Using a database of 300,000 patients and applying a predictive measure for mortality, these authors found that patients over 66 with a high likelihood of 6 month mortality at the time of presentation were more likely to be admitted to an ICU when they presented to an ED. The authors conclude there is much work to be done regarding discussion of goals of care based on this information.
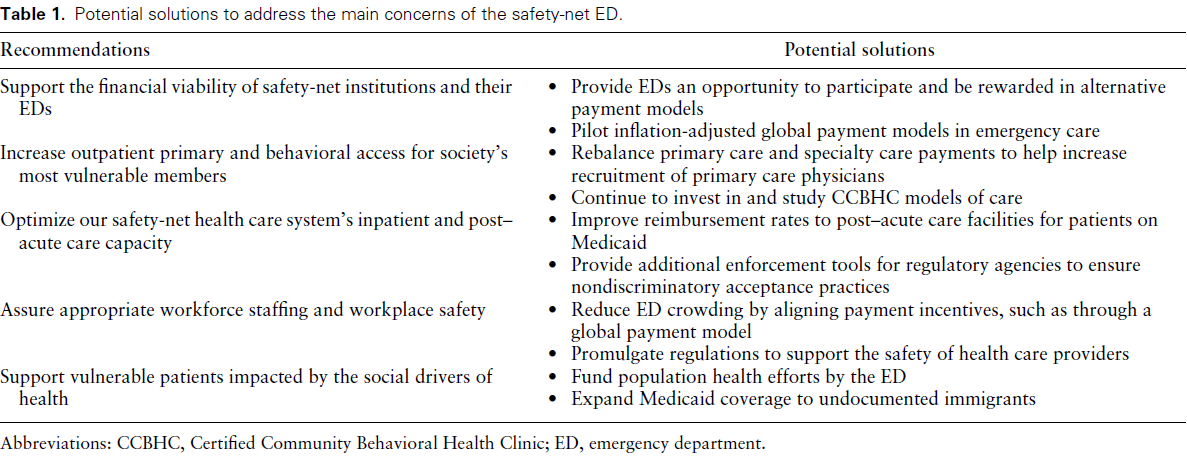
Bottom Line: Safety-net hospitals are those that see a substantial share of uninsured, Medicaid, or low-income Medicare patients. Their emergency departments (EDs) deliver disproportionally more undercompensated and uncompensated care, yet have similar operating costs as other EDs. Authors convened a group of 15 administrators of academic safety net EDs to identify and
develop a consensus understanding of barriers to delivering optimal care. See the link for details of their conclusions.
Click the link for below to read the bulleted, abridged version of the Executive Summary of the Updated SSC Guidelines for Adults with Sepsis and Septic Shock 2026…
Bottom Line: Among adult ED patients tested for gonorrhea and chlamydia, empiric treatment often does not align with confirmed infection. There are also notable sex disparities; in this study, females with confirmed infection were ~3.5 times more likely than males to not receive empiric treatment.
Looking at a national database, this study concluded the use of low titer O whole blood during trauma resuscitations was increasing at level one centers but not at level 2 and 3 centers. Is this a representation of the national blood supply as whole blood is harder to stock? We need to understand this trend to assure equal and appropriate care to trauma patients across the country.
Educational Pearls for the ED:
Many Muslim patients with diabetes will fast despite medical advice. Studies show a significant number continue fasting even when they are considered high risk.
Key medical risks during Ramadan fasting include:
- Hypoglycemia
- Hyperglycemia and diabetic ketoacidosis
- Dehydration
- Medication nonadherence or altered dosing schedules
This was review of 24 studies across 21 years that aimed to look at the complications associated with pediatric intubation in the hospital. The article also includes a list of all the articles with brief conclusions from each study for those interested.
Among a combined 7135 patients, there was an 84.7% overall success rate with a 30.1% rate of complication. There was a 69.8% first pass success rate. Desaturations < 90% was the most common complication followed by mainstem intubation. Studies also noted cardiac arrhythmia (55/3858 patients), hypotension (121/4536 patients) and cardiac arrest in 105/4836 patients). Other adverse events included esophageal intubation, surgical airway management and airway trauma.
Indications for intubation from most to least common are: neurologic, respiratory, trauma, cardiac arrest, sepsis, shock, cardiac failure and intoxication.
The debate of the best way to administer epinephrine in cardiac arrest continues. Pediatric arrests are different from adults in many ways, but some differences in arrest include 1) data supporting improved survival with early epinephrine administration and 2) less IVs are placed in children overall compared to adults making IO placement possibly quicker.
In this study, 739 patients were included with a median age of 1 year. The IO was used in 72% of patients and an IV was used in 27.6% of patients. There was no difference between survival to hospital discharge or prehospital ROSC between the two groups.
Beta-blocker is used for tachycardia among patients with sepsis. Landiolol, a new beta-blocker with highly selective B1-agonist (ratio of B1:B2 250:1) has recently been approved for use. In a network meta-analysis comparing landiolol with esmolol (B1:B2 ratio 30:1), landiolol was associated with increased 28-day mortality (relative risk [RR], 1.57; 95% CI, 1.08–2.30). This result carried low certainty as there were not as many studies using landiolol and there was no direct comparison between landiolol versus esmolol.
Similarly, landiolol was associated with higher norepinephrine requirements (mean difference [MD], 0.17 ?g/kg/min; 95% CI, 0.02–0.32). Again, there was no direct head-to-head comparison between landiolol versus esmolol.
Another study, this one from New Zealand, showing older trauma patients with similar injury severity score had less trauma team activations and higher mortality.
BOTTOM LINE: You are probably doing fine in your ED already, just delay cord clamping 60 seconds when possible.
The latest guidelines for neonatal resuscitation recommend a 60 second delay minimum in clamping the cord for neonates of all gestational ages who are stable.
In those OVER 28 weeks for whom clamping cannot be delayed (due to maternal or neonatal factors), cord milking can be performed.
DO NOT milk the cord in neonates under 28 weeks as this can increase the risk of intraventricular hemorrhage.
Cord milking is performed by gently massaging the cord blood starting about 20cm away from the infant and moving toward the infant's body 3-4 times before clamping. This essentially allows for a transfusion before clamping occurs, increasing LV preload and allowing for improved oxygenation.
Fortunately, in most EDs, the time to obtain the equipment for cord clamping likely takes more than 1 minute, so chances are in your practice you don't have to worry too much about this. But if you happen to have everything prepared, wait 60 seconds before clamping.
The 2026 Acute Pulmonary Embolism Guidelines were recently released. They recommend low-molecular-weight heparin (LMWH) over heparin for hospitalized patients with acute PE who require initial parenteral therapy unless they are in Category E2 Acute PE Cardiopulmonary Failure (level 1B-R).
Top benefits include:
JAMA Internal Medicine recently published a systematic review and Bayesian meta-analysis looking at the utility of prophylactic antibiotics in cirrhotics with acute upper GI bleeding
TLDR: shorter durations of antibiotics (including no antibiotics!) had a 97.3% probability of noninferiority for all-cause mortality
Bottom Line: We are terrible at estimating how much blood people are losing just by looking at it. Use calibrated drapes (drapes with markings that tell you how much blood is being lost), or just a large bag and then weigh it afterwards (1g ~ 1ml of blood loss).
This case report reminds us that vasculitis is an inflammatory process that attacks blood vessels leading to organ dysfunction. The etiology can be a hypersensitivity reaction (think drugs) or an IgA mediated process secondary to infection (Strep or Mycoplasma). In this case, concomitate use of NSAIDS (very common etiology of hypersensitivity) and Mycoplasma lead to vasculitis. Treatment ranges from supportive care, to steroids to immunosuppressive agents such as azathioprine.
Of 925 ED headache patients in this meta analysis comparing extrapyramidal side effects of bolus vs. continuous infusion of metoclopremide the majority of the reactions occurred in the bolus group.
Bottom Line:
Kratom is an herbal extract used as an alternative medicine and recreational substance with marked increase in use over recent years. Kratom contains a complex mixture of psychoactive ingredients with effects at multiple receptors (mu, serotonin, dopamine, and alpha-adrenergic receptors) and causes stimulant effects at lower doses and opioid effects at higher doses. Depending on the predominant clinical effects, treatment with naloxone, benzodiazepine, and labetalol have been reported.
When compared to saline(!) trauma patients with a high injury severity score who received ketamine via pca for pain control had better quality of life indicators at 1,3, and 6 months post injury.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}