Category: Toxicology
Keywords: holly, berry, poinsettia, mistletoe, berries (PubMed Search)
Posted: 12/2/2010 by Ellen Lemkin, MD, PharmD
Click here to contact Ellen Lemkin, MD, PharmD
Toxic Holiday Plants
Of the three plants listed, which is NOT poisonous?
1. Holly plant
2. Poinsettia
3. Mistletoe
Poinsettia plants were once thought to be very poisonous. Contrary to popular belief, poinsettias are safe to have in the home during the holidays.
Although there are reported cases of death with ingestion of Holly plants in older literature, recent experience shows gastrointestinal effects in small doses, and serious toxicity such as CNS depression in large ingestions.
Mistletoe ingestion of few of the berries would, at most, produce mild gastroenteritis; however, ingesting concentrated extracts of the plant, including the berries, may produce serious effects such as seizures, mental confusion, drowsiness, and hallucinations.
Happy holidays!
Poisondex.
Category: Neurology
Keywords: MS, multiple sclerosis, oligoclonal banding, brain MRI, ovoid plaques (PubMed Search)
Posted: 12/1/2010 by Aisha Liferidge, MD
(Updated: 6/24/2026)
Click here to contact Aisha Liferidge, MD
Category: Critical Care
Posted: 11/30/2010 by Mike Winters, MBA, MD
(Updated: 6/24/2026)
Click here to contact Mike Winters, MBA, MD
Beware Trendelenburg Positioning in the Critically Ill Obese Patient
Rahman O, Willis L. Vascular procedures in the critically ill obese patient. Crit Care Clin 2010;26:647-60.
Category: Cardiology
Keywords: pregnancy, cardiac arrest, compressions (PubMed Search)
Posted: 11/28/2010 by Amal Mattu, MD
(Updated: 6/24/2026)
Click here to contact Amal Mattu, MD
In the second half of pregancy, we've traditionally learned that the gravid uterus compresses the inferior vena cava and therefore decreases cardiac output when patient is in a supine position. Therefore, we've learned that patients in the second half of pregnancy the patient should be placed in a left lateral tilt position.
However, it is difficult to perform good quality chest compressions when the patient is in a titled position.
Therefore, the optimal position for chest compressions on the patient in cardiac arrest in the second half of pregnancy is to have the patient in a supine position; and have another rescuer manually deflect the uterus to the patient's left side. This provides optimal compressions + optimal venous return.
Category: Orthopedics
Keywords: Bursitis, heel pain (PubMed Search)
Posted: 11/27/2010 by Brian Corwell, MD
(Updated: 6/24/2026)
Click here to contact Brian Corwell, MD
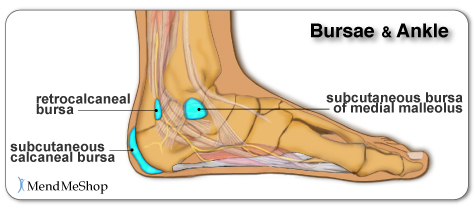
Chief complaint: “Posterior heel pain”
http://www.aidmybursa.com/_img/ankle-retrocalcaneal-subcutaneous-bursitis.jpg
Retrocalcaneal bursitis
The retrocalcaneal bursa is located between the Achilles tendon and the posterior superior border of the calcaneus.
H&P: Inflammation and pain may follow repetitive dorsi/plantar flexion of the ankle (excessive running, jumping activities). Tenderness anterior and superior to the Achilles insertion on the heel.
Treatment: Minimize weight bearing. ½ inch elevation. NSAIDs.
Posterior calcaneal bursitis
This bursa is subcutaneous, just superficial to the insertion of the Achilles tendon.
H&P: Inflammation and pain may follow irritation from the upper border of the heel counter of a shoe. Posterior heel pain. Tender “bump” (the inflamed and swollen bursa) on the back of the heel.
http://podiatry.files.wordpress.com/2006/12/patient2.jpg
Treatment: Opened-heeled shoes, sandals, or placement of a “U-shaped” pad between the heel and the counter. NSAIDs. Advance to shoes with soft or less convex heel counters.
Category: Pediatrics
Posted: 11/26/2010 by Rose Chasm, MD
(Updated: 6/24/2026)
Click here to contact Rose Chasm, MD
MedStudy Pediatric Board Review
Core Curriculum
Category: Toxicology
Keywords: sleep (PubMed Search)
Posted: 11/25/2010 by Fermin Barrueto
(Updated: 6/24/2026)
Click here to contact Fermin Barrueto
As we eat our turkey today and the myth that we are tired because of the tryptophan content is propagated further - nothing to do with the 2000kcals that we just ate - I would like to share an interesting and controversial study.
Use of stimulants and and sedatives by EM residents. Incidence is as follows:
In a study of 485 residents with 47% response rate:
Prescription Stimulants: 3.1%
Sleep Aids (all): 89%
Use of Nonbenzodiazepines (zolpidem): 14%
Use of Melatonin: 10%
Benzodiazepines: 9%
Difficult job with difficult hours. What is the appropriate medication or is there a medication that truly assists with performance? Are they doing harm to themselves? to patients?
Disrupted circadian rhythm, addiction tendencies and the hardship of a stressful nightshifts are the price we pay for this specialty. Awareness and education are needed for the residents as well as the attendings.
Shy BD, Portelli I, Nelson LS. Emergency Medicien residents use of psychostimulants and sedative to aid in shift work and circadian transitions. Am J Emerg Med 2010.
Category: Neurology
Keywords: vertigo, cerebellar stroke, stroke, dizziness (PubMed Search)
Posted: 11/24/2010 by Aisha Liferidge, MD
(Updated: 6/24/2026)
Click here to contact Aisha Liferidge, MD
Category: Critical Care
Keywords: Status epilepticus, non-convulsive, altered mental status, seizure, critical care, ICU, neurology (PubMed Search)
Posted: 11/23/2010 by Haney Mallemat, MD
Click here to contact Haney Mallemat, MD
Non-Convulsive Status Epilepticus (NCSE) is generally under reported. An ICU study found 10% admissions for altered mental status (AMS) were eventually diagnosed as NCSE.
Pearls:
- Include NCSE in the AMS differential
- NCSE may occur with or without convulsive seizures
- Difficult to distinguish from a post-ictal state (14% of convulsive seizures convert to
NCSE)
- Reported mortality is up to 44%
Consider NCSE when:
- Seizure history / recent seizures
- Post-ictal period >1 hour
- Odd behaviors (e.g., chewing, blinking, personality change) and abnormal eye
movements (86% specific)
- AMS without structural, metabolic or traumatic etiology
- Patient intubated for status epilepticus
If you are unsure but suspicious of NCSE order a STAT EEG. Treat NCSE like a convulsive status.
Slattery, D. Seizures as a cause of altered mental status. Emerg Med Clin North Am. 2010 Aug;28(3):517-34.
Category: Cardiology
Keywords: bradycardia, bradydysrhythmia, atropine, transplant (PubMed Search)
Posted: 11/21/2010 by Amal Mattu, MD
Click here to contact Amal Mattu, MD
We mentioned atropine's elimination from the cardiac arrest (asystole, PEA) protocols last week. Atropine (0.5 mg) is still indicated in unstable bradycardias that appear to be vagally-mediated, such as sinus bradycardia and Mobitz I bradycardia.
Beware, however, that atropine is not recommended in patients with transplanted hearts. These hearts lack vagal innervation, and in fact there's one small study suggesting that atropine may be associated with paradoxical slowing of the heart rate and worsening AV block. Go straight to pacing with these patients.
Neumar RW, Otto CW, Link MS, et al. Part 8: Adult Advanced Cardiovascular Life Support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010;122:S729-S767.
Category: Orthopedics
Keywords: Methylene Blue, Intra-articular, Joint (PubMed Search)
Posted: 11/21/2010 by Michael Bond, MD
Click here to contact Michael Bond, MD
Evaluation of Potential Intra-Articular Joint Lacerations
Skin and soft tissue injuries in proximity to a joint often prompt concern of whether the injury violated the joint space. Joint Space involvement is important to exclude as it can lead to septic joints and long term disability.
One easy way to determine if the joint capsule has been violated is to inject methylene blue into the joint and watch to see if any of the methylene blue extravasates through the soft tissue.
Indications for a methylene blue injection include:
There are no absolute contraindications. Though clearly the procedure does not need to be done when the injury highly suggests an open joint injury and the patient will require operative debridement and exploration.
To watch a video of a injection head to eMedicine by clicking http://emedicine.medscape.com/article/114453-overview
Shlamovitz, Gil. Injection, Intra-Articular Methylene Blue. eMedince, Accessed November 2010. http://emedicine.medscape.com/article/114453-overview
Category: Toxicology
Keywords: anticholinergic, physostigmine (PubMed Search)
Posted: 11/18/2010 by Fermin Barrueto
(Updated: 6/24/2026)
Click here to contact Fermin Barrueto
In the setting of a patient suffering from an anticholinergic overdose with hallucinations/agitation, it may be beneficial to administer the antidote: Physostigmine. Many hesitate simply because they have never administered before or there may be doubt in the diagnosis. Here is the skinny:
1) Anticholinergic OD seen in following meds: diphenhydramine (Benadryl), dimenhydrinate (Dramamine), scopolamine, benztropine (Cogentin), some plants like datura stromonium (thorn apple)
2) Physostigmine 1mg IV slowly over a REAL 5 min. Administer to fast and patient may seize. Maximum dose of 2mg IV.
3) Contraindications: suspicion of TCA OD (anectdotal and from old case report) - screening EKG should be done prior to administration of physostigmine. Also glaucoma, closed angle, obstructive uropathy.
Remember your clinical endpoint needs to be measurable, thus hallucinations and agitation should be reversed. No indication if the patient is only experiencing dry mouth or other more mild anticholinergic symptoms.
Category: Neurology
Keywords: pseudotumor cerebri, idiopathic intracranial hypertension, headache, lumbar puncture (PubMed Search)
Posted: 11/17/2010 by Aisha Liferidge, MD
Click here to contact Aisha Liferidge, MD
-- CSF reforms within 6 hours, making its removal short-term, unless there is a CSF leak.
-- LP can be challenging in obese patients and uncomfortable for patients, in general.
-- LP complications such as low pressure headaches, CSF leak, CSF infection, and intraspinal epidermoid tumors.
Category: Critical Care
Posted: 11/16/2010 by Mike Winters, MBA, MD
Click here to contact Mike Winters, MBA, MD
Positioning for Ventilated, Critically Ill Obese Patients
Ashburn DD, DeAntonio A, Reed MJ. Pulmonary system and obesity. Crit Care Clin 2010; 26:597-602
Category: Misc
Keywords: Epinephrine (PubMed Search)
Posted: 11/15/2010 by Rob Rogers, MD
(Updated: 6/24/2026)
Click here to contact Rob Rogers, MD
Dose of Epinephrine for Patients with Anaphylaxis
Many of us are familiar with 0.3-0.5 mg IM of 1:1,000. Important to give IM and not SC.
In severe cases, consider IV Epinephrine:
Corey Slovis, Vanderbilt University
Hans House, University of Iowa Emergency Medicine Residency,
USC Essentials Course 2010 (Mel Herbert and USC Faculty)
Category: Cardiology
Keywords: atropine, cardiac arrest (PubMed Search)
Posted: 11/14/2010 by Amal Mattu, MD
Click here to contact Amal Mattu, MD
The new 2010 AHA Guidelines no longer recommend the use of atropine in caring for patients with cardiac arrest. While it may be useful in vagally-mediated bradycardias, the evidence does NOT support the use of atropine in patients with asystole or PEA; therefore, it has been removed from the cardiac arrest algorithm.
Category: Orthopedics
Keywords: Transverse Myelitis, spinal cord, MS (PubMed Search)
Posted: 11/13/2010 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Transverse Myelitis
A group of inflammatory disorders characterized by acute or subacute motor weakness, sensory abnormalities and autonomic (bowel, bladder, sexual) cord dysfunction.
Symptoms are usually bilateral but both unilateral and asymmetric presentations can occur.
Look for a well-defined truncal sensory level
-below which sensation of pain and temperature is altered or lost.
Causes: Autoimmune after infection or vaccination (60% of cases in children), direct infection, or a demyelinating disease such as MS. No cause is found in 15 – 30% of cases.
Incidence: Bimodal peak at 10-19 years and at 30-39 years.
Diagnostic testing: MRI of the ENTIRE spine to both rule out structural lesions and rule in an intrinsic cord lesion. If MRI is normal reconsider the original diagnosis.
Treatment: Steroids are first-line therapy. Dosing is controversial but generally involves high IV doses for 3-5 days (1000 mg methylprednisolone). Plasma exchange is second line for those who don’t respond to steroids.
Transverse Myelitis. Frohman EM, Wingerchuk DM. NEJM 2010 Aug 5;363(6):564-72.
Category: Toxicology
Keywords: hydrogen peroxide, embolism, hyperbaric (PubMed Search)
Posted: 11/11/2010 by Bryan Hayes, PharmD
(Updated: 6/24/2026)
Click here to contact Bryan Hayes, PharmD
French LK, et al. Hydrogen peroxide ingestion associated with portal venous gas and treatment with hyperbaric oxygen: a case series and review of the literature. Clinical Toxicology 2010;48:533–38.
French LK, et al. Hydrogen peroxide ingestion associated with portal venous gas and treatment with hyperbaric oxygen: a case series and review of the literature. Clinical Toxicology 2010;48:533–38.
Category: Neurology
Keywords: movement disorders, chorea, athetosis, fasiculations, dystonia (PubMed Search)
Posted: 11/10/2010 by Aisha Liferidge, MD
(Updated: 6/24/2026)
Click here to contact Aisha Liferidge, MD
Category: Critical Care
Keywords: ultrasound, ocular, sonography, intracranial pressure, optic nerve sheath, ICP (PubMed Search)
Posted: 11/9/2010 by Haney Mallemat, MD
Click here to contact Haney Mallemat, MD
Ocular sonography is a fast, simple, and non-invasive tool to detect elevated intracranial pressure (ICP) by measuring the optic nerve sheath diameter (ONSD). Several studies have shown a positive correlation between increased ONSD (>5.7mm) and elevated ICP (>20mmHg). Although ultrasound may not replace CT or MRI to diagnose the cause of the increased ICP, its use as a triage tool can expedite these tests.
The technique:
Please see the references below for more information and, as with any new technique please consult local experts prior to making clinical decisions.
http://www.sonoguide.com/smparts_ocular.html
Soldatos, T. et al. Optic nerve sonography in the diagnostic evaluation of adult brain injury. Crit Care. 2008; 12(3): R67. Epub 2008 May 13.
{kind=link}
{kind=link}