2024 brought us an excellent new decision tool to prevent excessive radiation for children. NOTE: These are vastly different than adult criteria.
In children with traumatic injuries, most will NOT require CT imaging.
This study included over 22,000 patients (age 0-17 years) who were evaluated following blunt trauma. A rate of <1% were found to have c-spine injuries. Excluded from the study were strangulation patients, intoxicated patients, and predisposing conditions including prior fracture.
Indications for considering CT C-spine include ANY of the following:
Indications for consider C-spine XRs include ANY of the following:
Abnormal XR findings should receive further evaluation as per standard of care.
The remaining patients may have their c-spine cleared.
Background:
The 2010 Infectious Diseases Society of America (IDSA) cystitis and pyelonephritis guidelines recommend fluoroquinolones (FQs) as first line agents for pyelonephritis treatment and also support trimethoprim-sulfamethoxazole (TMP-SMX) usage if the urinary pathogen is known to be susceptible. However, alternative regimens need to be evaluated as FQs are increasingly associated with serious adverse events, and E coli resistance rates to both FQs and TMP-SMX are rising nationally. The Cephalosporins for Outpatient Pyelonephritis in the Emergency Department (COPY-ED) study aimed to evaluate the effectiveness of oral cephalosporins in acute pyelonephritis treatment when compared to IDSA guideline-endorsed first line treatments.
Study design:
This multicenter, retrospective observational cohort study screened patients with a primary diagnosis of uncomplicated or complicated pyelonephritis using ICD-10 codes. They included all patients >18 years of age who reported symptoms of a UTI and were discharged home on oral antimicrobial therapy. Exclusion criteria included pregnancy, acute or chronic prostatitis, orchitis, epididymitis, or urinary tract surgery within 7 days prior to ED visit or surgery planned during the study period.
The primary outcome was rate of outpatient treatment failure within 14 days of discharge from the emergency department with cephalosporins compared to FQs and TMP-SMX.
Patient Population:
Results:
Rates of treatment failure at 14 days were not statistically significant between groups, with a rate of 17.2% in the cephalosporin group and a rate of 22.5% in the FQ + TMP/SMX group. After adjusting for gender, complicated infections, previous use of intravenous or oral antibiotics, and urinary tract abnormality, the odds of treatment failure at 14 days were still not significantly different in patients who received fluoroquinolone or TMP/SMX (adjusted OR 1.275 [95% CI 0.86 to 1.9]) compared to cephalosporins.
Secondary outcomes included rates of treatment failure with first generation cephalosporins (cephalexin, cefadroxil, cefuroxime) and third generation cephalosporins (cefpodoxime, cefuroxime), rates of appropriate therapy selected based on urine culture susceptibilities, and rates of treatment failure compared to duration of treatment prescribed. None of these outcomes found statistically significant differences between groups.
Study Limitations:
Key Takeaways:
This article reminds us that hip fractures have a one year mortality rate of 12-25% and 50% of hip fracture patients develop complications while in the hospital. “Almost half of individuals hospitalized with hip fractures experience complications, such as delirium, pneumonia, acute kidney injury, urinary tract infection, and deep vein thrombosis”
Because of these complications, multidisciplinary teams should be caring for these patients and great care should be exercised when evaluating these patients.
Duan et al recently published in Intensive Care Medicine the results of a trial looking at a PEEP of 5 cm H2O vs 10 cm H2O and impact on failure rate (progression to intubation) when using non-invasive ventilation (NIV). In their trial, the high PEEP group had a lower rate of intubation (32% vs 43%), and this was statistically significant. It is important to note that they excluded patients whose indication for NIV was heart failure, asthma, or COPD exacerbation.
Ultimately, how to choose the right PEEP is a very complex question and requires tailoring to your patient's physiology and clinical circumstances. For example, hypercarbic patients may benefit more from a maximization of their driving pressure (Pplat - PEEP), which can involve lowering their PEEPs, especially when trying to avoid gastric insufflation (remember, pressures of 30 cm of H2O or higher are very likely to open the LES).
Bottom Line: PEEP and other vent settings should be tailored to the patient's pathophysiology, but this trial suggests that in hypoxemic patients not getting NIV for heart failure, asthma, or COPD exacerbation, a higher PEEP (10 vs 5) may reduce the risk of intubation.
The normal gallbladder dimensions on ultrasound are approximately 3 cm in width by 10 cm in length.
A recent study evaluated the diagnostic test characteristics of gallbladder distension on POCUS for cholecystitis.
The authors conducted a retrospective cohort study of 227 patients who were admitted to the hospital after undergoing a POCUS biliary study in the emergency department.
They found the prevalence of gallbladder distension to be 30% in their study population. When combined with other sonographic findings, the presence of distension increased the specificity for cholecystitis to 95.6%.
Gallbladder wall distension was associated with the presence of an obstructing stone in the gallbladder neck and with acute cholecystitis.
Additionally, gallbladder wall distension was associated with longer operative times (mean 114 minutes) compared to those without distension (mean 89 minutes; p=0.03), suggesting more severe disease and potentially more complex surgical intervention.
Bottom Line: When gallbladder wall distension is present, it is important to carefully evaluate the gallbladder neck for signs of an obstructing stone.
Aortic dissection remains a difficult diagnosis to make. This article is a nice review. The pathology behind this involves an intimal flap in the aortic wall. Death occurs due to aortic rupture or obstruction of branching artery.
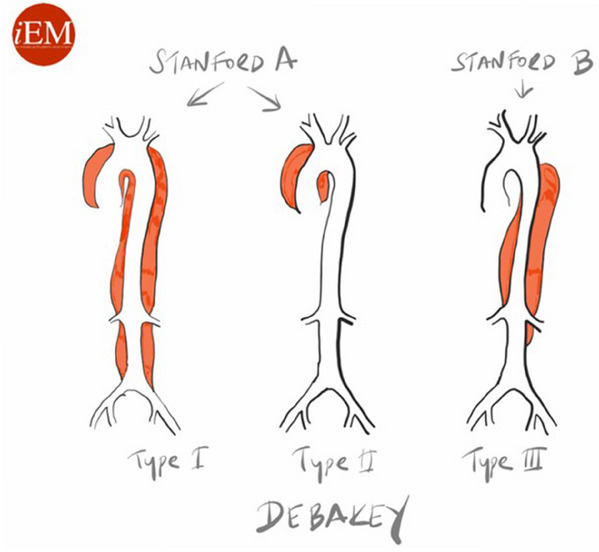
Risk factors: male 2:1 female, Marfan Syndrome, HTN, aortic aneurysm, cocaine and methamphetamine use, pregnancy
Pain is variable however tearing, ripping migrating, maximum at onset, and sharp are all associated with Aortic Dissection. Think about Dissection with atypical CP with ECG changes as well as in stroke like presentations along with chest pain.
Gold standard for diagnosis is CT angiogram. Decision rules with the use of D-Dimer have been proposed however there is still not sufficient evidence to use these. ACEP guidelines currently give use of decision rules a long with DDImer a level C recommendation.
A study published in the NEJM (March 2025) looked at recurrence of bacterial vaginosis at 12 weeks in two groups: a control group where women received standard treatment but male partners were not treated, and a partner-treatment group. In the partner-treatment group, women received standard treatment, and the male partner received both oral and topical treatment. Male partners in this study received Metronidazole 400 mg BID x 7 days in addition to 2% topical clindamycin cream applied to penile skin BID x 7 days. The trial was actually stopped early as it was found that only treating the female was inferior to treatment of both.
This study concluded that treatment of both the female and male partners led to significantly decreased recurrence of bacterial vaginosis within 12 weeks (35% with dual treatment vs. 65% with female-only treatment). This study suggests that we should consider offering treatment to both sexual partners for patients presenting with bacterial vaginosis.
Sedation for the Mechanically Ventilated Adult ICU Patient
This study looked at exposure to gun violence and found increased use of mental health resources, depression and suicide risk even with a single exposure. Repetitive exposure increased suicide risk as well as mental health service utilization, depression and overall health service utilization. While further work is needed, screening our patients for gun violence exposure could undercover mental health needs.
In the April edition of Annals of EM, there are opposing view points on the optimal antibiotic regiment for necrotizing soft tissue infection. One group proposes linezolid alone will cover all the worrisome pathogens namely group A Strep and Staph. There are less side effects including C. Diff infection with this medication. Another group suggests sticking to vancomycin plus/minus BLactam along with clindamycin. Their arguement centers around clindamycin is useful as an antitoxin more so than its antibacterial property.
Both offer reasonable evidence and neither is compelling enough to say one is superior to the other.
Pseudo-Brugada pattern in hyperkalemia
Category: ECG
By: Chuck Siegel
Keywords: Brugada sign, hyperkalemia, ECG, arrhythmia
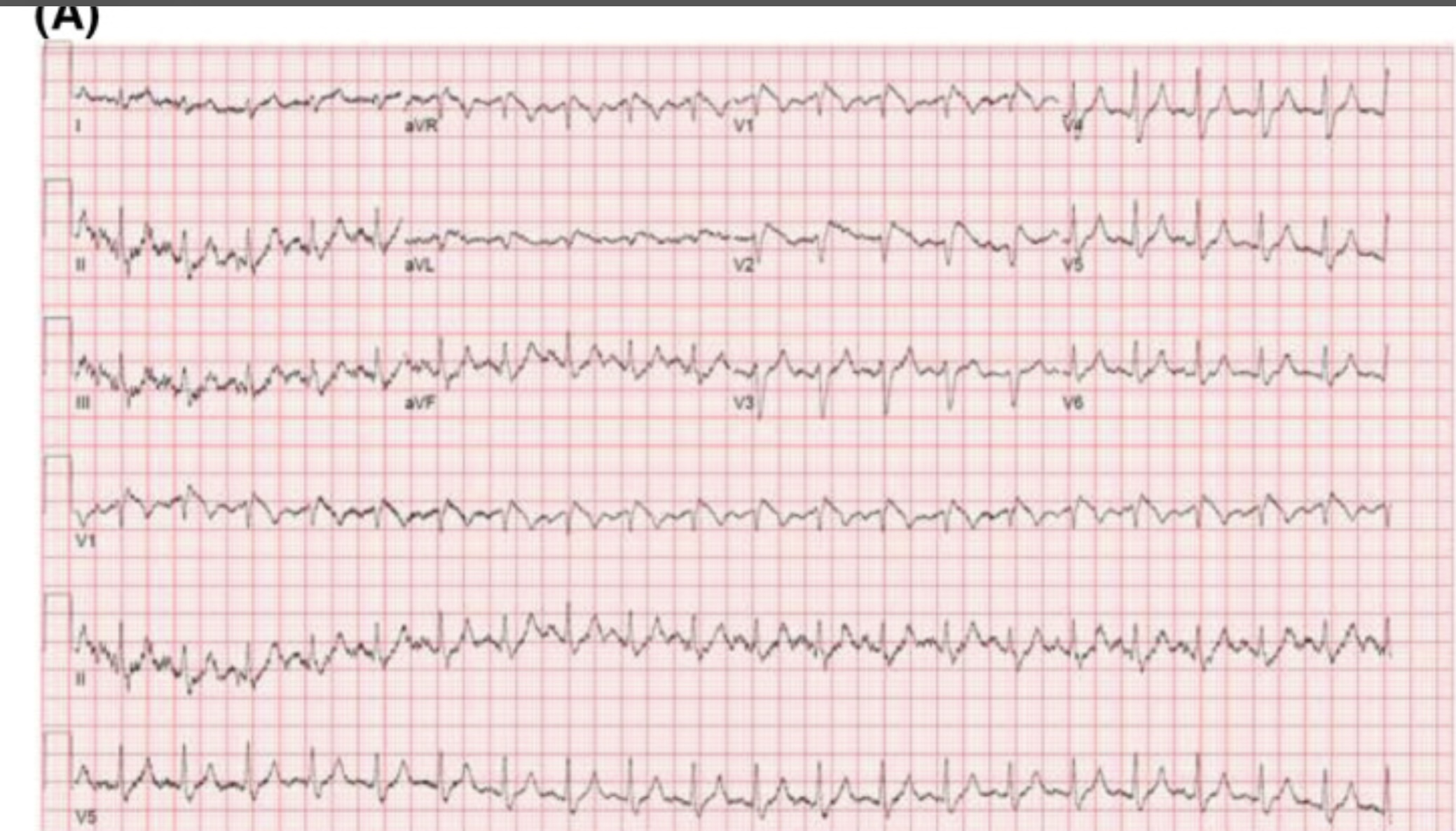
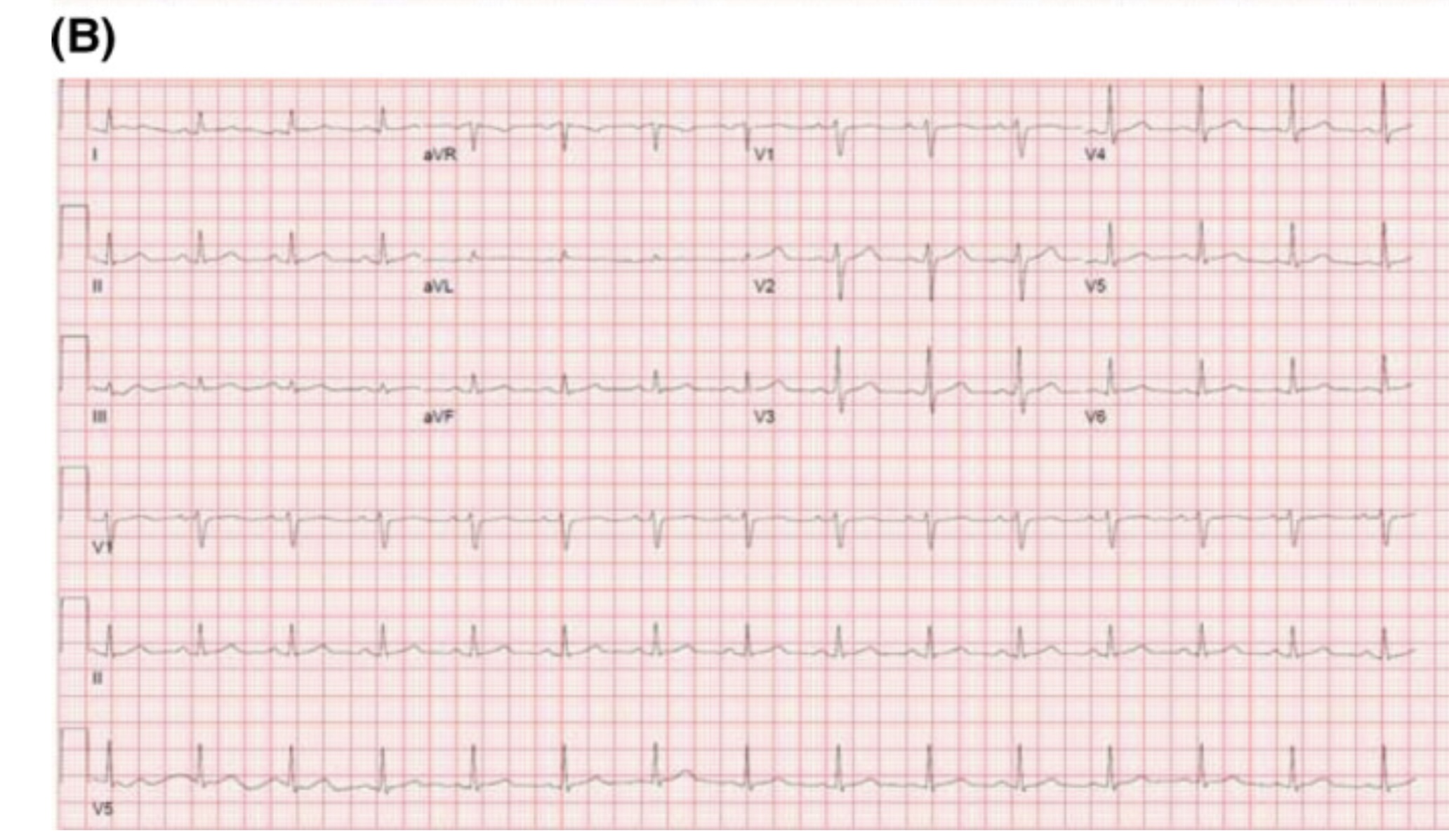
Hyperkalemia can produce a variety of ECG changes, including well-known changes such as peaked t-waves, QRS widening, PR-interval prolongation, loss of the p-waves, and the sine wave morphology. One change not as commonly seen is coved ST-elevation in V1-V3 that mimics the ECG changes associated with Brugada sign. Unlike Brugada syndrome, these ECG changes are transient and resolve upon treatment of the hyperkalemia.
The mechanism of these ECG findings relate to the elevated extracellular potassium’s inactivating effect on sodium channels, similar to the sodium channelopathy found in Brugada syndrome. The mean serum potassium concentration of reported cases is often above 6.5 mEq/L. Importantly, hyperkalemia-induced Brugada pattern has not been associated with sudden cardiac death or ventricular arrhythmias.
An example of a hyperkalemia-induced pseudo Brugada pattern in a patient with a K of 7.2 mEq/L (A) as well as that same patient’s ECG following treatment of their hyperkalemia (B).
You may have seen the headline.
93 million CT examinations conducted on 62 million US patients in 2023 projected to lead to 103000 new cancer diagnoses accounting for 5% of new cancers.
The details of the modeling can be found here, https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2832778.
What does this have to do with administration?
The solutions rely on administrative involvement:
There’s an editorial here, https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2832782 and a commentary with interviews that put the findings nicely in context here https://arstechnica.com/health/2025/04/ct-scans-could-cause-5-of-cancers-study-finds-experts-note-uncertainty/ (including pointing out that lifetime risk of cancer in the US is 40% and the increase from CT scanning on the order of 0.1% / scan).
This large RCT compared High-Flow Nasal Oxygen (HFNO) against Noninvasive Ventilation (NIV) via face mask in 5 types of Acute Respiratory Failure (ARF): non-immunocompromised hypoxemia, immunocompromised hypoxemia, COPD with acidosis, acute cardiogenic pulmonary edema (ACPE), and COVID-19.
Bottom Line:
RENOVATE suggests HFNO might be a reasonable, more comfortable initial choice for non-immunocompromised hypoxemic ARF or COVID-19 ARF. However, exercise caution using HFNO first-line for COPD exacerbations with acidosis or immunocompromised hypoxemic ARF due to conflicting analyses and potential harm signals. The signal for HFNO benefit in ACPE is intriguing but needs confirmation before changing practice. Close monitoring for failure and timely escalation are essential regardless of the initial noninvasive strategy.
This study looking at the type of facility that cared for rural injured patients reminds us that the majority of trauma care for rural patients occurs in non-trauma centers. This included some of the most severely injured and for many definitive care was received at these centers.
This may lead to lack of inclusion in trauma registries and under valuing the care being delivered by non-trauma centers. Protocols to facilitate transfers, air medical protocols and availability along with tele-health all are important in rural trauma care. Non-trauma designated centers are a critical part of the trauma network for rural residents and their value can not be ignored.
This study was the first look at the author's experiences with racial disparities in head and neck trauma in children. It looked at community EDs, and found that white children were more likely to be diagnosed with concussion compared to black children. White children were more likely to be seen as a result of sports or motor vehicle accidents, while black children were more likely to be seen as a result of an assault.
This study revealed the need for further research into the cause of the disparities in care that they identified.
Have you been wondering what the latest pediatric emergency medicine lecture says?
See the attached table from this review which highlights the 10 top articles from 2024 with their key findings!
Pulseless electrical activity (PEA) is the initial rhythm in up to 25% of out of hospital cardiac arrests.
This paper is a systemic review and analysis examining if the rate or width of the initial PEA qrs complex was associated with survival. The qrs complex was either wide (>= 120 ms) or narrow (<120ms) and a frequency of fast (>= 60/s) or slow (<60/s). 7 studies including 9727 patients were included. Analysis showed:
- mortality was higher in the wide qrs group compared to narrow
- mortality was higher in the slow PEA rate compared to fast
- neurological outcome was better in patients with a fast PEA rate compared to slow.
Emergency contraception comes in multiple forms, all of which have their own side effects and best case use scenarios that emergency medicine providers should be aware of to offer the best counseling.
Consider your patient before advising - if their BMI is > 25, consider ulipristal. If they want the most effective method, that'll be a copper IUD - but make sure they can get an appointment within 5 days of the unprotected intercourse! If they cannot afford ulipristal or levonorgestrel (which can both be $50 without insurance), but they already have OCPs, combining OCPs to the total noted above can be a method of emergency contraception that is still very effective.
Background:
Acetaminophen can reduce hemoprotein induced oxidative damage. There has been growing discussion about its benefits in critically ill patients with sepsis. Multiple observational studies have found conflicting results on mortality in critically ill patients with sepsis. The ASTER trial found no difference in number of days alive and free of organ support. Interestingly their secondary outcomes found significantly less development of ARDS in the acetaminophen group 2.2% vs 8.5%, p = .01. There was also a non-statistically significant difference in mortality between the groups in favor of the acetaminophen group, 17% vs 22% p = 0.19. This study looked to further evaluate if acetaminophen used in critically ill patients with sepsis would have a decrease in mortality and increase in ventilator free days.
Study:
- Retrospective analysis of the Ibuprofen in Sepsis Study (ISS)
- The ISS was a randomized clinical trial comparing ibuprofen with placebo in critically ill patients with sepsis. Careful documentation of Acetaminophen use was recorded for the trial
- Critically-ill adults across 7 ICU’s in the US and Canada with known or suspected infection and severe organ dysfunction
- Acetaminophen use within 48 hours of enrollment = Acetaminophen exposed
- Primary outcome: 30-day mortality
- Secondary outcome: Renal failure and ventilator free days up to day 28
- 455 patients. 172 Acetaminophen unexposed, 235 Acetaminophen exposed.
Results:
- Propensity-matched analysis showed a lower mortality risk at 30 days in patients exposed to acetaminophen compared to unexposed, 32% vs 49% (HR 0.58, p .004)
- Secondary outcomes found acetaminophen exposed group had more ventilator free days (p .02) but there was no difference in renal failure among the groups.
Limitations:
- Major risk for confounding variables
- Retrospective and the data used was from decades ago (1989 -1995). Sepsis care has evolved and improved since this time
- Dose and frequency of acetaminophen administration was not standardized
Take Home Points:
- Interesting research that provides further support on the possible benefit to using acetaminophen in the management of critically ill patients with sepsis.
- With the ASTER trial showing a signal for the decrease in development of ARDS and this study showing improvement in mortality one could make a case for starting acetaminophen early in the course for these patients. However, the data is conflicting and more prospective, RCT’s are needed to confirm these findings before making this a staple for sepsis care in critically ill patients.
This study looked at pre-trauma mental health diagnosis (from medical records) and post-trauma mental health symptoms as assessed by survey. The majority of patients suffered blunt trauma and mean age was 67. Having pre/traumatic mental health diagnosis and particularly post-traumatic symptoms lead to worse health outcomes and financial conditions. Further work needs to be done to assess how to improve mental health symptoms post-traumatic injury.