Delirium in the ICU means badness as delirious ICU patients are associated with longer stay and higher mortality. While medications are not proven to prevent delirium, certain environmental interventions such as window access, light and sound levels have been recognized as legit interventions to prevent ICU delirium.
Settings: This is a retrospective study at Massachusetts General Hospital
Participants: 3527 patients admitted to a surgical ICU between 2020 and 2023.
Outcome measurement: This study hypothesized that patients in a windowed ICU room will have lower rates of delirium, decreased ICU length of stay, hospital LOS. Multivariable logistic regressions were performed for the association of clinical variables and the presence of delirium.
Study Results:
Delirium was observed in 460 patients (21%) of the windowed rooms group and 206 patients (16%) of the nonwindowed rooms group. Multivariable logistic regression showed that patients in windowed rooms were associated with higher odds of delirium (aOR, 1.29; 95% CI, 1.07–1.56; p = 0.008), although they were not associated with longer ICU LOS or longer HLOS
Discussion:
The study’s findings added to the literature that natural lighting might not be the effective prevention of delirium. The presence of windows might not be the answer.
In this study, all the windows were facing another building, and there was no view of other natural scenes, with a limited view of the sky. Therefore, the authors suggested that the overall quality of the windows would be more important.
Conclusion:
The ICU environment is more important for patients’ delirium than just the presence of windows.
Stellate Ganglion Blocks (SGB) have been reported in case reports as a last-line treatment for patients with refractory ventricular arrhythmias.
A recent multicenter study evaluated the efficacy and safety of SGB in managing refractory ventricular arrhythmias.
The study included 117 critically ill patients, with 9 on ECMO, 5 with Impella devices, and 15 with LVADs.
70% were given long-acting bupivacaine, 28% were given ropivacaine and 1 patient received lidocaine.
SGBs were primarily performed by anesthesiologists during short periods of when the patients were not in ventricular arrhythmia
The median 24-hour episodes of VT/VF decreased from 9.0 (interquartile range [IQR]: 3.0–31.0) pre-SGB to 1.0 (IQR: 0.0–5.0) post-SGB.
2 patients had complications; recurrent laryngeal nerve block with resultant hoarseness and brachial plexus block.
Limitations: This study was conducted in a controlled setting (ie not in active arrest, not in the emergency department) and involved a selective cohort. Randomized controlled trials (RCTs) are needed to validate these findings.
Fractures of the occipital condyles are a relatively rare injury that occur in high energy blunt mechanisms (IE roll over MVC) most commonly. Physical exam will show signs of basilar skull fracture and significant pain at the base of the skull/upper C-spine. CT scan is the gold standard to make the diagnosis. Look for signs of upper extremity weakness on physical exam or cranial nerve injuries. Those type of findings should also prompt emergent MRI evaluation. Treatment generally is long term immobilization in a collar however Type 3 and those with neurologic findings may require surgical intervention.
Anderson and Montesano Classification
Type I 3% of occipital condyle fracturesImpaction-type fracture with comminution of the occipital condyle
Due to compression between the atlantooccipital joint
Stable injury due to minimal fragment displacement into the foramen magnum
Type II 22% of occipital condyle fracturesBasilar skull fracture that extends into one or both occipital condyles
Due to a direct blow to skull and a sheer force to the atlantooccipital joint
Stable injury as the alar ligament and tectorial membrane are usually preserved
Type III 75% of occipital condyle fractures Avulsion fracture of condyle in region of the alar ligament attachment (suspect underlying occipitocervical dissociation)
Due to forced rotation with combined lateral bending
Has the potential to be unstable due to craniocervical disruption

This was a retrospective, multicenter cross-sectional study of pediatric sedations over 3 years using the Pediatric Sedation Research Consortium database.
85,599 pediatric sedations were included. These sedations did include the operating rooms.
8.7% of sedations required an intervention for airway/breathing/circulation in patients who did NOT have procedural oxygenation while 10.1% of patients in the group that did have procedural oxygenation required an intervention. The majority of these interventions were minor, ie airway repositioning. The group that did have procedural oxygenation did have a lower rate of hypoxia compared to the group without procedural oxygenation (2.5% vs 4.5%).
The authors concluded that preemptive procedural oxygenation did NOT decrease the overall need for interventions in the ABCs compared to no procedural oxygenation.
Intrathecal baclofen pumps are increasingly used to manage spasticity in patients with conditions such as cerebral palsy, spinal cord injury, multiple sclerosis, traumatic brain injury, and other dystonias. The most common causes of baclofen pump dysfunction include pump-related issues (e.g., programming errors, battery failure), catheter problems (e.g., extra-thecal dislodgement, kinking, leaks), and medication depletion (e.g., overdue or insufficient refills). Symptoms of dysfunction can be nonspecific, ranging from mild (spasticity, dysphoria, dysesthesias) to severe (e.g., rigidity, rhabdomyolysis, seizures, fever, autonomic dysfunction, cardiomyopathy).
Once dysfunction is recognized, management involves stabilizing vital functions (ABCs, temperature management, fluids), administering multimodal antispasmodics (enteral or parenteral baclofen, benzodiazepines, dexmedetomidine, tizanidine), and performing pump interrogation, often in collaboration with neurology or PM&R specialists. Restoration of intrathecal flow is the preferred and definitive therapy; however, patients with severe withdrawal may require aggressive temporizing measures including intubation. Some authors describe intrathecal baclofen administration via lumbar puncture as a rescue measure for severe cases with limited access to definitive care. Imaging with plain radiographs, fluoroscopy, or CT may be indicated in select cases where there is concern for catheter displacement or kinking, and some patients may require surgical revision.
Takeaway: Consider baclofen withdrawal in patients on chronic baclofen therapy who present with nonspecific symptoms that may mimic conditions such as alcohol withdrawal, delirium, sympathomimetic toxicity, neuroleptic malignant syndrome, serotonin syndrome, thyrotoxicosis, rhabdomyolysis, sepsis, or status epilepticus. In cases of intrathecal pump dysfunction, the definitive treatment is restoration of baclofen flow, so involve consultants early for pump interrogation while temporizing with supportive measures.
Previous studies have shown that an on scene time of 10-35 minutes was associated with improved survival in pediatric out of hospital cardiac arrests compared to an on scene time of > 35 minutes. There was no significant difference in overall survival between < 10 minutes and 10-35 minutes of on scene time.
This study involved a total of 2854 pediatric cardiac arrests in the US and Canada. The patients who had a cardiac arrest during transport were compared to patients who received on scene CPR by equal minutes.
Among patients < 1 year, intra-arrest transport was associated with lower survival to hospital discharge compared to those that were resuscitated on scene. There was no association for patients > 1 year.
Bottom line: This study supports resuscitating in place for pediatric cardiac arrests, especially in patients < 1year.
These 2 papers challenge management dogmas in critical care that have persisted despite low-quality/absent evidence.
In particular, one explores the dogma, “bicarbonate improves ventricular contractility in severe metabolic acidosis,” with the following points:
-intracellular pH (which has a large impact on myocardial contractility) correlates poorly with blood gas pH
-many of the studies regarding bicarbonate in severe metabolic acidosis and hemodynamics are done on animal shock models
-two studies in patients with lactic acidosis showed increase in pH with bicarb administration without beneficial impact on hemodynamics (even in pts with pH < 7.1)
-bicarb administration is associated with hypernatremia, hypokalemia, and decreased ionized calcium levels
This meta analysis of studies looking at thrombolytics and prostaglandins in treating significant frost bite offers some insight into the possibilities these therapeutics offer. Unfortunately, the studies available are not high quality and most are case reports.
“Our results suggest that thrombolysis or intravenous iloprost is effective when administered promptly to treat severe frostbite. For grade 3–4 frostbite the Wilderness Medical Society frostbite guidelines recommend the use of intravenous iloprost within 48 h of injury, and thrombolysis within 24 h of injury. The Helsinki protocol recommends the use of tPA for patients with grade 3–4 frostbite presenting within 48 h of injury with angiographic evidence of thrombosis."
“Iloprost is a synthetic prostaglandin I2 that has been used to treat frostbite . Like other prostacyclins, it inhibits platelet aggregation and promotes vasodilation. Iloprost may stimulate the release of endogenous tissue plasminogen activator or counteract its inhibitory effects [35]. Iloprost reduces vasoconstriction induced by thromboxane A2 , and may reduce oxidative stress from free radicals, moderating reperfusion injury [37, 38]. The effect on platelet aggregation may be reversed within two hours), but prostacyclin effects may disrupt the vicious cycle of activated platelets and leukocytes that damages endothelium .”
More research in this area is needed. Transfer to a center with these capabilities seems worth a discussion in the case of severe frostbite.
The Trauma Frailty Index has been validated to predict inpatient mortality, major complications and discharge to rehab facility. “In addition, frailty was significantly associated with higher adjusted odds of mortality, major complications, readmissions, and fall recurrence at 3 months postdischarge ( p < 0.05).”
It is a simple 15 variable index.

Background
Treatment of acute agitation often involves combining antipsychotics and benzodiazepines. Injectable olanzapine, a second-generation antipsychotic, uniquely carries a warning against concomitant use with parenteral benzodiazepines. The olanzapine prescribing information states that “concomitant administration of intramuscular (IM) olanzapine and parenteral benzodiazepines is not recommended due to the potential for excessive sedation and cardiorespiratory compromise”. The European Medicines Agency (similar to the United States FDA) cautions against use of the two within 60 minutes of each other using similar language.
The above warnings were based on a 2010 publication of 160 adverse event reports from a post-marketing database maintained by the drug manufacturer, and have resulted in many institutions prohibiting co-administration of IM olanzapine and parenteral benzodiazepines. The publication cited 29 fatal adverse events involving injectable olanzapine, concluding that caution should be exercised when using IM olanzapine and parenteral benzodiazepines simultaneously. However, 25 of the 29 patients received other sedating medications in addition to olanzapine and benzodiazepines, and the majority of fatalities were >12 hours after the last dose of olanzapine. Following this publication, a 2013 randomized controlled trial by Chan et al. found no difference in adverse event rates between patients receiving IV midazolam alone and patients receiving IV midazolam plus IV olanzapine for acute agitation.
This December 2024 study by Cole et al. aimed to re-evaluate the risks of cardiorespiratory compromise with concomitant injectable olanzapine and injectable benzodiazepine administration.
Study design
This was a single-center retrospective cohort study of 693 patients who received 2 parenteral doses of eligible sedating medications within 60 minutes of each other. A total of 549 patients received 2 doses of olanzapine, and 144 received olanzapine and a benzodiazepine (midazolam, lorazepam, or diazepam). To avoid cohorts with a higher baseline risk of sedation, patients who received other sedating medications and patients who received more than 2 doses of olanzapine or 1 dose of a benzodiazepine were excluded.
Patient Population
Results

*One death during hospitalization was due to missed occlusion myocardial infarction
Study Critique:
Key Takeaways
Extracorporeal cardiopulmonary resuscitation (ECPR) is a type of extracorporeal support following cardiac arrest available at a small, but growing number of ECMO centers around the world. After some initial promising results, more recent data have been mixed. There is a nice narrative review in JACEP Open recently which summarizes the most recent evidence. Implementation considerations and patient selection seemingly drive the variance seen in the studies reviewed.
To this point, a new article from Critical Care Medicine was just published looking at the outcomes of eCPR with respect to age using 5 years of ELSO patient data. Unsurprisingly, advancing age is associated with worse outcomes, with significantly reduced odds of survival above the age of 65.
The level of fitness/health a patient has entering the marathon of recovery from critical illness or trauma has a major impact on morbidity and mortality. Frailty is a measure of this fitness level. The clinical frailty scale can be used to assess your patients ability to survive critical illness. Age is a number. Frailty is more useful.


This study followed patients presenting to the ED with elevated (SBP>180, DBP>120) blood pressure without evidence of end organ dysfunction for one year. The patients were followed for major adverse cardiac events. They found:
“A total of 12,044 patients were enrolled. The prevalence of MACE within one year was 1,865 (15.5%). Older age, male gender, history of cardiovascular disease, cerebrovascular disease, diabetes, smoking, presentation with chest pain, altered mental status, dyspnea, treatment with intravenous and oral hydralazine, and oral metoprolol were independent predictors for one-year MACE. Additionally, discharge with an SBP ?160 mm Hg was not associated with 30-day MACE-free survival after propensity matching (hazard ratio 0.99, 95% confidence interval 0.78–1.25, P?=?0.92).”
Treating to reach a magic number did not help. Most likely, long term control of blood pressure is a more important factor than attempts to lower in the ED. While this is a high risk group, there is no evidence that acute lowering of blood pressure impacts long term survival.
Post-Intensive Care Syndrome (PICS) is an increasingly recognized phenomenon of impairment of physical, cognitive, and/or mental health after intensive care admission. Even more recently, similar deficits in caregivers of patients admitted to the ICU, often called Post-Intensive Care Syndrome Family (PICS-F) is increasingly recognized. A study recently published by Watland et al in Critical Care Medicine looking at reducing PICS-F through a “caregiver pathway” got me wondering if there's any literature out there about reducing PICS-F via interventions in the emergency department. Patients' treatment course in the ED is a highly stressful and uncertain time for both the patient and family members, so it stands to reason this is an impactful period where intervention may help, and even in patients where their condition is too advanced for us to make a medical difference, our actions could have a positive impact on long term outcomes for the family members.
The short answer is no, to this author's knowledge and based on my review of the literature, there is no good evidence for reducing PICS-F by ED interventions (hint, hint: if anyone's looking for a good area to study…) Based on evidence from the critical care realm, the following are probably reasonable approaches that would translate well to the ED:
This study suggests no. The control arm was given standard physical therapy and the intervention arm was instructed in four basic exercises to do on their own daily for a week. Patents were then surveyed to assess for long term pain. There was no difference in pain between the two groups. Meaning, at least in this study reliant on patient journaling and follow up, that these four simple exercises did not impact long term pain in chest wall injured patients. More work needs to be done in this important area.
In a fascinating perspective piece, Matt Bivens and colleagues explain that the combination of struggle and restraint leads to death not because of hypoxia, but because of acidosis.
The sequence is something like this: exertion or struggle results in an acidotic state -> restraint reduces respiratory ability, especially when held prone or weight is applied to back or chest -> acidosis worsens with the potential for cardiac arrhythmia and arrest.
In this setting, “I can’t breathe” does not mean that there is no air movement over the vocal cords but that respiration is impaired, much as it is in asthma or obstructive lung disease.
Use of sedation in this setting reduces respiration even further, worsening acidosis and risking death. It’s not hypoxia that kills; it’s acidosis.
See the complete perspective here: https://www.nejm.org/doi/full/10.1056/NEJMp2407162.
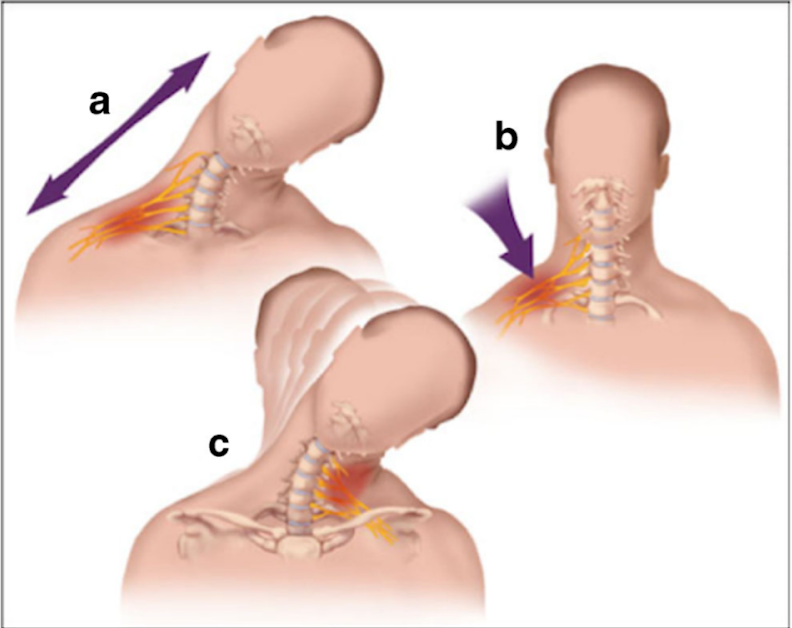
A stinger is a short lived neuropraxia to the upper brachial plexus
Named for the temporary sensation that radiates from the shoulder to the hand
Can occur though 3 common mechanisms
Most commonly from direct traumatic or tractional injury
https://www.physio-network.com/wp-content/uploads/2021/11/unnamed-1.png
Common in American Football
Occurs in almost 50% of players over a 4-year college career
Most commonly to running backs and linebackers in one NFL study
Symptoms: Unilateral burning pain and tingling in the arm with transient weakness
Symptoms NOT confined to a single dermatome.
Usually in C5, C6 innervated muscles (deltoid and biceps).
Symptoms are transient usually resolving in approximately 2 minutes
If asked to examine someone for this at a sporting event
Evaluate patient for:
C spine tenderness
Full cervical range of motion
UNILATERAL weakness in shoulder Abductors and external rotators
UNILATERAL weakness in biceps
UNILATERAL weakness in forearm pronation
UNILATERAL weakness in triceps extension
Consider evaluation for concussion symptoms if appropriate
Majority of patients in college and profession sports return to play in game when exam returns to normal
Clinical practice in the world of the Electronic Medical Record has made many a clinician question the value of electronic reminders.
Banners warn of sepsis, the need for repeat evaluation, vital signs outside expected limits, wait times, and risks for readmission.
Can they instead help ED flow?
Sayan Dutta and colleagues suggest that they can. When clinicians chose to receive notice of a lab or imaging result, push notification reduced time between final result and ED disposition by 18 minutes (95% CI: 15-21 minutes).
The likely key here? Clinicians actively chose when and about what to be notified.
See: Result Push Notifications Improve Time to Emergency Department Disposition: A Pragmatic Observational Study, Annals of Emergency Medicine, 85(1), 53-62. https://www.annemergmed.com/article/S0196-0644(24)00404-9/abstract.
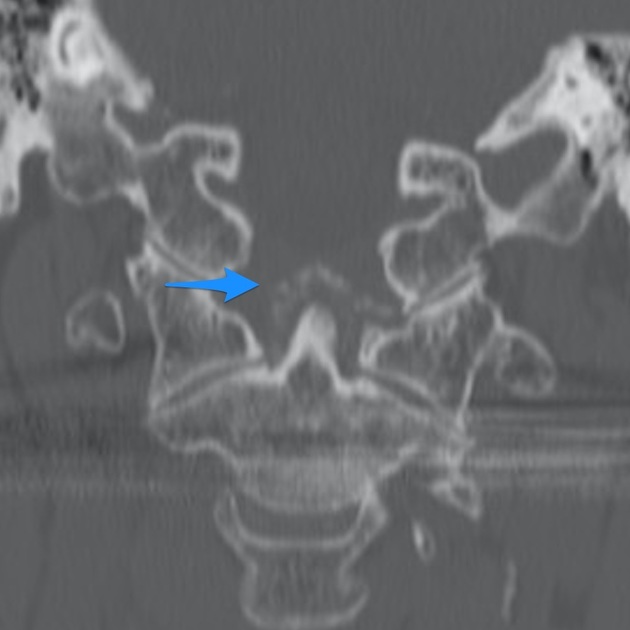
Crowned dens syndrome is an acute inflammatory disease caused by deposition of calcium pyrophosphate dihydrate crystals or hydroxyapatite crystals in the soft tissue and ligaments surrounding the dense. Patient presentation is severe pain in the neck and base of the skull, low grade fever, and elevated inflammatory markers. It is most commonly seen in elderly females. Ct scan is the gold standard for diagnosis. Once meningitis and other significant infectious process has been excluded, treatment is anti inflammatory medications including steroids.
{kind=link}
{kind=link}
{kind=link}