Extracorporeal Membrane Oxygenation
Got some interesting info today on the costs of some commonly used antihypertensive medications. Keep in mind that in patients with severe hypertension, your options of IV drips are limited.
Here is some info from our hospital:
Fenoldopam - $113.28
Nicardipine - $94.67
Esmolol - $82.15
Nitroprusside - $20.86
Labetalol - $14.40
Nitroglycerin - $2.90
Although Fenoldopam (Corlopam), which has been around for years, is more expensive than Nitroprusside, it is just as effective and without the side effects.
A new drug on the market that we don't have yet, Clevidipine, is just as effective as the big guns Nipride and Fenoldopam. Costs at this point are unknown.
More on antihypertensive medications next week....
It's no secret that the elderly are at high risk for adverse drug effects. The average elderly patient takes 5 prescribed medications plus two over-the-counter medications. As many as 5% of admissions in the elderly are attributable to adverse drug effects.
Anytime you prescribe a new medication to an elderly patient, ALWAYS check for the possibility of drug interactions.
Snuff Box Tenderness:
It has become the standard of care that individuals with snuff box tenderness, or pain with axial loading of the thumb, be placed in a thumb spica splint for 1-2 weeks until follow up x-rays can be done. This is done to rule out an occult scaphoid fracture. However, this practice can be hugely inconvenient to the patient and result in some atrophy of their forearm.
An alternative approach is to obtain a CT scan through the wrist to look specifically at the scaphoid bone. If the CT scan is negative you can send them home with some pain control, RICE (Rest, Ice, Compression, Elevation) treatment and let them use thier thumb. No splint is needed. If it is positive then you can splint them and have them follow up with orthopedics or hand surgery.
This is a semi-synthetic opiate with partial agonist activity at the mu receptor. For an example of what a partial agonist is - see attached illustration. It is used in opioid addiction but is not as regulated as methadone clinics. Take a small course and you are licensed to prescribed it. Primary caregivers are now able to administer buprenorphine to assist addicts though it is not recommended if the patient is requiring more than 40mg of methadone (rules out everyone in Baltimore).
The tablets (Suboxone) also contain naloxone to prevent intravenous injection which would induce withdrawal. Naloxone is not orally bioavailable and thus can be mixed into the pill.
Overdose is treated like any other opioid and naloxone should work.
Buprenorphine can illicit an opioid withdrawal response if the patient is currently on an opioid and then takes buprenorphine.
Suppose to be safer than methadone - no QT prolongation and less respiratory depression
Critically Ill Patients with H1N1
Management of Heparin-Induced Thrombocytopenia (HIT)
HIT occurs when antibodies form to a Heparin-Platelet Factor 4 (PF4) complex in patients who have been exposed to Heparin.
The main clinical manifestation is thrombosis (arterial/venous). Treatment is unique in that only certain medications can be used.
Medical Management options in HIT:
So, when a patient with a history of HIT shows up in the ED with a DVT/PE or other thrombotic problem, these are your mainstay drugs.
The recent Baltimore City Marathon served as a nice reminder in a few cases that long-distance running and other ultra-endurance events can produce elevations in troponin levels. To review the non-cardiac-disease causes of troponin elevations:
sepsis, PE, COPD, carbon monoxide, intracranial abnormalities (including SAH, stroke, IC hemorrhage, seizures), ESRD, rhabdomyolysis, eclampsia and preeclampsia, extreme endurance exercises, UGI bleeding, LVH, catecholamine toxicity
Reimburshment Pearls:
Often charts are down coded as it is not clear from the documentation that your medical decision making was complex.
For instance, if your final diagnosis is GERD, and you do not document that you were also concerned about angina or a pneumothorax your level 5 chart could be coded as a level 3, since the final diganosis does not seem that complex. In order to prevent this document:
I realize that when you are busy this might be the last thing on your mind, but the difference between a level III chart and a level V chart is about $100, and the only additional work is the 3 minutes it would take to document what you did for the patient.
More to come...
While it is often ok to defer removal of pesky nasal foreign bodies until ENT follow up, if the foreign body may be a button battery, emergent identification and removal is indicated.
Damage can occur in 3 hours, and by 24 hours, near complete necrosis of turbinates and ala has been described.
A 34 y/o m presents to the ED agitated and combative with the following vitals signs: T 104.6, P 136, BP 198/124. His urine toxicology screen is positive for amphetamines.
Damage Control Resuscitation
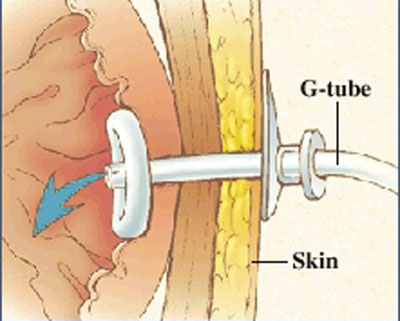
I am sure everybody has received a patient from a nursing home that had a malfunctioning PEG tube. Now if they would only crush the tablets before putting them down the tube, or better yet use liquid medications our life would be easier.
But what do you do if it is Friday and the GI lab is not open to Monday. The answer is that you can remove the PEG and replace it with another PEG tube or even a foley catheter will do for the weekend. The original PEG tube has a semi-rigid plastic ring (as shown in photo) and does not have a balloon that can be default. You can pull these out by placing counter traction on the abdominal wall and pulling with steady firm pressure. This may take a little more force than you are initially comfortable with.
Please see the attached photo of a PEG tube, and remember the other option is to admit these patients for IV fluids until the GI lab opens.
While breastfeeding is still the preferred source of infant nutrition by the AAP, a little-known fact is that breastfeeding may expose the nursing infant to environmental pollutants to which they might not normally be exposed. If you have a mother that appears ill due to exposure to any of these agents, don't forget to have the infant examined as well for signs of intoxication.
Severe mitral regurgitation (MR) after MI, accompanied by cardiogenic shock carries a poor prognosis.
Severe MR in many cases is due to infarction of the posterior papillary muscle, and in these cases the area of infarction tends to be less extensive than in those with MR due to severe left ventricular dysfunction.
Take Home Pearl:
The presence of pulmonary edema and/or cardiogenic shock in a patient with an inferior STEMI should prompt consideration for acute MR due to papilary muscle rupture. Get an echo as fast as you can to confirm or r/o the diagnosis. Treatment is afterload reduction, inotropic support, and urgent surgical repair.