented, with values consistent >0.45, demonstrating significant heterogeneity.
Bottom line: LUS appears to be an accurate test for the diagnosis of pneumonia in children. The limitation of this meta-analysis is mainly in the small number of studies and the significant heterogeneity between them, likely due at least in part to the fact that they used CXR +/- clinical data as the diagnostic standard. Nevertheless, the results provide evidence for the use of LUS as a cost-effective tool that potentially eliminates ionizing-radiation from the work-up of pediatric pneumonia and has application potential in resource-limited settings.