Emergency contraception comes in multiple forms, all of which have their own side effects and best case use scenarios that emergency medicine providers should be aware of to offer the best counseling.
Consider your patient before advising - if their BMI is > 25, consider ulipristal. If they want the most effective method, that'll be a copper IUD - but make sure they can get an appointment within 5 days of the unprotected intercourse! If they cannot afford ulipristal or levonorgestrel (which can both be $50 without insurance), but they already have OCPs, combining OCPs to the total noted above can be a method of emergency contraception that is still very effective.
Background:
Acetaminophen can reduce hemoprotein induced oxidative damage. There has been growing discussion about its benefits in critically ill patients with sepsis. Multiple observational studies have found conflicting results on mortality in critically ill patients with sepsis. The ASTER trial found no difference in number of days alive and free of organ support. Interestingly their secondary outcomes found significantly less development of ARDS in the acetaminophen group 2.2% vs 8.5%, p = .01. There was also a non-statistically significant difference in mortality between the groups in favor of the acetaminophen group, 17% vs 22% p = 0.19. This study looked to further evaluate if acetaminophen used in critically ill patients with sepsis would have a decrease in mortality and increase in ventilator free days.
Study:
- Retrospective analysis of the Ibuprofen in Sepsis Study (ISS)
- The ISS was a randomized clinical trial comparing ibuprofen with placebo in critically ill patients with sepsis. Careful documentation of Acetaminophen use was recorded for the trial
- Critically-ill adults across 7 ICU’s in the US and Canada with known or suspected infection and severe organ dysfunction
- Acetaminophen use within 48 hours of enrollment = Acetaminophen exposed
- Primary outcome: 30-day mortality
- Secondary outcome: Renal failure and ventilator free days up to day 28
- 455 patients. 172 Acetaminophen unexposed, 235 Acetaminophen exposed.
Results:
- Propensity-matched analysis showed a lower mortality risk at 30 days in patients exposed to acetaminophen compared to unexposed, 32% vs 49% (HR 0.58, p .004)
- Secondary outcomes found acetaminophen exposed group had more ventilator free days (p .02) but there was no difference in renal failure among the groups.
Limitations:
- Major risk for confounding variables
- Retrospective and the data used was from decades ago (1989 -1995). Sepsis care has evolved and improved since this time
- Dose and frequency of acetaminophen administration was not standardized
Take Home Points:
- Interesting research that provides further support on the possible benefit to using acetaminophen in the management of critically ill patients with sepsis.
- With the ASTER trial showing a signal for the decrease in development of ARDS and this study showing improvement in mortality one could make a case for starting acetaminophen early in the course for these patients. However, the data is conflicting and more prospective, RCT’s are needed to confirm these findings before making this a staple for sepsis care in critically ill patients.
This study looked at pre-trauma mental health diagnosis (from medical records) and post-trauma mental health symptoms as assessed by survey. The majority of patients suffered blunt trauma and mean age was 67. Having pre/traumatic mental health diagnosis and particularly post-traumatic symptoms lead to worse health outcomes and financial conditions. Further work needs to be done to assess how to improve mental health symptoms post-traumatic injury.
Non benzodiazepine muscle relaxants
Muscle relaxants were the most commonly (32%) prescribed medication upon discharge from the ED for lower back pain.
Muscle relaxants, such as cyclobenzaprine, provide short term pain-relief for patients with acute low back pain compared to placebo.
There is little difference in efficacy among the various muscle relaxants.
Evidence for muscle relaxants for back pain is weak compared to NSAIDs, so limit use to patients who have contraindications to NSAIDS.
There is no strong evidence that combination therapy with NSAIDs is more effective than NSAIDs alone.
If using during the day, consider using a lower dose (cyclobenzaprine 5mg) and a higher dose at night (10mg).
If treating with NSAIDs, consider using only at night to promote sleep.
Also, limit use to those patients who can tolerate the side effect profile of muscle relaxants, which include anticholinergic effects, dizziness, and sedation.
Risks of these agents increase with age, so should be used with caution in older adults.
Often given to this population due to fears of NSAID side effects.
Presentation:
JME is a common cause of juvenile/adolescent seizures.
Patients typically present between 12-18 years of age with a combination of myoclonic movements, absence seizures and generalized tonic-clonic seizures.
This diagnosis is often mistaken for morning clumsiness due to the myoclonic movements and asking about myoclonic movements can help make the diagnosis.
Diagnosis:
Diagnosis is primarily based on history. Myoclonic seizures are required to make the diagnosis. Patients with consistent history can receive outpatient EEG to confirm the diagnosis.
No ED images or tests needed with the correct clinical history and return to baseline. (even outpatient with appropriate history imaging is not needed as it is usually normal)
Treatment:
Valproic acid is typically the treatment of choice for patients though must be used with caution in women of childbearing age. Other common treatment options include levetiracetam and lamotrigine. With the correct clinical history, these can be started in the ED.
Be sure to discuss good sleep hygiene and avoidance of alcohol with patients as these can be triggers.
Albuterol, a common bronchodilator used in the treatment of asthma and chronic obstructive pulmonary disease (COPD), can cause a surprising increase of lactate levels. The increase in lactate is usually mild to moderate (typically < 4 mmol/L) and transient. It does not necessarily indicate underlying sepsis, tissue hypoxia, or severe metabolic acidosis.
Mechanism:
Albuterol can cause a transient increase in lactate levels due to its beta-2 agonist effects, which promote glycogenolysis and increase anaerobic metabolism. This can result in elevated lactic acid production, even in the absence of tissue hypoxia or shock.
Timing:
This effect is typically seen within 30 minutes of albuterol administration and can persist for 1-2 hours after discontinuing treatment.
Monitoring:
If lactate levels are elevated in a patient receiving albuterol, consider the possibility of a pharmacologic cause rather than immediately assuming a more serious etiology like shock or severe metabolic disturbance.
Differentiating Causes of Elevated Lactate:
In a critically ill patient, elevated lactate can indicate hypoperfusion (e.g., septic shock, cardiogenic shock, or hypovolemic shock). However, when elevated lactate is associated with albuterol administration, the rise in lactate is often lower and resolves without intervention.
Management:
If albuterol-induced lactate elevation is suspected, continue with supportive care and monitor lactate trends. No specific treatment is necessary for the elevated lactate unless there are other concerning clinical findings that suggest a different underlying cause.
Conclusion:
In emergency settings, it's important to recognize that albuterol can cause a transient increase in lactate levels. Understanding this phenomenon can help avoid misdiagnosis and prevent unnecessary interventions in patients receiving albuterol therapy. Always correlate lactate levels with the broader clinical picture to guide management decisions.
Flow rates are, in theory, determined by Poiseuille’s Law, which states that the flow rate depends on fluid viscosity, pipe length, and the pressure difference between the ends of the pipe .
Of course we won’t be calculating this during a resuscitation! Nor would it be useful if we did: the equation assumes laminar flow, whereas turbulent flow is more likely. Nor is it practical to look up the viscosity of crystalloid/blood/plasma, which also dramatically impacts flow rates.
Instead, remember this equation: Larger + shorter = faster
And keep in mind the following:
In practice, our friends in Australia actually put common catheters to the test, and provided these helpful results:
Or, as a picture:
Note, these flow rates were achieved using crystalloid. Blood will be slower due to higher viscosity.
Do you ever tell your patients to “follow up with your primary care physician in 3-5 days”? How many of them actually do it? And does it make a difference?
Study Overview:
This study is a retrospective analysis of 28,085 adults (?20 years) presenting with acute abdominal pain (AAP) at 15 German emergency departments (EDs) in 2016.
Key Findings:
Hospitalization rate:
39.8% were admitted to the hospital from the ED.
Outpatient Care (OC) Before ED Visit:
33.9% had an OC visit within 3 days before their ED visit.
Of these, 48.6% were hospitalized.
Outpatient Care After ED Visit:
62.7% had OC follow-up within 30 days.
Factors Increasing Hospitalization Odds:
Age ?65 years: aOR 3.05
Prior OC: aOR 1.71
Male sex: aOR 1.44
In-Hospital Mortality:
3.1%
ED Re-visits Within 30 Days:
More likely in age ?65: aOR 1.32
Less likely with prior OC: aOR 0.37
Conclusion:
Acute abdominal pain in the ED is associated with high hospitalization and mortality rates, especially in older adults and those with prior outpatient visits. Prior outpatient contact is linked with both increased admission likelihood and reduced risk of ED re-visits, highlighting its complex role in care continuity. Improving outpatient care access and coordination may reduce ED burden and enhance outcomes for AAP patients.
While there are other factors to consider ie the health care system and its infrastructure, this does provide some interesting food for thought about what happens when we discharge patients.
A recent systematic review and meta-analysis evaluated the diagnostic accuracy of ultrasound in detecting acute diverticulitis. The analysis included 12 studies with a total of 2,056 patients. Ultrasound demonstrated a sensitivity of 92.5% (95% CI: 86.9%–95.8%) and a specificity of 87.7% (95% CI: 75.7%–94.2%).
The most commonly used diagnostic criteria across the studies included:
Similar to prior research on POCUS for nephrolithiasis, these findings support a POCUS-first approach for patients at low risk for serious alternative diagnoses. Ultrasound is a great alternative for patients with contraindications to contrast-enhanced CT, such as those with contrast allergies.
As the authors state, while ultrasound may be effective in identifying acute diverticulitis and its complications, such as abscess, additional imaging with CT may still be required to assess the severity of complications.
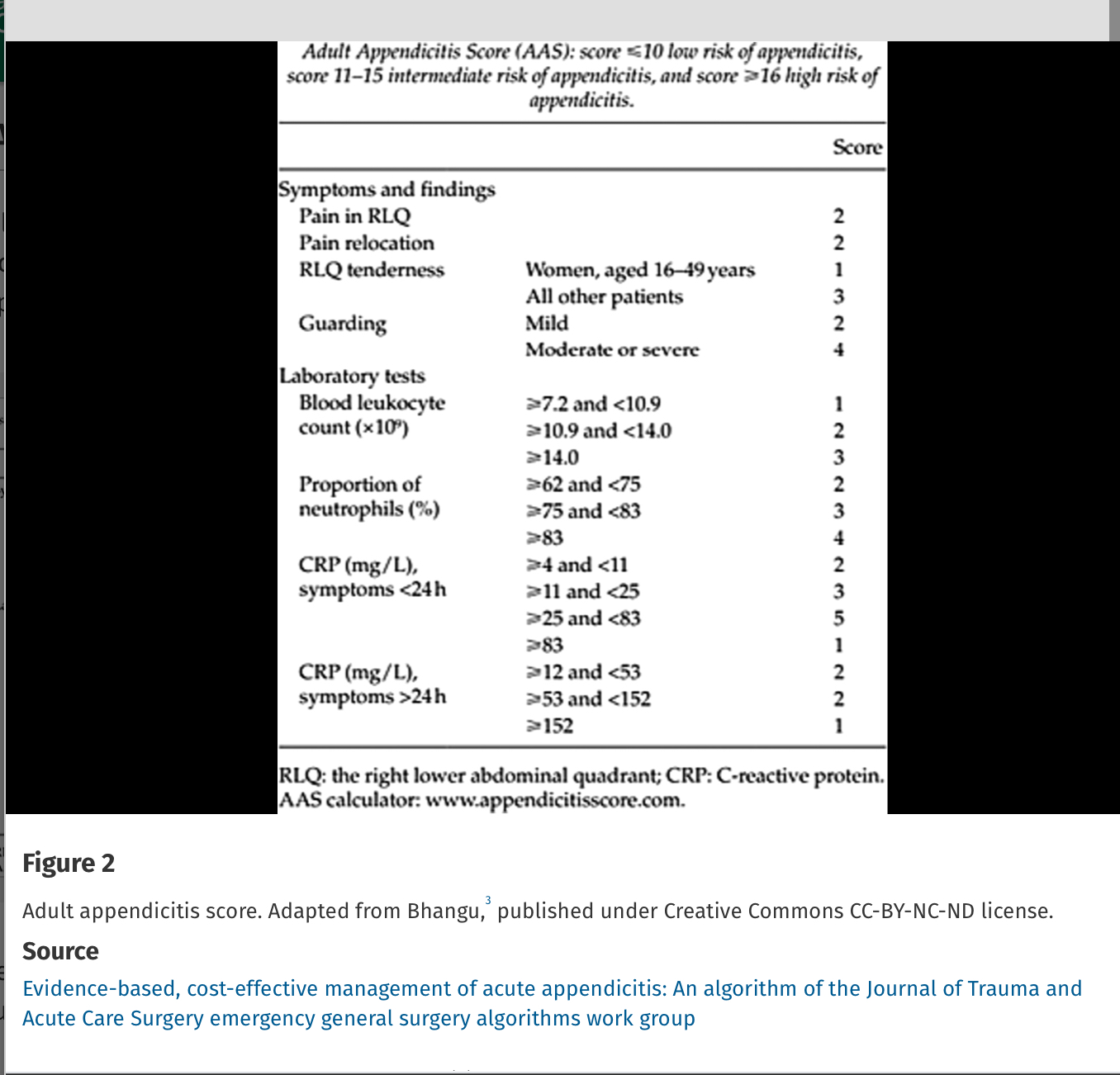
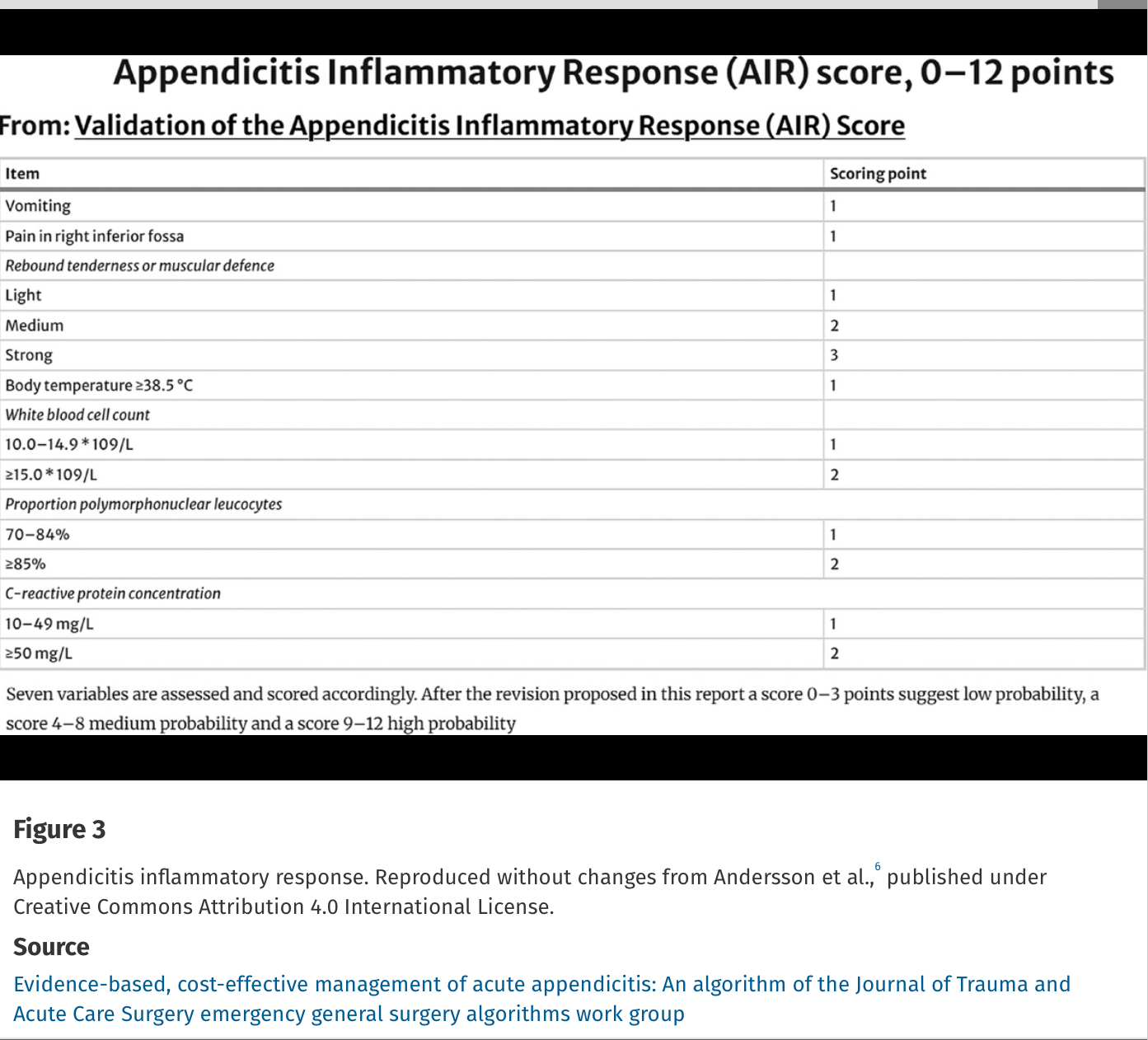
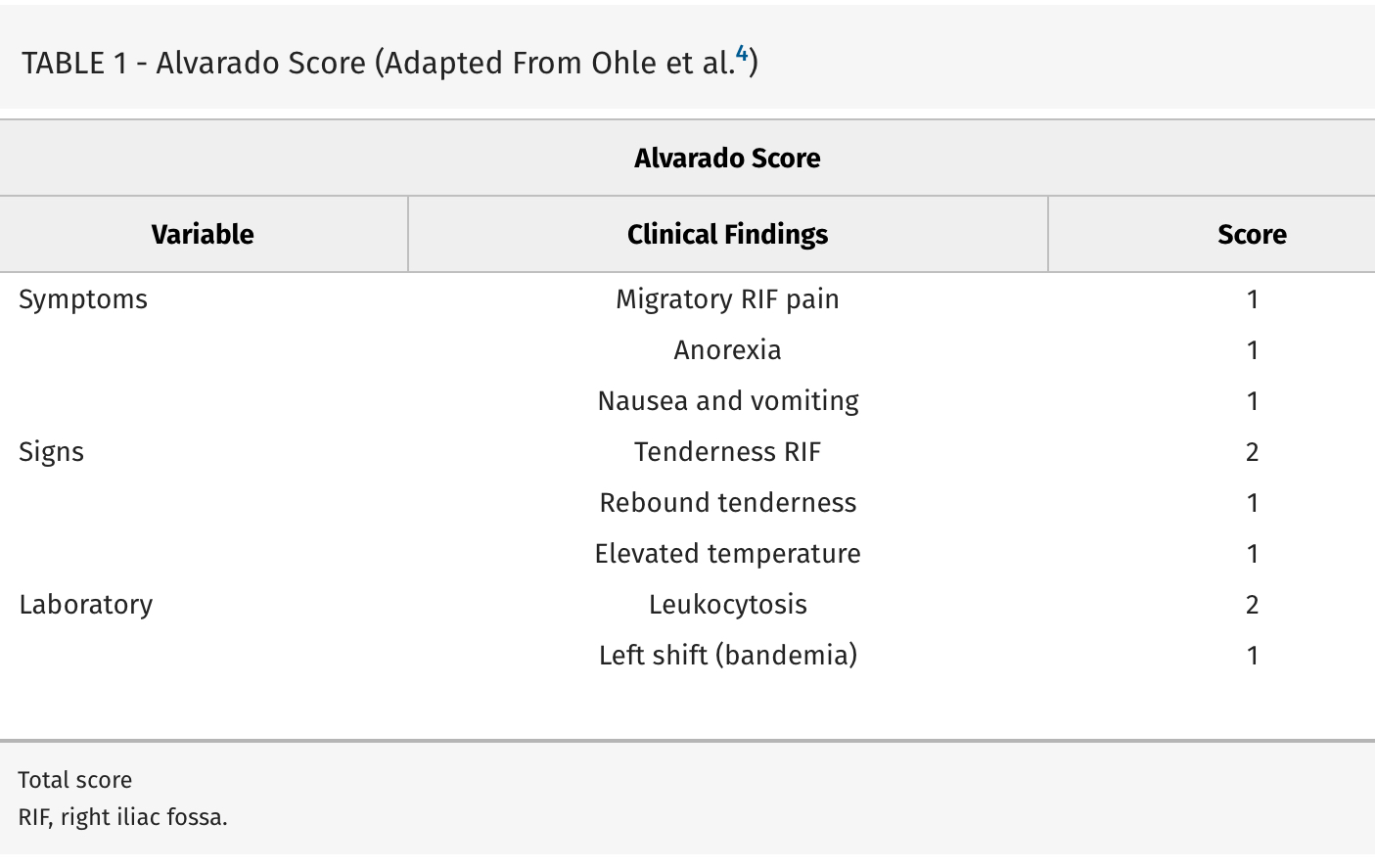
Missed appendicitis leading to rupture and peritonitis leads to morbidity, mortality, and malpractice claims. Part of a longer article looking at evaluation and management of appendicitis, these authors provide three scoring systems that can be used to identify appendicitis. Use of these scores can guide imaging and surgical consultation.
Alvarado Score: If a patient scores 1 to 4, the risk of appendicitis drops to 33%. If a patient scores >5, the risk of acute appendicitis is 66% or greater.
This study from Australia reminds us that what patients think they ingested isn’t always what they did ingest. A high percentage of “cocaine” and other stimulants was actually fentanyl or other opiates. The authors do a nice job referencing similar studies in the United States. Any overdose could be a mixed picture due to impure street drugs.
Perinatal HIV transmission in the U.S. can approach rates of <1% if appropriate interventions are offered to both pregnant individuals and their neonates.
However, a recently published case series evaluating hospitals in Maryland noted that there were 6 new cases of perinatal HIV transmission in 2022, compared with nationwide decreases and zero cases in the state of MD in 2021. Transmission was believed to be related to several issues: delayed entry to prenatal care, HIV diagnosis occurring in pregnancy (as opposed to pre-conception), adherence in the setting of hardships such as substance use, and delays in anti-retroviral therapy (ART) initiation during pregnancy.
How can we work to lower perinatal HIV transmission? Opportunities include the use of pre-exposure prophylaxis (PrEP), routine HIV testing in individuals of child-bearing age (especially if at high-risk of HIV acquisition), and rapid initiation of ART in pregnant individuals. As emergency physicians and providers, we are at the front line of assessing for these barriers and getting patients the resources they need to minimize perinatal transmission.
A 2023 retrospective cohort study comparing amiodarone to lidocaine for in-hospital cardiac arrests (IHCA) with refractory VT/VF found that use of lidocaine was associated with increased chance of ROSC, 24 hour survival, survival to discharge, and favorable neurologic outcome at hospital discharge.[1]
Now, a recent study comparing amiodarone to lidocaine in the pre-hospital setting for OHCA has found similar results. [2] Another retrospective cohort study using propensity score matching, they evaluated 23,263 adult patients with OHCA and defibrillation refractory VT/VF managed by 1700 EMS agencies.
Use of lidocaine was associated with greater odds of prehospital ROSC, fewer post-drug administration defibrillations, and greater odds of survival to discharge.
In comparison to earlier trials, these studies are some of the first demonstrating benefits to lidocaine use over amiodarone that reach statistical significance, but of course have all the limitations that come with retrospective studies and are not further analyzed in the context of etiologies for cardiac arrest or application of post-ROSC care.
Bottom Line: If you happen to be someone who reaches for amiodarone as your go-to, it may be time to start considering lidocaine.
The Jarisch-Herxheimer reaction (JHR) is a non-specific set of symptoms (fever, malaise, worsened rash, hemodynamic instability, leukocytosis) seen after treating syphillis and other spirochete induced infections. In this study 1 in 4 patients treated with 2.4 million units of benzathine penicillin G developed a short lived JHR. Those who developed the reaction were more likely HIV negative, had secondary syphillis and had successful treatment at 6 months.
A recent cohort study performed by the NCAA and US Department of Defense looked at NCAA athletes and military cadets who had suffered a concussion.
The study included 1661 NCAA athletes and military cadets, mean age was about 18 years, and 45% were women.
In these groupings, 813 people took over-the-counter pain relievers after their concussion and 848 people did not take any pain relievers.
Analgesics used included medications such as acetaminophen or NSAIDs such as ibuprofen.
Acetaminophen (n = 600), NSAIDs (n = 75), and those taking both (n = 78).
1) 50% recovery
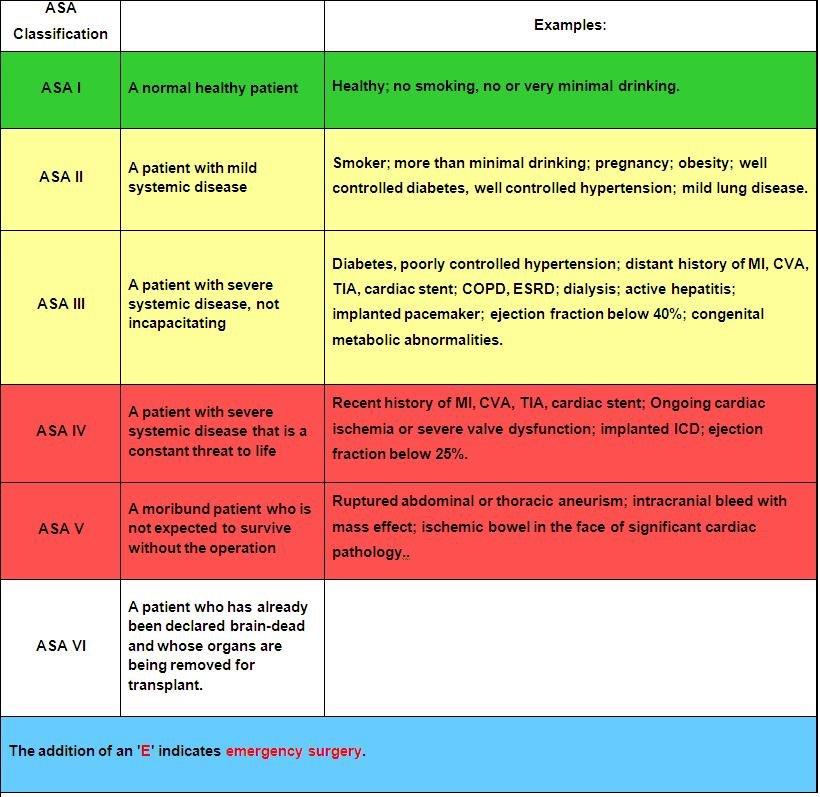
The American Society of Anesthesia score was an independent predictor of 90-day mortality as
well as low functional status at one year in 720 patients presenting to a single center with
moderate to severe brain injury. When used in conjunction with other prognosticating tools such
as the Trauma and Injury Severity Score, it increased the prognostic value of these scales.
Anticoagulation is the mainstay of treatment of cerebral venous sinus thrombosis, irrespective of whether associated venous hemorrhage is present. Anticoagulant selection is variable, with physicians opting for unfractionated heparin (UFH) about 72% of the time in one international study. However, recent evidence favors the use of low-molecular-weight heparin (LMWH), with meta-analytic data showing trends towards lower mortality rates and improved functional outcomes in LMWH cohorts. UFH is often viewed more favorably due to the ability to rapidly discontinue the infusion in the event of major bleeding; however, risk of major bleeding complications were actually found to be lower in patients treated with LMWH compared to UFH. Further, LMWH has many pharmacological and practical benefits compared to UFH, including more predictable pharmacokinetics, reduced risk of heparin-induced thrombocytopenia (HIT), lack of need for frequent aPTT monitoring, ease of administration (daily subcutaneous injection), and ease of transition to outpatient therapy.
Takeaway: Consider LMWH (1.5mg/kg subcutaneously once daily) as first-line treatment for CVST in patients with acceptable renal function.
Better teamwork creates better outcomes in emergency medicine. This study investigated how communication practices between physicians and nurses in the ED influence team dynamics and the sense of belonging to the healthcare team.
Methods: 38 emergency physicians and emergency nurses from EDs within a single metropolitan area participated in focus groups.
Positive Influences on Team Belonging:
Negative Influences on Team Belonging:
The findings emphasize the importance of fostering positive communication practices to enhance team dynamics, cohesiveness, and overall well-being within ED healthcare teams.
If you watch those medical drama (House MD, ER, Grey’s Anatomy, Resident…), the doctors and residents are always faced with a dilemma – is it a rare autoimmune disorder or is it an infection? They are worried that if they give steroid to a patient with infections, that would kill the patients.
Well, it might not be the case for Community acquired pneumonia.
A meta-analysis of randomized control trials involving 3224 patients to look into the efficacy of adjuvant corticosteroids for CAP. The authors assessed the heterogeneity of treatment effect (different groups should have different response to treatment).
For patients who were anticipated to benefit (those who had CRP > 240 mg/L), corticosteroids were associated with lower odds of 30-day mortality (OR 0·43 [0·25–0·76], p=0·026).
When stratifying by risk, there was no significant effect between those with Pneumonia Severity Index (PSI) I-III versus those with PSI IV-V.
However, corticosteroids increased odds of hyperglycemia (OR 2·50 [95% CI 1·63–3·83], p<0·0001), odds of hospital readmissions (1·95 [1·24–3·07], p=0·0038)
Discussion:
There were different regiments for corticosteroids in the included studies. However, hydrocortisone appeared to be more effective than other corticosteroids.
Furthermore, the time intervals for treatment is still debatable. The data suggested that the ideal treatment is within 24 hours of hospital admission, but patients can still benefit from treatment in up to 48 hours.
A response-dependent treatment is also recommended: 8 days or 14 days, depending on how patients respond to treatment by day 4.
Conclusion:
Adjuvant treatment with corticosteroids among hospitalized patients with CAP was significantly associated with reduction of 30-day mortality. The treatment effect, however, varied according to patients CRP concentrations at baseline.
Controlling pain from rib fractures impacts morbidity and mortality. Over the past decade there has been a focus on decreasing opiate use and approaching this painful condition in a multimodal way. “The multimodal approach utilizes a combination of delivery methods including oral, parenteral, and regional single-shot or catheter-based techniques. Oral medications include opioids, non-steroidal anti-inflammatory drugs (NSAIDs), acetaminophen, skeletal muscle relaxants, alpha-2 agonists, mood stabilizers, and neuropathic pain medications. Parenteral medications encompass most of the oral options in addition to ketamine and lidocaine. Regional anesthesia includes epidural analgesia (EA), paravertebral blocks, intercostal blocks, and myofascial plane blocks.”
This study is a single center in Canada looking at medication used for patients admitted over 10 years with rib fractures along with demographics, injury severity and outcomes. The authors concluded:
“Although multimodal pain management strategies have improved over time, a large proportion of patients, even among those with flail chest, still do not receive multimodal pain management. Elderly patients, at highest risk of adverse outcomes, were less likely to receive multimodal pain management strategies and should be the target of performance improvement initiatives.”

