A fentanyl patch contains 100-fold more fentanyl in the reservoir than what is posted on the patch. For instance, 100mcg/hr patch will have over 10mg - thats milligrams - of fentanyl. This provides a rather large source for potential abuse. Overdose and deaths have occurred by patients in the following ways:
It is the many
(Sorry for the previously mislabeled pearl...)
Necrotizing soft tissue infections (NSTI) are on the rise and, despite improved surgical and critical care, over the years there has only been a mild reduction in mortality. Survival is associated with early diagnosis and treatment. Unfortunately, NSTI are not always obvious because deeper tissues made be involved first. Despite a validated scoring system and better radiology, our clinical suspicion still rules and relies on a meticulous history and physical exam.
Here are some subtle signs of NSTI:
Pain out of proportion to exam
Edema beyond region of erythema
Skin anesthesia
Skin erythema and/or hyperthermia
Epidemolysis
Skin bronzing
If NSTI is suspected, be vigilant! Start broad-spectrum antibiotics, begin appropriate resuscitation and involve your surgeons early.
17-18% of cases of syncope are attributable to arrhythmias
The greatest predictors of arrhythmias as the cause of syncope are:
a. Abnormal ECG (odds ratio 8.1)
b. History of CHF (odds ratio 5.3)
c. Age older than 65 (odds ratio 5.4)
[Sarasin, et al. Academic Emergency Medicine 2003]
Supraspinatus: “Empty can” test. Have the patient abduct the shoulders to 90 degrees in forward flexion with the thumbs pointing downward. The patient attempts to lift the arms against the examiner’s resistance.
http://bjsportmed.com/content/42/8/628/F2.large.jpg
Infraspinatus and teres minor: These muscles are responsible for external rotation of the shoulder. Have the patient flex both elbows to 90 degrees while the examiner provides resistance against external rotation.
http://www.physio-pedia.com/images/4/4b/Infraspinatus_test.jpg
Subscapularis: “Lift-off” test. The patient rests the dorsum of the hand on the lower back (palm out) and then attempts to move the arm and hand off the back. Patients with tears may be unable to complete test due to pain.
http://www.aafp.org/afp/2008/0215/afp20080215p453-f4.jpg
As RSV season approaches, remember these key points in managing bronchiolitis:
In the setting of acute cyanide poisoning, it is virtually impossible to obtain a timely cyanide level to help assess toxicity. However, there are two diagnostic tests that can help confirm your diagnosis.
Remember cyanide halts cellular respiration meaning the cells cannot utilize oxygen. Therefore, the venous PO2 should be about the same as the arterial PO2. The cells then switch to anaerobic metabolism, thereby producing lactate.
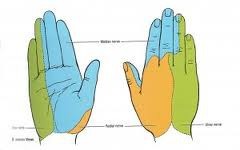
How to Perform a Median Nerve Block
Pulmonary Contusion and Ventilator Management
Acute use of cocaine increases risk of acute MI due to tachydysrhythmias, vasospasm, and increased platelet aggregation. There is a 24-fold increased risk of MI in the first hour after use of cocaine. 6% of patients presenting with cocaine-chest pain rule in for acute MI.
[Weber, Acad Emerg Med 2000]
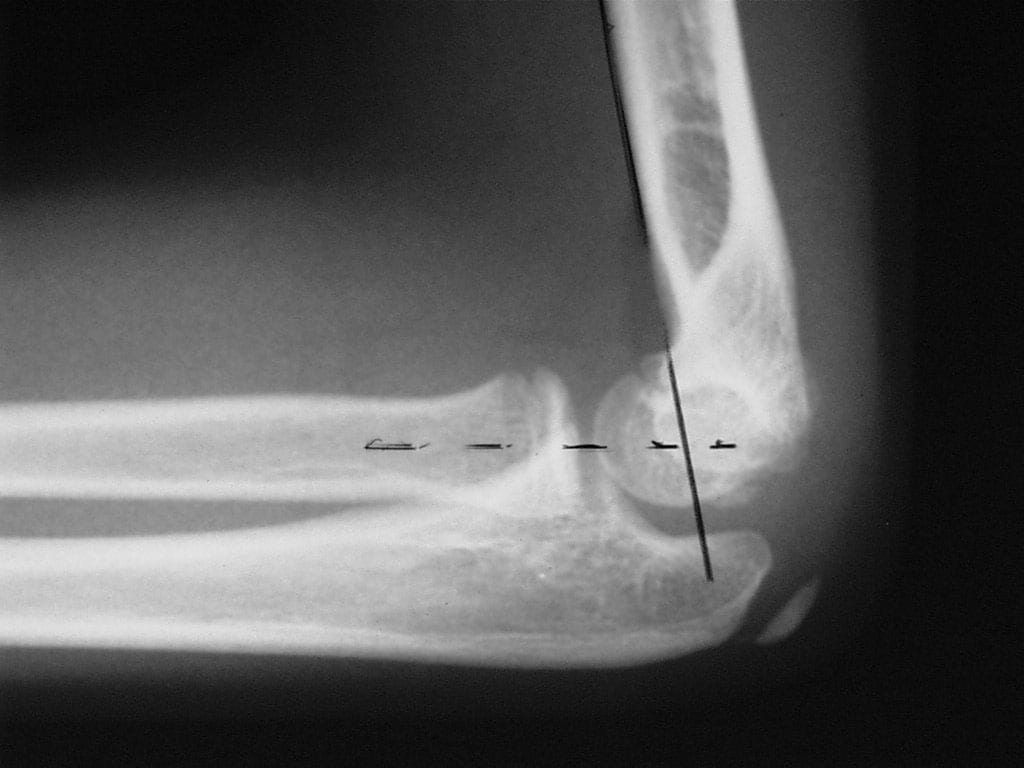
Radiologic evaluation of the elbow (Part 2)
Helpful clues in the evaluation of elbow trauma:
A recent study examined the effects of accidental digital epinephrine injection from auto-injectors. 127 cases with complete follow-up had the following effects:
Pharmacologic vasodilators were used in 23%. Four patients had possible digital ischemia. All patients had complete resolution of symptoms, most within 2 hours. No patient was admitted, received hand surgery consultation, or had surgical care.
Although this speaks for the safety of digital anesthesia using epinephrine, it underscores the importance of providing education to patients who are prescribed epinephrine auto-injectors.
Hyponatremia plagues many neurosurgical patients due to the syndrome of inappropriate secretion of ADH (SIADH) or the cerebral salt wasting syndrome (CSW). Both diseases may appear similar (hyponatremia, increased urine osmolarity, increased urine sodium, normal adrenal, renal and thyroid function), but there is one BIG difference. Patients with SIADH are euvolemic or hypervolemic (excess ADH causes fluid retention) whereas patients with CSW are fluid depleted (impaired renal handling of sodium and water). To differentiate, look for signs of hypovolemia: orthostatics, dry mucus membranes, hemoconcentration, pre-renal azotemia, and/or hemodynamics (IVC collapse anyone?).
Bottom line: Distinguish SIADH from CSW because the treatments are exact opposites:
SIADH: Fluid restrict
CSW: Give water and salt (i.e., 0.9% saline)
Hypertensive Encephalopathy (HE) is a clinical diagnosis and can look like many other disease entities.
HE refers to a relatively rapidly evolving syndrome of severe hypertension in association with severe headache, nausea, and vomiting, visual disturbances, convulsions, altered mental status and, in advanced cases, stupor and coma.
The key is the presence of severe hypertension. Remember, though, that 160/105 mm Hg may be high for an individual patient. Most patients with the syndrome will have diastolic pressures well in excess of 120-130 mm Hg. The only way you will know if the diagnosis is correct is to treat the BP (carefully control), work up other etiologies, and see of symptoms improve with BP control.
Beware the patient with severe HTN and seizure. Seizure may be the first, and only, symptom of hypertensive encephalopathy.
Some confusion exists regarding proper distinction and treatment between the different tachydysrhythmias associated with WPW. Here's the scoop:
1. orthodromic SVT: narrow regular tachycardia, looks just like a routine SVT, treat just like any other SVT (AV nodal blockers work fine)
2. antidromic SVT: wide regular tachycardia, looks just like VTach, treat like VTach (amiodarone, procainamide, shock; lidocaine won't work, though won't harm either)
3. atrial fibrillation: very different!! irregularly irregular, morphologies of the QRS complexes vary between narrow and wide, some areas may have rates as high as 250-300/min, MUST avoid all AV nodal blockers (which includes adenosine, CCBs, BBs, digoxin, amiodarone); treat with procainamide or sedation+cardioversion
Adhesive Capsulitis -- Frozen Shoulder
In a previous pearl we were discussing the need to perform EGD for any suicidal patient with a history of ingestion of a caustic to grade injury and assess chance of perforation and/or stricture formation. Suicidal patients are intentionally ingesting the caustic and can thus justify the risk/benefit ratio more easily than the pediatric unintentional ingestion. The concerned parent will bring the child in with a possible ingestion of a caustic. The container could be simply in the same room, spilled on the child and never be ingested. Even if ingested, the amount is less if the child tastes the caustic and will reflexively cause spitting. The literature is scant in regards to this type of patient but seems to point to this general algorithm:
Child displays 2 or more of the following symptoms there is enough evidence from case series that there will be a clinically signficant lesion found on EGD.
Vomiting, Drooling, Stridor, Presence of Oropharyngeal Burns
That being said, many clinicians would elect for EGD and assessment of airway with stridor alone. Do not be fooled into thinking if you see no oral lesions that there is no way the child ingested the caustic. Each case series showed a lack of correlation of physical exam findings to EGD findings.
-- ulnar nerve >>> supplies palmar surface and dorsal tips of little finger and medial half of ring finger, including
adjacent parts of hand.
-- median nerve >>> supplies palmar and dorsal aspects of thumb, index finger, middle finger, and lateral half
of ring finger, including adjacent parts of hand.
-- radial nerve >>> supplies most of dorsal surface of hand.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}